
Case Study
Kevin is a 48-year-old runner, who has completed multiple marathons in the last decade. Since 8 months, he has developed vague lower abdominal and groin pain and also pain in front of the pelvis, which started while training for an ultra-marathon event. Imaging results have confirmed the diagnosis of osteitis pubis and his condition has not improved despite extensive rehabilitation, soft tissue therapy, adjuncts like compression therapy, etc.
So, how do you manage a patient like Kevin?
What is Osteitis Pubis?
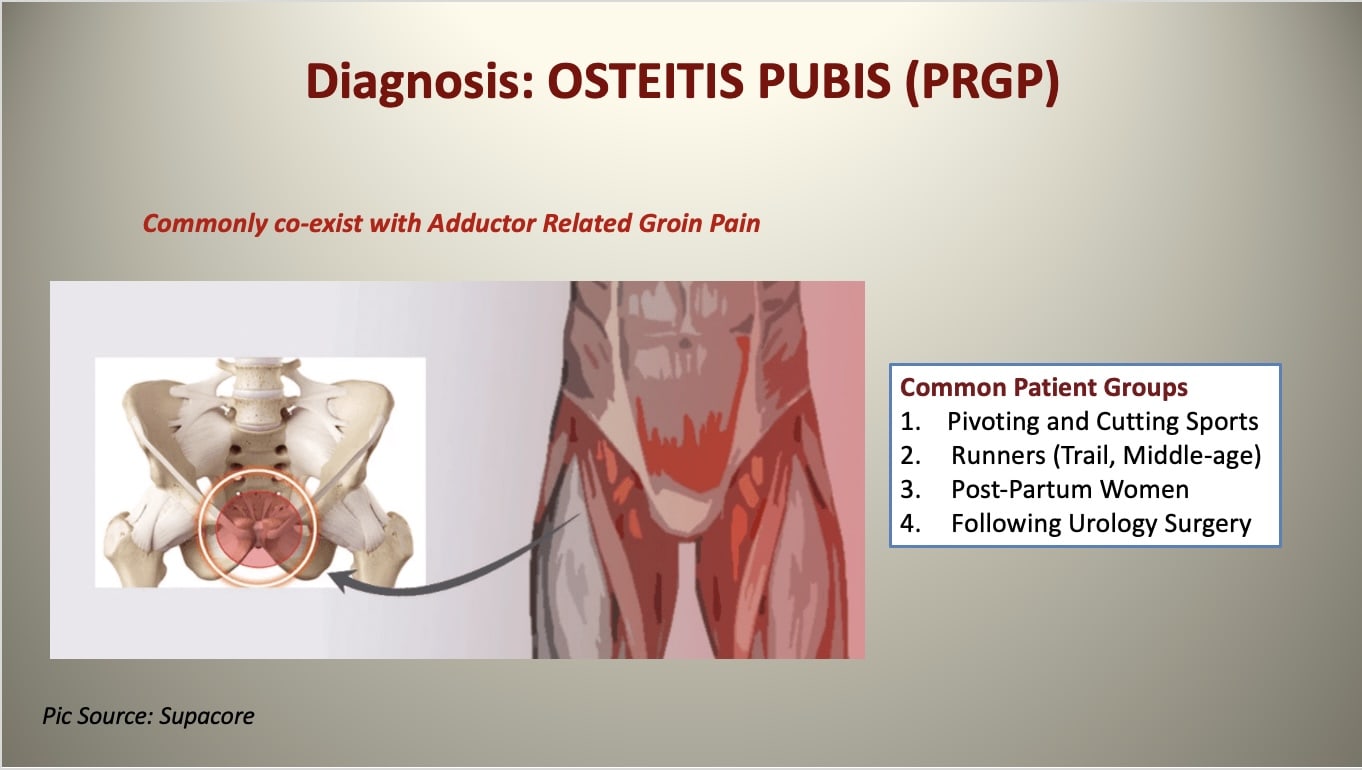
Osteitis Pubis refers to a non-infectious, inflammatory overuse syndrome affecting the symphysis pubis and surrounding soft tissues such as musculature and fascia, mainly in subjects participating in strenuous athletic activities. It can also occur in post-partum women or following certain lower abdominal surgeries. It was first described by Beer, a urologist in 1924, as a complication of suprapubic operations.
