
Next to our ability to listen, validating concerns, and provide education to our patients, exercise prescription is one of our best interventions to help people with a physical complaint. However, effective implementation in practice is unsatisfactory.
We have already discussed that many health professionals are not up to date on recommended physical activity guidelines and surveys on senior physiotherapists revealed that a majority of physios appear to have limited knowledge on exercise program design for optimal results. Hence why you hear 3×10, 3 times a week across gyms and clinics all around the world. It has become the default dose when prescribing exercises.
3×10 is better than 0x0 but specificity matters in exercise prescription to achieve optimal outcomes
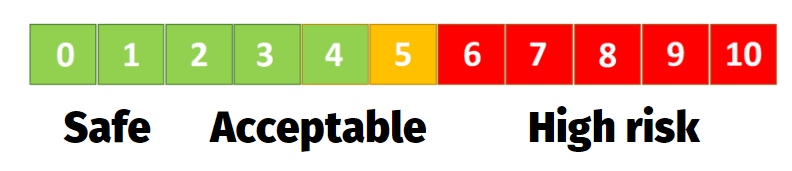
Sure, 3×10 is better than 0x0 but specificity matters in exercise prescription to achieve optimal outcomes. As a sidenote, we will disregard “pain reduction” as the outcome for this blog, as dosage for pain relief is still not that clear and many more factors are associated with pain relief than simply complying with strength training guidelines. As a rule of thumb for training with pain, we employ a simple traffic light system. Is pain high, say a 7/10, we want to decrease the intensity to for example 3/10. Are pain levels low, we can increase the intensity.
But some patients may not even need a tailored exercise program at all but for this article we want to showcase how to make exercise prescription specific to your goals: whether that’s to improve strength, power, hypertrophy or muscular endurance. I assume that you have heard of: 1-5 reps are needed to build strength, 6-12 to build hypertrophy and anything beyond 12 reps is meant to build muscular endurance.
HOW TO REHAB HAMSTRING, CALF & QUADRICEPS MUSCLE- & TENDON INJURIES
However, it is not that simple. And research has actually shown that when we for example look at maximizing hypertrophy, the total volume of training is more important than adhering to a specific repetition range. But what’s most crucial and what is missing in the 3×10 3 days a week programming is “intensity”. Because even when low intensity training is performed until failure, that is at an intensity of 30% of ones 1RM, it does not result in the same degree of muscle activation that occurs at moderate or high intensities even when volume is matched. In rehab, I’d say many tend to shy away from prescribing higher intensity exercise to patients. This may be due to fear of injury, not only from the patient’s side but also from a belief the therapist may hold. Or simply because they don’t know how to do it. But that would be like a doctor prescribing medicine without providing details on dosage. From personal experience, we’ve heard many stories of patients with a musculoskeletal problem who have had unsatisfactory results in the past that could (partially) be explained due to chronic underloading. Our bodies, tissues but also mind adapt to the stresses they are exposed to. If we want to instill robustness and resilience in our patients, we need appropriate intensity. There are several ways we can gauge intensity, whether that’s maximal or submaximal RM testing using the Holten Diagram, ratings of perceived exertion (RPE) during or after an exercise, such as the BORG scale for aerobic exercise, or a more novel approach using Repetitions in reserve aka RIR.
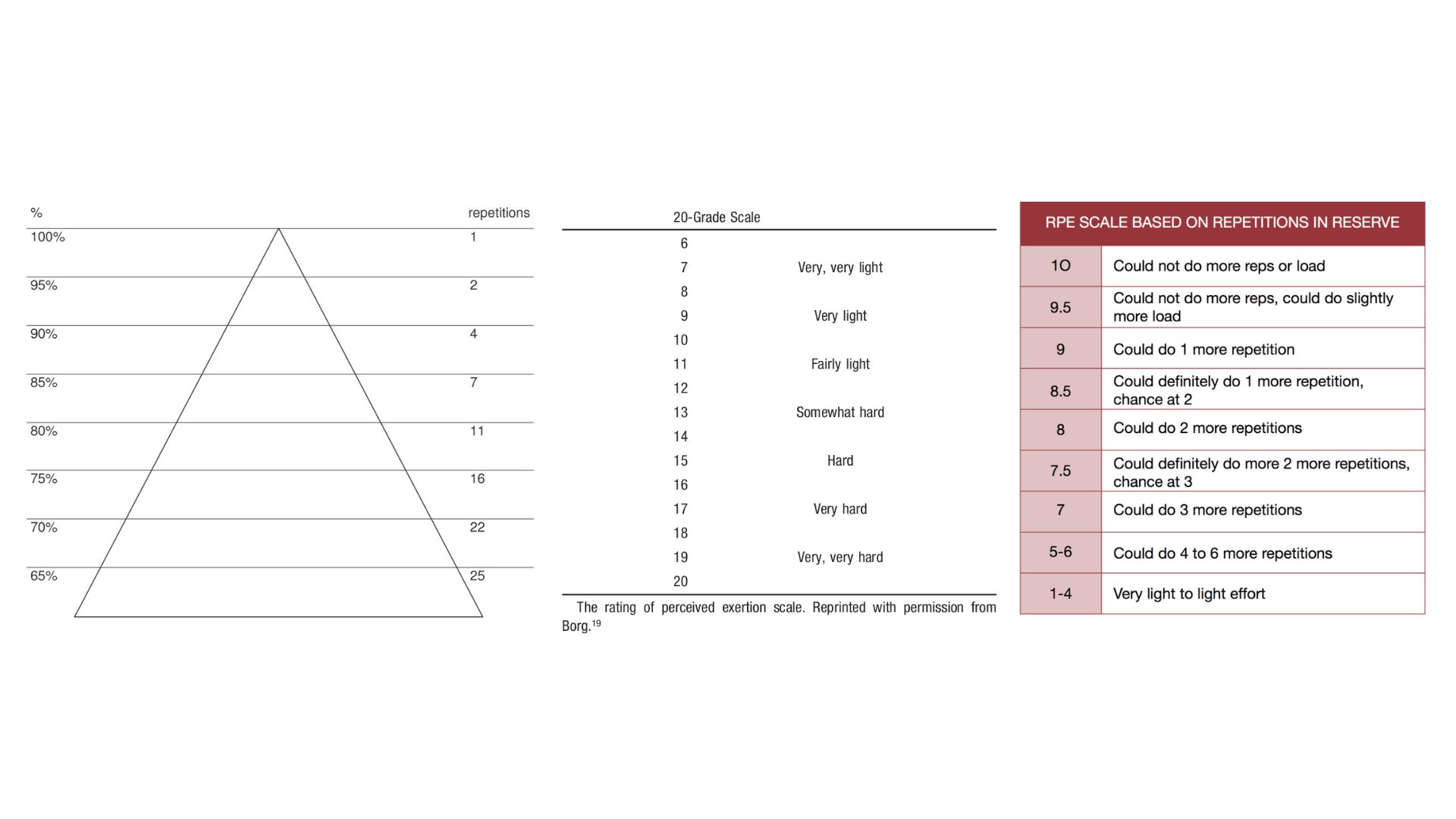
