Cervical Radiculopathy | Diagnosis & Treatment for Physiotherapists

Cervical Radiculopathy | Diagnosis & Treatment for Physios
Introduction & Epidemiology

Cervical radicular syndrome is the umbrella term encompassing cervical radicular pain and/or cervical radiculopathy. Even though “radicular pain” and “radiculopathy” are synonymously used in the literature, they are not the same. Radicular pain is defined as “pain evoked by ectopic discharges originating from a dorsal root or its ganglion”. Disc herniation (hernia nucleus pulposus, HNP), the most common cause, and inflammation of the affected nerve seem to be the critical pathophysiological process. Radiculopathy is yet another, distinct entity. It is a neurological state in which conduction is blocked along a spinal nerve or its roots (Bogduk et al. 2009).
This leads to objective signs of loss of neurologic function such as sensory loss (hypoesthesia or anesthesia), motor loss (paresis or atrophy), or impaired reflexes (hyporeflexia).
In the cervical spine, true disc prolapse and herniation of the nucleus pulposus are uncommon. The neural foramen is bordered ventrally by the uncovertebral joint and dorsally by the superior articular process of the caudal vertebrae. Compressive radiculopathies occur as a result of the mechanical distortion of the nerve root either by hypertrophied facet joints or uncovertebral joints, disc protrusion, spondylotic spurring of the vertebral body, or a combination of these factors (Abbed et al. 2007). HNP accounts for about 20%-25% of cervical radiculopathies and degenerative disc disease (DDD) accounts for about 70%-75% (Roth et al. 2009).
A review from Van Zundert et al. (2010) reports an annual incidence of 82,3 new cases of cervical radicular syndrome in 100.000 people, with an adjusted incidence of 107 for males and 64 for females. The study also reports that the most commonly affected nerve root is C7 in 45-60% of all cases, followed by C6 (20-25%) and C5 and C8 with both 10%.
Clinical Presentation & Examination
Signs & Symptoms
The following signs & symptoms can be indicative of neck pain grade III (Bono et al. 2011, Kuijper et al. 2008):
- Pain in the neck is minor compared to arm pain, additionally possible scapular and periscapular pain
- Neck movements and maneuvers increasing intraspinal pressure like coughing
and sneezing worsens pain or tingling in the arm - Varying degrees of paresthesia, sensory loss (hypoesthesia) in the dermatomal region of the affected nerve root
- Identification of a restricted cervical range of motion, defined as rotation less than 60 degrees or limited and painful rotation
- Varying degrees of motor weakness (paresis) in the myotome of the affected nerve root
- Varying degrees of decreased deep tendon reflexes (hyporeflexia) of the corresponding nerve root
- Atypical signs & symptoms include deltoid weakness, scapular winging, weakness of the intrinsic muscles of the hand, chest or deep breast pain, and headaches
Examination
After patient history-taking, you might have formed the ICD (International Classification of Disease) hypothesis that your patient suffers from cervical radicular syndrome. You can then further decrease your clinical uncertainty by performing physical tests to either exclude or confirm the hypotheses. The first test battery is focused on the reproduction or easing of radicular pain and/or paresthesia:
A positive Spurling test is a very specific test that can confirm the diagnosis of cervical radicular syndrome. The test is positive upon reproduction of symptoms like pain and paresthesia in the arm and hand.
