Meniscus Tear | Diagnosis & Treatment for Physios

Meniscus Tear | Diagnosis & Treatment for Physios
The meniscus is essential for stability, shock absorption, distribution of forces, lubrication in the knee as well as proprioception. (Englund et al. 2009)
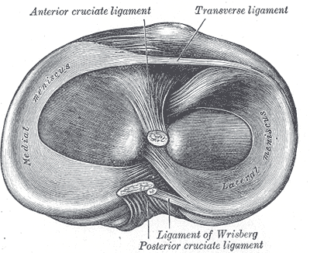 The medial meniscus has the form of a C and is approximately 3cm wide and 4-5cm long. The posterior horn of the meniscus is bigger than its anterior portion. The medial horn is generally attached to the tibia. The anterior horn is loose in 3-14% of the population. In general, the medial meniscus has a good capsular attachment via the coronary ligaments.
The medial meniscus has the form of a C and is approximately 3cm wide and 4-5cm long. The posterior horn of the meniscus is bigger than its anterior portion. The medial horn is generally attached to the tibia. The anterior horn is loose in 3-14% of the population. In general, the medial meniscus has a good capsular attachment via the coronary ligaments.
The lateral meniscus has the form of a half-circle and has a greater tibial surface area than the medial meniscus. It is approximately 3cm wide and 3-4 cm long and is attached to the tibia anteriorly and posteriorly. The ligamentous attachment of the lateral meniscus is less developed, which gives it more freedom of movement than the medial meniscus.
Meniscus injuries are mostly caused by rotation of a flexed knee into extension (Bansal et al. 2002).
All movements which can lead to ligament injuries in the knee can also cause meniscus injuries (Solomon et al. 2002). For this reason, meniscal tears are often seen together with anterior cruciate ligament (ACL) tears. In acute injuries, the lateral meniscus is torn more often than its medial counterpart (Smith et al. 2001). On the other hand, the medial meniscus tears more often in patients with chronic ACL- insufficient knees who suffer a new trauma (Murrel et al. 2001, Keene et al. 1993, Irvine et al. 1992).
These different scenarios also lead to a different localization and type of rupture: In the case of a medial meniscus tear (with a chronic ACL tear) peripheral ruptures in the dorsal horn are seen more often and with a lateral meniscus tear (in the case of an acute ACL tear) more ruptures are seen in the dorsal horn or the mid-lateral third. (Shelbourne et al. 1991, Thompson et al. 1993, Smith et al. 2001).
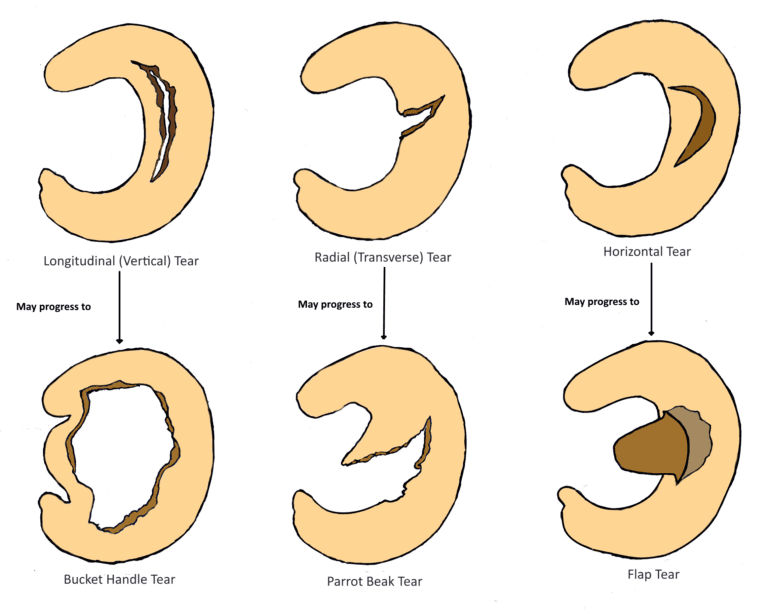
The menisci can be damaged through acute trauma or long-lasting overuse. Partial or full tears in the medial or lateral meniscus are further categorized into:
– Vertical/longitudinal tears may progress to Bucket Handle Tears
– Radial/Transverse tears may progress to Parrot Beak Tears
– Horizontal tears may progress to Flap tears
Epidemiology
The incidence of a meniscus injury presenting to the general practitioner is estimated at 2 out of 1.000 patients per year with a male: female ratio of 2,5:1 (Belo et al. 2010). In a prospective cohort study in a primary care setting in the Netherlands, 35% of patients between 18 and 65 with an acute knee injury were diagnosed with a meniscus tear. In the same study, 11% had a combined ACL and meniscus tear, while 9% had a combined medial collateral ligament tear and meniscus tear (Kastelein et al. 2008).
While traumatic tears often occur in the menisci periphery and are seen in patients younger than 30, more complex and degenerative patterns tend to occur in older adults (Poehling et al. 1990).
It should be mentioned that meniscus abnormalities seen on MRI seem to be extremely common in the asymptomatic population as well.
In a study by Beattie et al. (2005) 43 out of 44 asymptomatic individuals with mean age of 41.1 (age range 20-68) showed at least one meniscal abnormality.
27 individuals (61.4%) had abnormalities in at least three of the four regions of the knee.
It is important to add that meniscal tears can lead to knee osteoarthritis (OA), but knee OA can also lead to a spontaneous meniscal tear through the breakdown and weakening of meniscal structure (Englund et al. 2009). While the prevalence of meniscus tears is very high in asymptomatic individuals, Bhattacharyya et al. (2003) found a significantly higher frequency of meniscal tears in individuals with symptomatic OA. On top of that, a study by Hunter et al. (2006) found a strong association between meniscal damage and cartilage loss.
Clinical Picture & Examination
A meniscal injury can cause pain and edema and a locking knee during flexion and extension.
The chance of a meniscus lesion is increased in case the patient is older than 40 years of age and has suffered from a rotation trauma during weight-bearing of the knee, which makes continuing activity impossible. Furthermore, a popping sensation during trauma makes a meniscal tear more probable (Wagemakers et al. 2008).
Further clinical signs & symptoms include (Décary et al. 2018, Wagemakers et al. 2008), :
– Isolated medial or diffuse knee pain location
– Knee complaint with progressive onset in degenerative meniscus tears
– Mild to severe pain while pivoting on the knee during activities of daily living or sports
– Joint swelling 12-24 hours after trauma
– Joint line tenderness
– Reduced AROM
– Pain in the end ranges of motion
Physical Examination
Shrier et al. (2010) argue that the physical examination for meniscal tears is different than diagnostic tests as meniscal tears are heterogeneous in nature, for example, posterior vs. anterior tears. Therefore, the authors reason that sensitivity and specificity values should not be relied on for meniscus injuries, but the choice of physical tests should rather be based on the logic underlying how different tests stress different parts of the meniscus.
Another very common test to diagnose meniscus tears is the Appley Test:
Other orthopedic tests to assess patellofemoral pain are:
- Joint Line Tenderness
- Jump Sign /Finochietto Test
- Thessaly Test
- Ege’s Test
- Duck Walk Test
- Bounce Home Test
THE ROLE OF THE VMO & QUADS IN PFP