The latter may be a bit more difficult to employ as it requires experience with the particular exercise to accurately estimate repetitions in reserve. In a rehab setting we often have someone do a test set of a given exercise and ask them to stop when they feel they have 2-3 reps left in the tank. Then we ask them to keep going to show them how accurate or not they were with their estimation on how close they were to failure. In practice we prefer to use RPE or RIR over a percentage of one’s 1RM as sticking to a set percentage can vary on a day-to-day basis. So 75% of your 1RM may feel light on a day one is well rested, has little discomfort but on another day where one is stressed, under slept and feels more discomfort can feel closer to 90% than 75. RPE or RIR allows us to modulate the intensity on a day-to-day basis or even between sets and stay flexible with the weights in either direction (up or down) while focusing on creating the right stimulus.
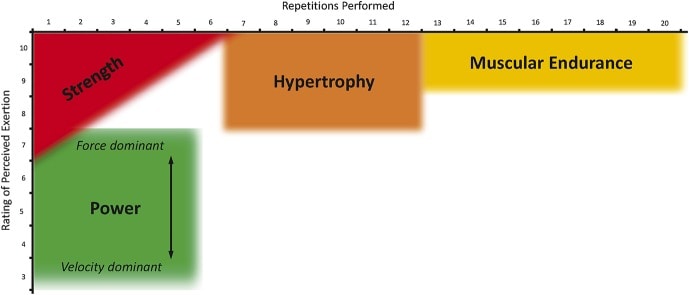
But let’s look at what is regarded as appropriate intensity with regards to training goals such as strength, hypertrophy, or muscular endurance.
Exercise prescription for Muscular Hypertrophy
A previously mentioned, recent research into what makes a muscle grow has revealed that the total volume of training is more important than adhering to a specific rep range of say 6-12 reps as is still believed by many. Loads that are heavy enough and performed with an adequately high volume will build muscle. Whether that’s a heavy 3 repetition maximum or moderate 10 RM doesn’t seem to matter as far as hypertrophy is concerned. But there are a few things to consider. One is time. High repetition training takes less time than volume-matched sets with very heavy loads. And the other is the nature of the exercise. Doing high repetition exercises closer to failure can be fine for exercises with a low biomechanical complexity and risk of injury (such as bicep curls or other isolation exercises) whereas doing the same with deadlifts or back squats can be soul crushing. So, for hypertrophy we’d use and RIR based RPE of 8-10 (so 0-2 reps left in the tank) in a rep range between 6-12 for isolation exercises and for compound lifts such as the squat or bench-press we tend to stay in the RPE range of 6-8 (or 2-4 RIR).
High repetition training takes less time than volume-matched sets with very heavy loads.
Exercise prescription for Strength
Strength, or maximal strength, in itself would mean that we should approach an RPE of 10 or 0RIR. However, this is not necessarily desirable or could be detrimental in the rehab setting. Training to failure regularly can hamper gains in strength compared to performing only a moderate amount of volume in this range. Generally accepted are 80-100% of 1RM, which translates to intensities in the 1-6RM range or 6 reps with 0 RIR, 5 reps with 1RIR, 4 reps with 2 RIR or 3 reps with 3 RIR.
Exercise prescription for Endurance
Let’s look at muscular endurance, which is fairly similar in principle to hypertrophy training but with a focus on developing fatigue resistance. So rest periods are shorter to stimulate faster interest recovery and training to failure with moderate loads is desired. So we aim for sets of more than 12 reps with and RPE 9-10 or 0-1 RIR.
It has to be said that these principles have been studied in healthy novice and experienced lifters but we feel confident in applying the same principles in a patient population but adjusting it to the individual in front of us depending how symptoms behave. Because we also need to be specific with our rehab goals. Some patients may need to work more on strength to allow them to better cope with day-to-day tasks when lifting or moving objects at work or at home. For others it’s more about local muscle endurance to cope with static work environments or hypertrophy for those recovering from surgery or immobilization. And then there are all the other mental and physical benefits of exercise I haven’t even talked about.
Thank you for reading
References