Athletes that develop osteitis pubis typically participate in sports producing twisting/shearing forces about the pelvis such as football, rugby, ice hockey, and American football. Often, this condition is accompanied by concomitant pathology, including sacroiliac joint dysfunction, athletic pubalgia (sports hernia), Femoro-acetabular impingement (FAI), adductor tendinopathy, and weakness in the core and pelvic stabilizer muscles (Beatty 2012).
Often osteitis pain takes more than 12 months to resolve and is a significant cause of disability in the athletic population (Morelli & Weaver 2005). If not managed adequately, this condition can lead to premature termination of athletic careers.
Pathophysiology
Osteitis pubis is thought to be a stress injury of the peri-symphyseal pubic bones secondary to increased strain on the anterior pelvis (Hiti et al. 2011). Bone biopsies of the superior pubic ramus in patients have shown the formation of new woven bone, osteoblasts, and neovascularization, with an absence of inflammatory cells and no signs of osteonecrosis, which is consistent with a bone stress injury (Verall et al. 2008). However, there are also reports of infectious aetiologies and osteomyelitis of the pubis, which can present in a similar manner (Pham & Scot, 2007).
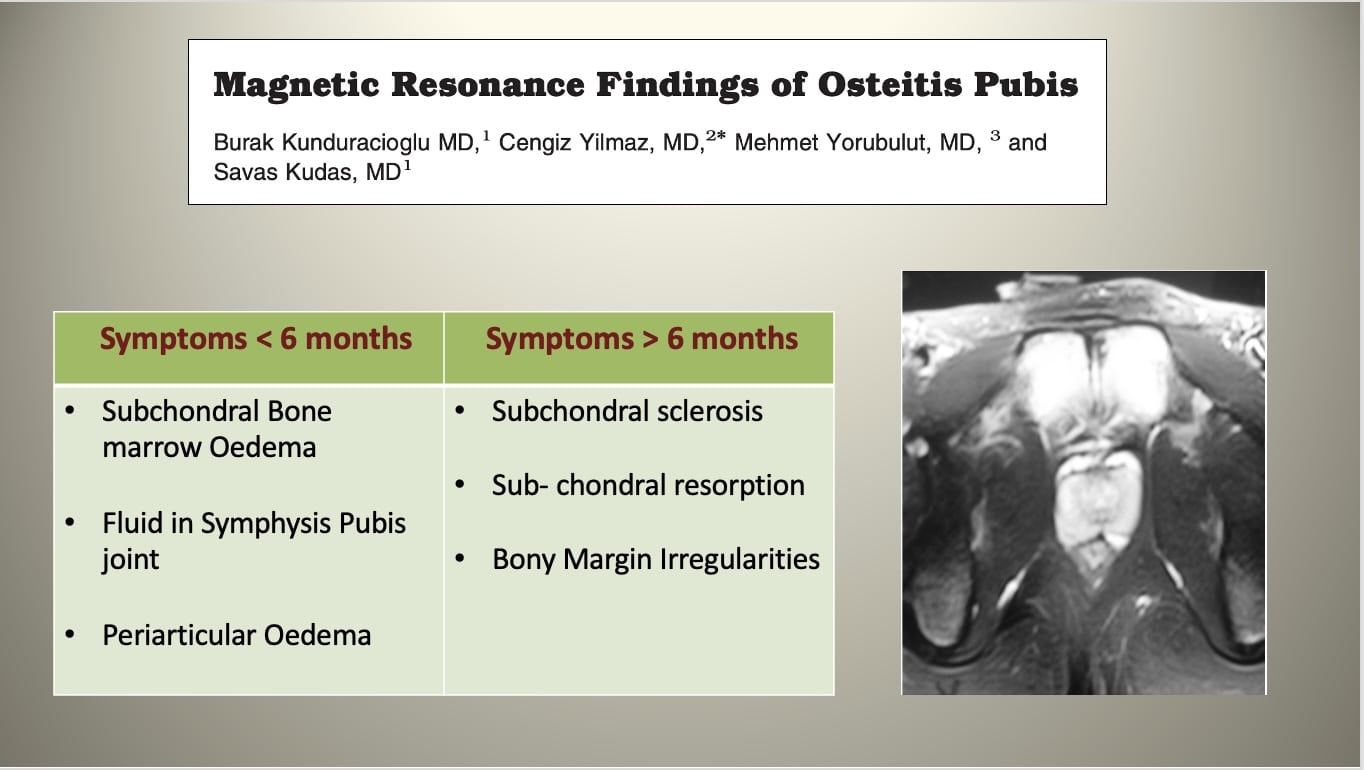
Chronic cases of osteitis pubis (> 6 months) can present with cystic changes, sclerosis, or widening of the symphysis on AP pelvis radiographs. A 1-legged stance AP pelvis radiograph (Flamingo view) can be used to evaluate for associated pubic instability. Widening (>7mm) or vertical shift (>2mm) indicates instability at the pubic symphysis (Garras et al. 2008).
