Lumbar Radicular Syndrome | Diagnosis & Treatment for Physiotherapists
Lumbar Radicular Syndrome | Diagnosis & Treatment
Introduction & Epidemiology

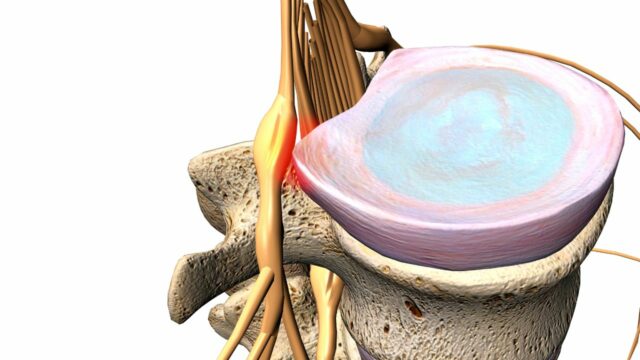
Lumbar radicular syndrome is the umbrella term encompassing radicular pain and/or signs of radiculopathy in the lumbar spine and sacrum. Even though “radicular pain” and “radiculopathy” are synonymously used in the literature, they are not the same. Radicular pain is defined as “pain evoked by ectopic discharges originating from a dorsal root or its ganglion”. Disc herniation (hernia nucleus pulposus, HNP), the most common cause, and inflammation of the affected nerve seem to be the critical pathophysiological process. Radiculopathy is yet another, distinct entity. It is a neurological state in which conduction is blocked along a spinal nerve or its roots (Bogduk et al. 2009). This leads to objective signs of loss of neurologic function such as sensory loss (hypoesthesia or anesthesia), motor loss (paresis or atrophy), or impaired reflexes (hyporeflexia). As disc herniations are by far the most common cause of lumbosacral radicular pain (90%, Koes et al. 2007), let’s have a closer look at facts & fiction around them:
The prevalence of herniated discs is highest on levels L4-L5 and L5-S1 with both 45% of all cases. This is due to the fact that static and kinetic forces are the highest on these two levels. Furthermore, hernias on levels L3-L4 are reported to be less prevalent (5%), followed by an even lower prevalence on levels L2-L3 and L1-L2 (Schaafstra et al. 2015). In case of a disc herniation between L4-L5, the nerve root of L5 will be compressed and in the case of L5-S1, the nerve root of S1 is affected. This is due to the fact that most discus hernias present as mediolateral prolapses:
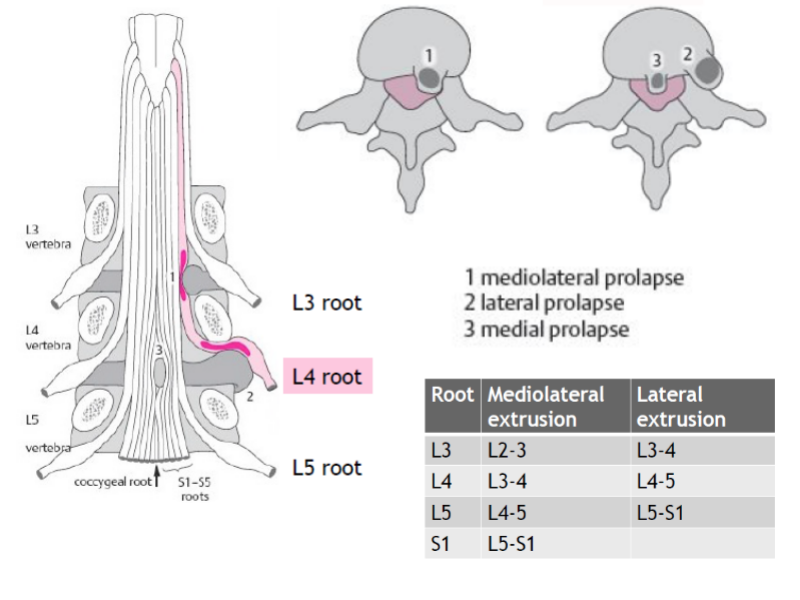 Epstein et al. (2002) have studied lateral disc herniations in detail. According to the authors, far lateral disc herniations represent 7-12% of all lumbar disc herniations and usually involve free fragments which have migrated superolateral to the disc space of origin. A far lateral disc herniation compresses the nerve root which exits at the same level; this is in contrast to classic mediolateral disc compression which affects the nerve root leaving at the level below (see illustration above). Most frequently far lateral disc herniations are encountered at either the L3-L4 or L4-L5 levels followed by L5-S1.