Other orthopedic tests to diagnose cervical radicular syndrome are:
- Cluster of Wainner
- Cervical Distraction Test
- Shoulder Abduction Sign
- Valsalva Maneuver
- Arm Squeeze Test
- Neck Tornado Test
During the second part of your examination, you should perform a neurological examination focusing on the presence and degree of radiculopathy evaluating hyporeflexia, hypoesthesia, and paresis:
The following video on dermatome testing was derived from the American Spinal Injury Association (ASIA) form:
Lee et al. (2008) evaluated the literature and created a composite dermatome map based on published data from 5 papers they considered to be the most experimentally reliable. Their maps look like this:
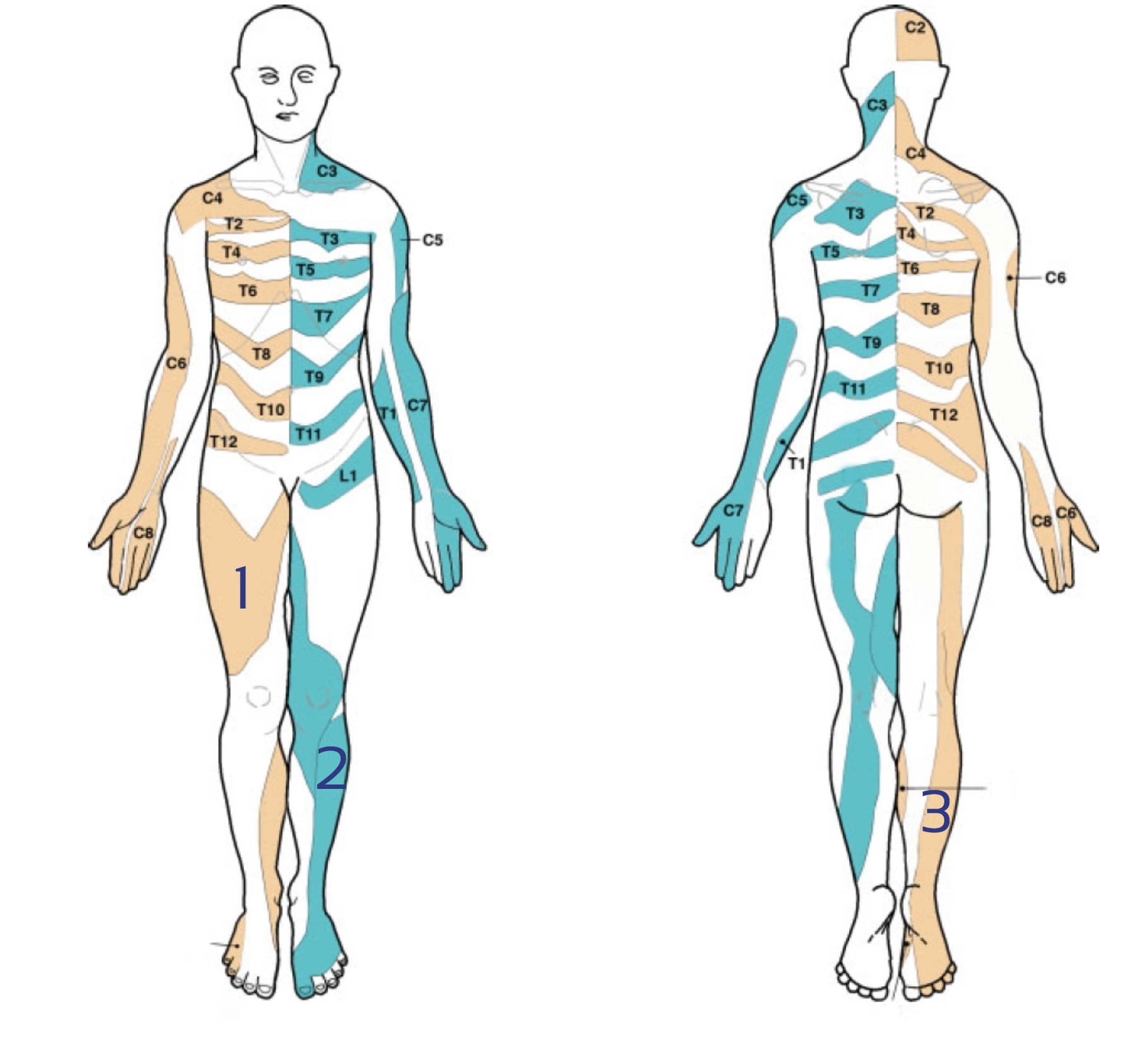
There is a lot of discussion going on about the reliability of dermatome maps. Check out our blog articles and research reviews if you want to learn more about it:
- Determining the Level of Cervical Radiculopathy
- Why Dermatome Maps may still useful
- 3 Truths University Didn’t Tell You about Radicular Syndrome
You can test the upper limb myotomes as explained in the following video:
Be aware, that cervical radiculopathy can be mimicked by a peripheral nerve entrapment. For more information check out the following videos:
- C5 radiculopathy or suprascapular nerve entrapment?
- C6, C7 radiculopathy or Carpal Tunnel Syndrome?
- C8 Radiculopathy or Ulnar Nerve Entrapment?
5 ESSENTIAL MOBILIZATION / MANIPULATION TECHNIQUES EVERY PHYSIO SHOULD MASTER