In this blog post, we will discuss a concept called “the envelope of function” and how it can help you and your patient to make sense of the role of load & overload in pathology and pain.
Envelope of Function – Definition
Effective treatment for any orthopedic condition is an accurate understanding of the etiology of the symptoms. With the structural and biomechanical explanation for pain giving way to the biopsychosocial model, it becomes increasingly evident that a crucial factor for possible pathology and pain is often simple overload.
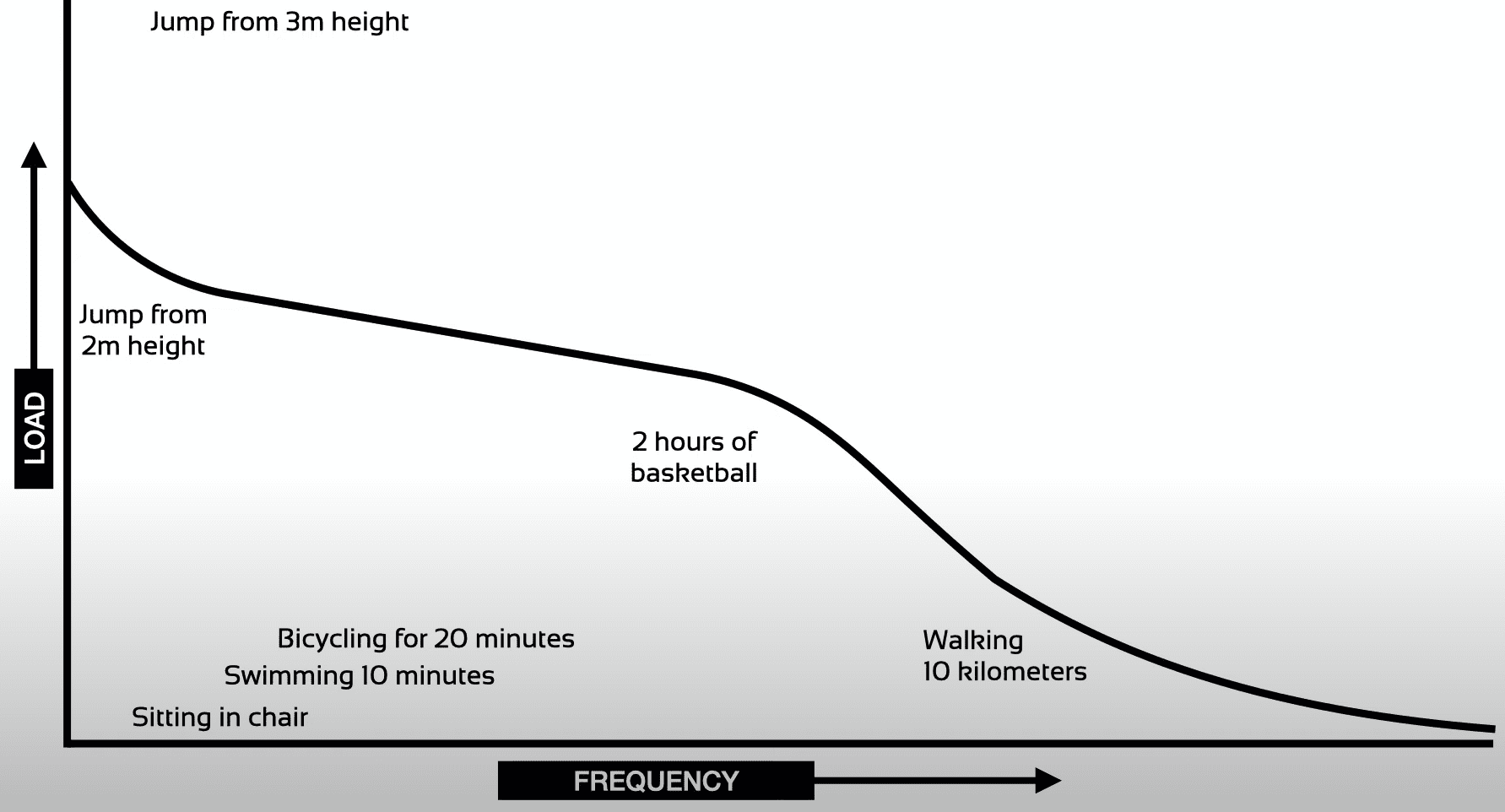
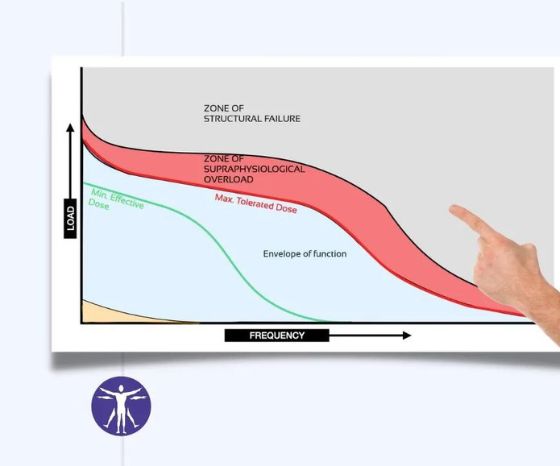
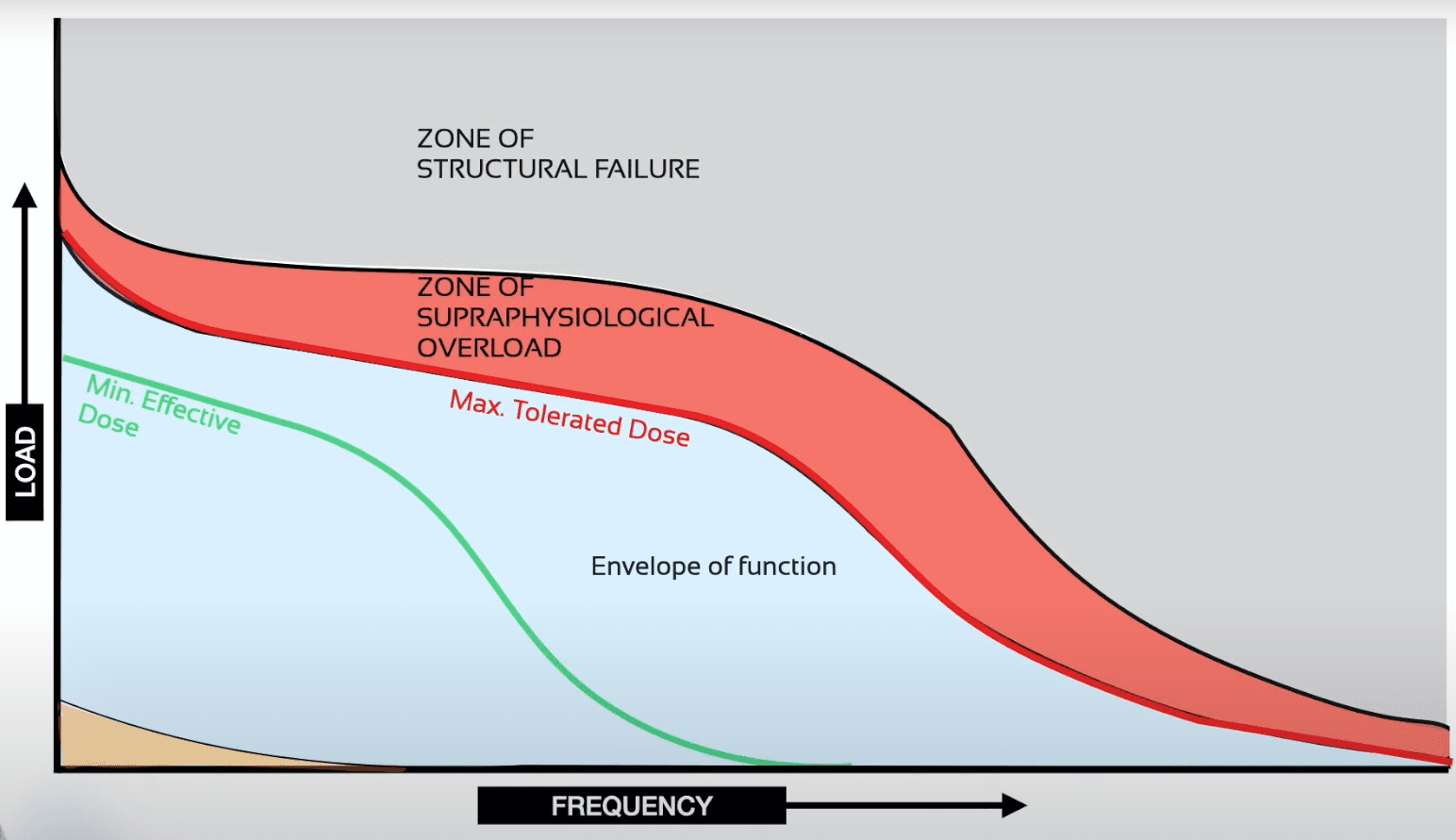
The concept of the envelope of function was proposed by orthopedic surgeon Scoot Dye (2005) who used it in order to explain the symptomatic loss of tissue homeostasis in Patellofemoral pain. The envelope of function is depicted by the black line and displays what an individuum is conditioned to tolerate in terms of load (seen on the y-axis) and frequency (seen on the x-axis) without losing tissue homeostasis. Be aware that this is only an example and not actual data. What it shows is that higher loads like a jump from 2 meters height will be tolerated at low frequencies. On