Epstein et al. (2002) have studied lateral disc herniations in detail. According to the authors, far lateral disc herniations represent 7-12% of all lumbar disc herniations and usually involve free fragments which have migrated superolateral to the disc space of origin. A far lateral disc herniation compresses the nerve root which exits at the same level; this is in contrast to classic mediolateral disc compression which affects the nerve root leaving at the level below (see illustration above). Most frequently far lateral disc herniations are encountered at either the L3-L4 or L4-L5 levels followed by L5-S1.Patients with far lateral disc herniations are typically in their mid-fifties, ranging from 50-78 years of age and often report extreme radicular pain associated due to a compromise of the dorsal nerve root ganglion in the lateral compartment. Leg pain is usually unremitting while back pain is often minimal.
Similarly to the cervical spine, a nerve root can also become entrapped between hypertrophied facet joints, a disc protrusion, spondylotic spurring of the vertebral body, or a combination of these factors. In these cases, we are talking about a lateral stenosis, which we will cover in the next unit amongst others. Other less likely reasons for radicular pain can be tumors, synovial cysts, infection, vascular abnormalities, or spinal stenosis, which we will cover in the following unit. You will learn how to recognize some of these red flags in the part on screening.
Clinical Presentation & Examination
Signs & Symptoms
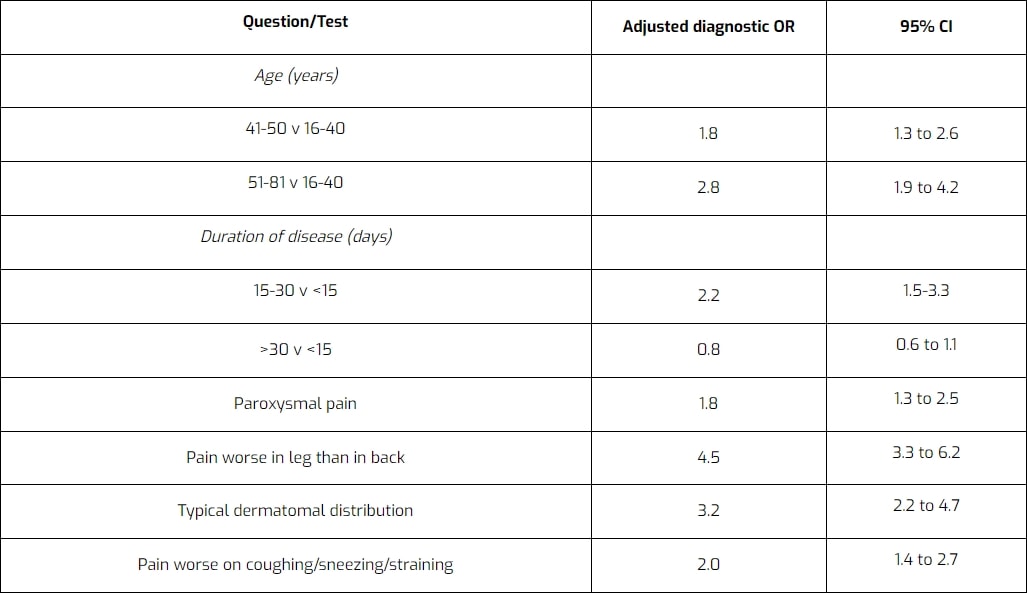
Similar to other pathologies, a thorough patient history can already point you in the right direction when considering the possibility of lumbosacral radicular syndrome. Vroomen et al. (2002) have evaluated different items during patient history regarding their accuracy to diagnose lumbosacral radicular syndrome. They have found the following items to be diagnostic for lumbosacral radicular syndrome due to disc herniation:
