
“Should exercise be painful or not?” This is a popular question among both physiotherapists and patients, which is still a topic of large debate. Indeed, although exercise is a proven effective treatment in chronic rotator cuff-related shoulder pain, the level of pain during exercise is still unclear.
Pain-monitoring model
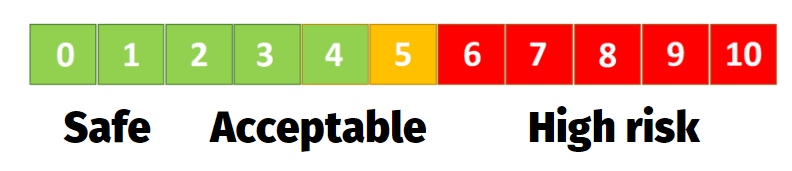
A pain monitoring model is often used during exercise, which describes a scale from 0 to 10, where 0 is indicating “no pain” and 10 indicates “worst imaginable pain” (Thomee et al. 1997). Pain between 0 and 2 is considered “safe”, between 2 and 5 is “acceptable” and above 5 is “high risk”. Moreover, pain is allowed to reach 5 after exercise but it should decrease by the next morning. These are general guidelines that have been applied in clinical practice, studies, and with a variety of indications in shoulder rehabilitation (Holmgren et al. 2012, Maenhout et al. 2012, Valles-Carrascocsa et al. 2018).
What is the current practice among physiotherapists in shoulder rehabilitation?

The lack of clear evidence-based guidelines reflects also on the current clinical practice. Several surveys on the physiotherapeutic management of subacromial shoulder pain have been performed in 4 different countries (United Kingdom, Belgium, The Netherlands, and Italy)(Bury et al. 2018, Pieters et al. 2019, Brindisino et al. 2018) and showed variable results on the instructions about pain during exercise. Most physiotherapists instructed their patients not to have any pain or at least not more than acceptable discomfort. Experts in the field recently suggested using different types of exercises according to symptoms’ acceptability as long as they could sufficiently challenge weakness and train to fatigue (Littlewood et al. 2019).
Hurt ≠ Harm

Physiotherapists usually don’t encourage patients to train in pain. However, there is no strong scientific basis for this fear of “exercising into pain”. Indeed, considering the principle that “hurt does not equal harm, a recent systematic review challenges this belief and suggests that painful exercises are more beneficial in short term compared to pain-free exercise in chronic musculoskeletal pain (Smith et al. 2017). Considering that pain does not always correspond to tissue damage (such as a tear or tendon degeneration), other factors such as fear of movement and central sensitization can play an important role in the development or maintenance of pain. If painful exercises are allowed with suitable “safety cues”, the physiotherapist can gradually reduce the threat perception of the painful movement (Smith et al. 2018). If the shoulder is considered “de-conditioned” and the purpose is to strengthen the shoulder muscles, the patients will re-think and re-modulate under the guidance of the treating physiotherapist.
A recent systematic review suggests that painful exercises are more beneficial in short term compared to pain-free exercise in chronic musculoskeletal pain
No pain, no gain?

We know from the literature that painful exercises usually have higher loads or doses of exercises (sets and repetitions). We also know that higher loads or doses might give superior benefits. So, is a painful exercise program better than pain-free exercises? Will higher loads challenge the patient enough to gain strength and decrease pain? Is it feasible to exercise into pain and if so, which exercises should be prescribed?
ROTATOR CUFF RELATED SHOULDER PAIN: SEPARATING FACTS FROM FICTION
It’s Time to Stop Nonsense Treatments for Shoulder Pain and To Start Delivering Evidence-based Care
We are trying to answer these important clinical questions at the University of Antwerp in Belgium. We already conducted a feasibility study on exercising into the pain in 12 shoulder pain patients with 4 individualized painful exercises (pain ranging between 4 and 7/10 during exercise). Preliminary results showed that most patients were able to train into pain, but for some 9 consecutive weeks was too much. However, overall, increasing loads with a tailored progression improved symptoms and increased functionality. More precise results on this feasibility trial and the large randomized controlled trial will be published soon.
References