the other hand, higher frequency activities will be tolerated better at lower loads such as walking 10 kilometers. All other activities like 10 minutes of swimming or cycling for 20 minutes are well tolerated because they fall within the envelope of function. Activities that fall outside of the envelope of function, such as a jump from 3 meters height fall outside of the envelope of function and will disrupt tissue homeostasis. We have to be careful when we are talking about load as if this is only a mechanical factor. According to the biopsychosocial modal, load can also include psychosocial factors such as fear, lack of sleep, etc.
Zones in the Envelope of Function
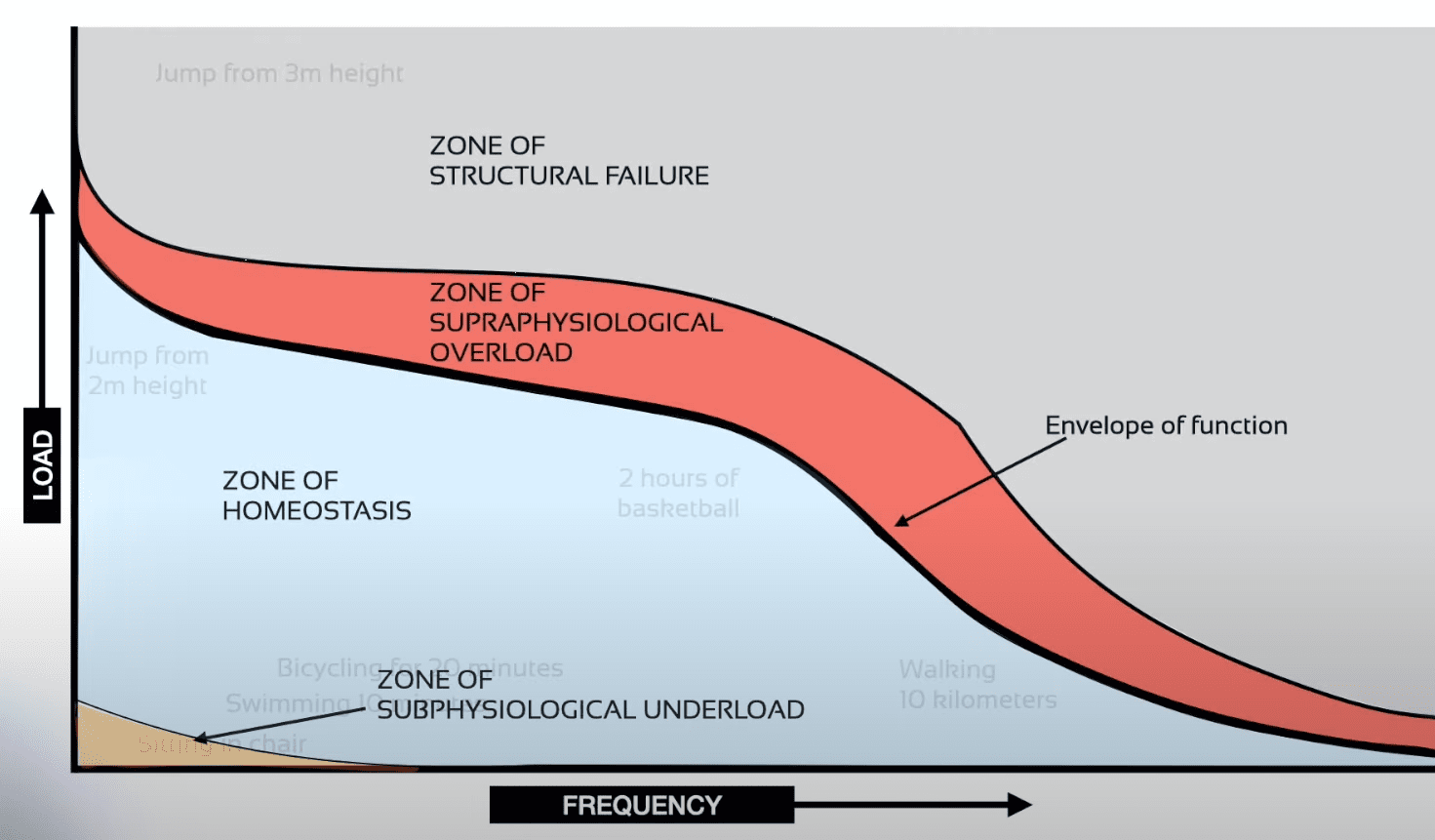
Now if you only perform activities in the bottom left with low load and low frequency you will experience deconditioning. Above the envelope of function, Scott Dye added 2 layers: The zone of supraphysiological overload will disrupt homeostasis, but it will not instantly cause structural failure. He argues that prolonged overload in this zone might eventually lead to structural failure.