Examination
After patient history-taking, you might have formed the ICD (International Classification of Disease) hypothesis that your patient suffers from lumbosacral radicular syndrome. You can then further decrease your clinical uncertainty by performing physical tests to either exclude or confirm the hypotheses. The first test battery is focused on the reproduction or easing of radicular pain and/or paresthesia:
A more specific test to confirm the presence of lumbosacral radicular syndrome is the crossed SLR:
Other orthopedic tests to diagnose lumbar radicular syndrome are:
- Bowstring Test
- Slump Test
- SLR with proximal and distal initiation
- Slump Test with proximal and distal initiation
During the second part of your examination, you should perform a neurological examination focusing on the presence and degree of radiculopathy evaluating hyporeflexia, hypoesthesia, and paresis:
The following video on dermatome testing was derived from the American Spinal Injury Association (ASIA) form:
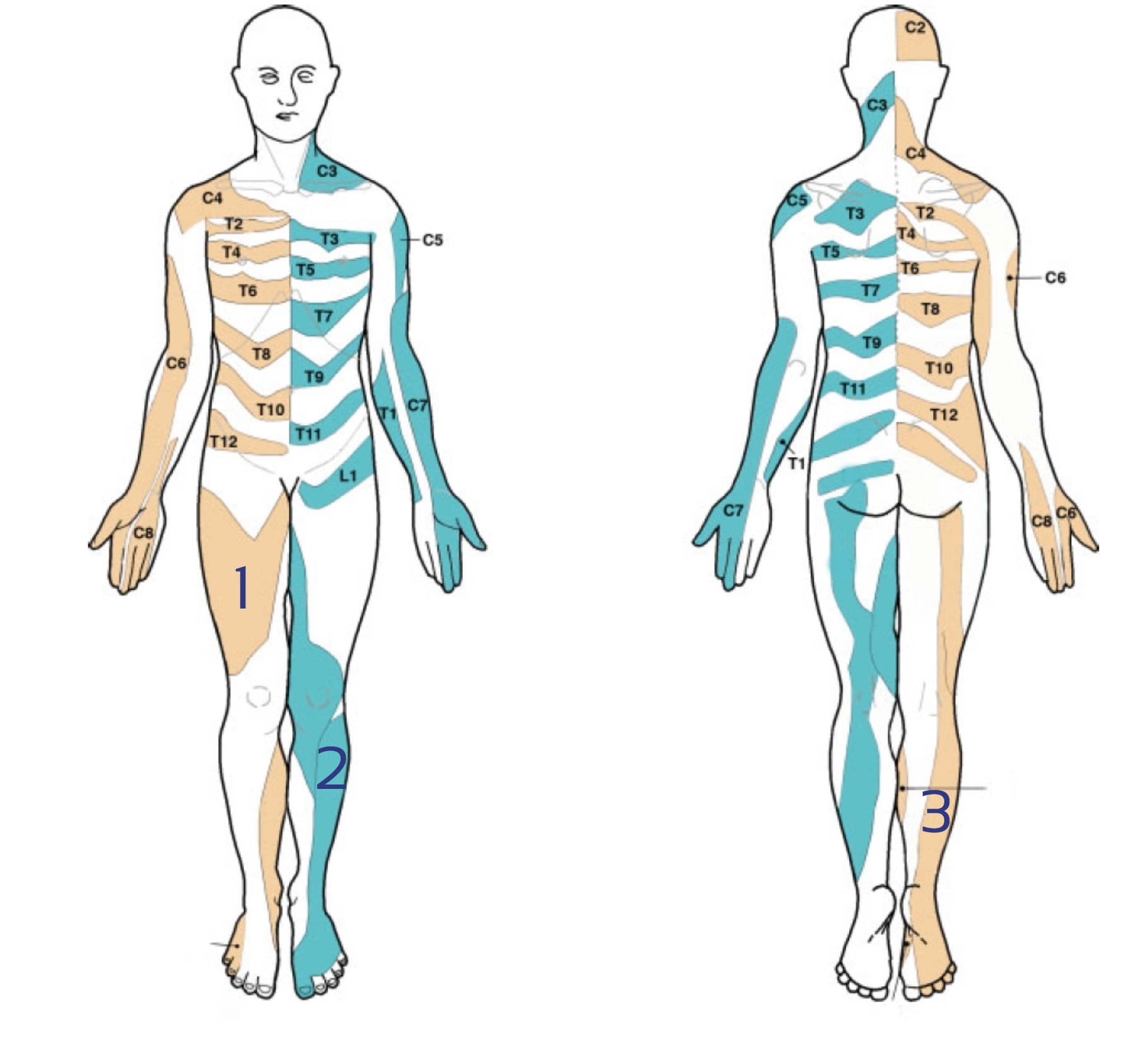
Lee et al. (2008) evaluated the literature and created a composite dermatome map based on published data from 5 papers they considered to be the most experimentally reliable. Their maps look like this:
There is a lot of discussion going on about the reliability of dermatome maps. Check out our blog articles and research reviews if you want to learn more about it:
You can test the lower limb myotomes as explained in the following video:
Be aware, that there can be other underlying reasons for nerve root entrapment than a herniated disk. On top of that, pain radiating to the proximal leg could also be referred pain instead of radicular pain. For more information check out the following videos:
- Lumbar Radicular Pain vs. Referred Pain
- Lumbar Radicular Syndrome vs. Intermittent Neurogenic Claudication from Lumbar Spinal Stenosis
5 ESSENTIAL MOBILIZATION / MANIPULATION TECHNIQUES EVERY PHYSIO SHOULD MASTER