The layer on top of the supraphysiological overload is the zone of structural failure. In the example, this would be a jump from 3 meters height which might lead to bone fracture. On the other end of the spectrum, this might be a very high frequency without adequate rest for recovery.
Orthopedic Physiotherapy of the Upper & Lower Extremities
Boost Your Knowledge about the 23 Most Common Orthopedic Pathologies in Just 40 Hours Without Spending A Fortune on CPD Courses
Establishing a Patient’s Tolerable Dose
Every time, you see a new patient in practice, start with evaluating the individual’s current abilities and where they have to go on this graph in order to reach their goal. As a second step, you will have to determine what their minimum/maximum tolerated dosage is. This defines the amount of stress necessary to create physiological & biological adaptations. A dosage below the minimal effective dose isn’t going to create these adaptations. That’s okay if your goal is to work on something like tolerance via graded exposure, skills, etc. A quick shout-out at this point to Scott Morrison from physio_praxis who explained this subject very well on his Instagram handle.
Obviously, every person’s conditioning is different, so with each and every person, and probably even if you compare your left to your right knee, the curve will be different. In the following example, the person seems to be conditioned to play 2 hours of basketball, but for another person, this will overload the person’s knee, disrupt tissue homeostasis and possibly lead to pain.
Patellofemoral Pain – An Example of the Drop of the Envelope of Function due to Overload
Let’s look at Dye’s example of a person before and after they experience patellofemoral pain:
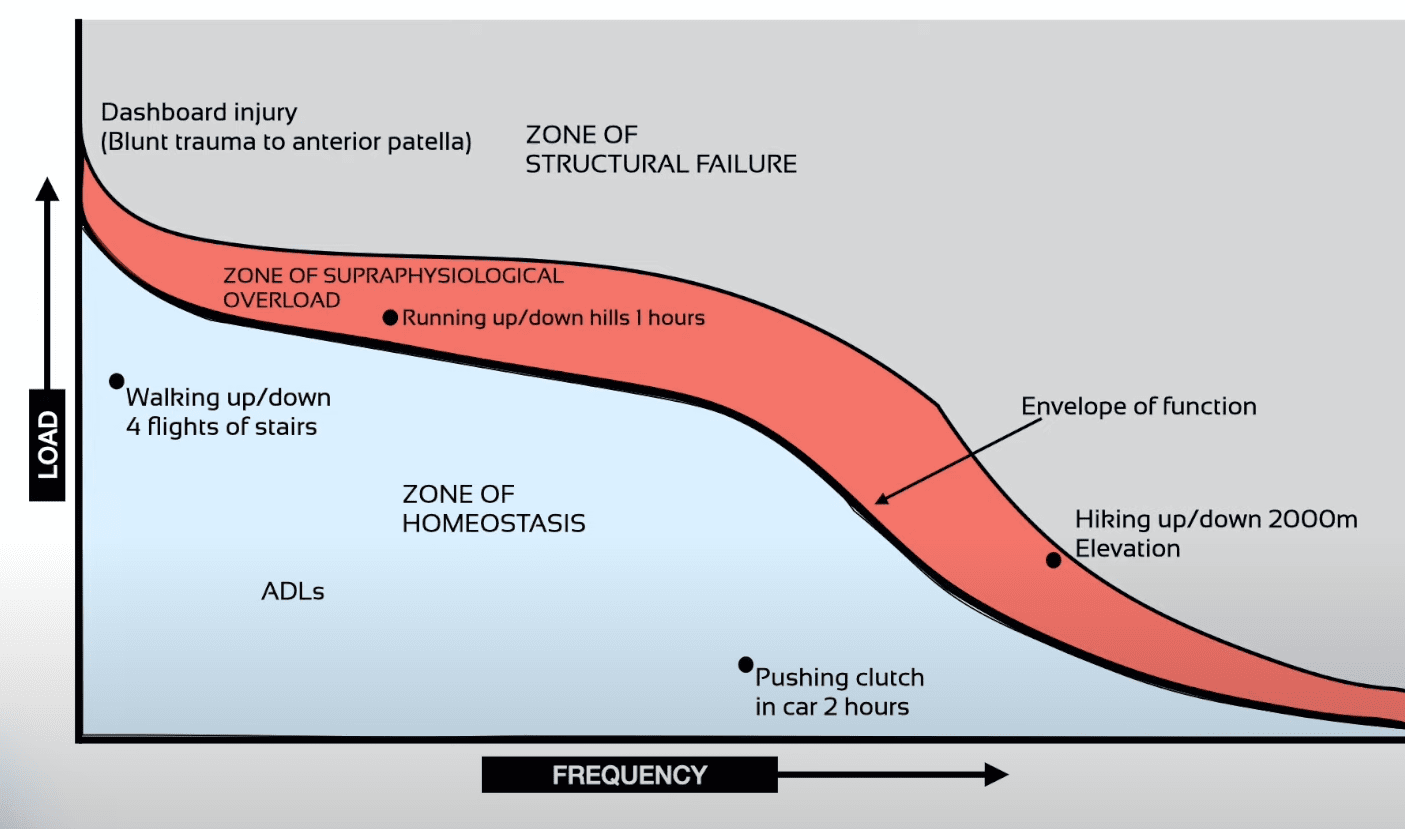
Here we can see that walking up and down the stairs, ADLs, and pushing the clutch in the car is well tolerated by this person. If this person starts hill running for 1 hour or hikes up and down 2000 meters of elevation they might irritate their knees without any evidence of structural failure.
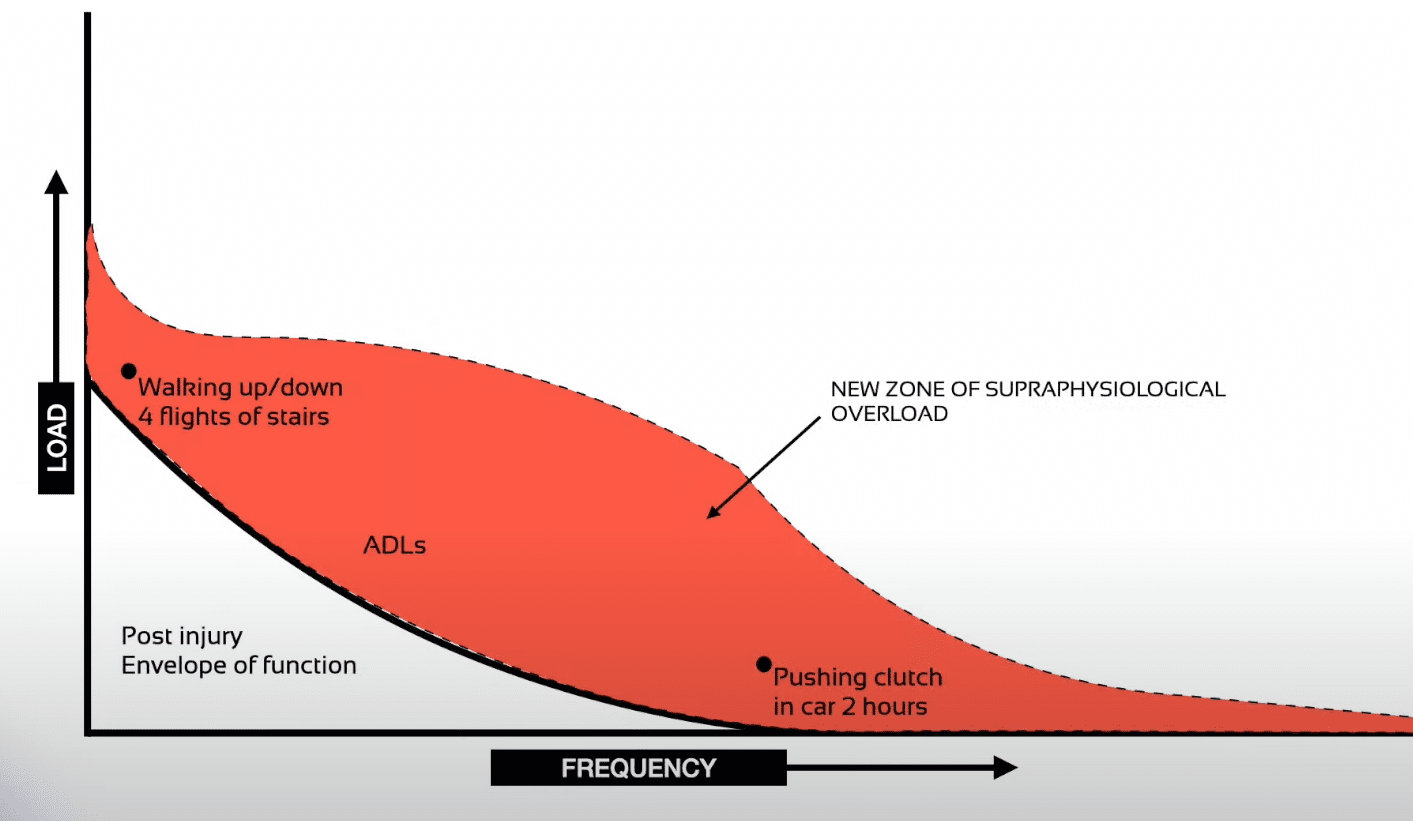
Once your knee is irritable it is going to drop the envelope of function. So suddenly, activities that were once tolerated well are now also irritating the knee: walking the stairs, ADLs, or pushing the clutch now fall outside the envelope of function as well and are not tolerated anymore. Notice that not the activity has changed, but the tolerance. We cannot change the activity or how they walk the stairs. So how do we solve this?
Increasing the Envelope of Function
First of all, we want to stop performing activities that are within the zone of supraphysiological overload temporarily to calm down the knee. There are a couple of modalities that can help that process further such as patellar taping for example.
Second of all, we want to prevent the envelope of function to decrease further. That’s why complete rest is often a recipe for disaster and we need to encourage this patient to keep doing activities that are still within his envelope of function.
As a third step, we want to keep pushing the envelope of function to the top right again. Performing activities that are already well tolerated is not going to lead to change. That would be like lying on the couch and expecting your muscles to grow. To achieve this goal we need to train in a zone above the minimum effective dose and below the maximally tolerated dose.
Complete rest is often a recipe for disaster as it will drop the envelope of function further
Finding the Right Dosage – The 24-Hour Rule
How do we know our dose is right? As a rule of thumb, tolerable pain during exercise is acceptable as long as it settles within 24 hours after the training. There are 2 things I would like to add that are very important:
First of all, we saw that the curve of the envelope of function is very specific. So if our patient wants to get back to playing basketball for 2 hours, what should he do? Obviously, he should play basketball to condition himself to tolerate 2 hours of basketball. Instead of completely avoiding an aggravating activity it often makes sense to reduce the volume of this activity, so you might get him started to play for 10 minutes.
The envelope of functio is specific. Gradually expose a patient to what he want to get back to.
The second thing that is important is not to stop with the training as soon as the patient can just tolerate the task he wants to get back to. You always want to push the envelope of function a bit further to make him resilient more resilient and to prevent fallbacks. This way, the knee won’t act up when he plays a bit longer, on a different court, or if he lacked sleep the night before.
Alright, this was our blog post on the envelope of function to understand load and overload. If you like learning about basic principles of physiotherapy, check out the following resources:
- 5 Reasons Your Therapy Sucks
- Orthopedic Special Tests are not so special
- Exercise prescription – Going Beyond 3×10
As always, thanks a lot for reading!
Kai
References