Clinical Symptoms
The most common symptom of osteitis pubis is pain over the front of the pelvis. The pain is often central, although can be worse on one side than the other. It can also radiate down into one thigh or into the groin. Common complaints include the following:
- Pain localized over the symphysis and radiating outward
- Adductor pain or lower abdominal pain that then localizes to the pubic area
- Pain is exacerbated by activities such as running, pivoting on 1 leg, kicking, or pushing off to change direction, as well as by lying on the side
- Pain occurring with walking, climbing stairs, coughing, or sneezing
- A sensation of clicking or popping upon rising from a seated position or turning over in bed.
- Patients will have point tenderness to palpation directly over the symphysis pubis.
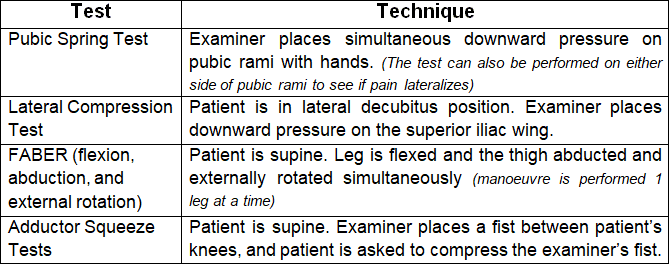
Specific physical examination tests that may elicit the classic pain include the “pubic spring” test and the “lateral compression” test, as shown in Table 1. A positive finding is pain reproduced at the pubic symphysis on the provocation maneuver.
Table 1 (Physical Examination Tests in Osteitis Pubis)
Differential Diagnosis
There are multiple causes of groin pain in runners including inguinal hernia, pubic rami stress fracture, intra-articular hip disease, genitourinary disease, and osteomyelitis. A key differential diagnosis for groin pain is sports hernia (also called Gilmore groin, Athletic Pubalgia, or Groin disruption). The term “sports hernia” has gained wide acceptance in the general population due to its common use in the media describing chronic groin pain in athletes. However, “sports hernia” is a misleading term, since it is not a true hernia but a core muscle injury and indicates a soft tissue defect of the posterior abdominal wall and its accompanying pain. Typically, the tendons of the oblique muscles, conjoint tendon, or transversal fascia are involved. To reproduce the pain of sports hernia, the patient should perform a resisted sit-up in crook-lying, while the examiner palpates the rectus abdominis insertion.
RUNNING REHAB 2.0: FROM PAIN TO PERFORMANCE
THE ULTIMATE RESOURCE FOR EVERY THERAPIST WORKING WITH RUNNERS
Imaging
X-rays of patients with osteitis pubis typically show an irregular pubic symphysis with sclerotic (thick) bone edges and evidence of chronic inflammation. An MRI test is usually not needed for diagnosis but will show inflammation of the joint and the surrounding bone.
Management Strategies
Early diagnosis and management are important as this injury can lead to a high degree of disability and time away from running an sport. Initial treatment is conservative with relative rest, activity modification, progressive loading program, and systemic non-steroidal anti-inflammatory drug therapy for pain relief.
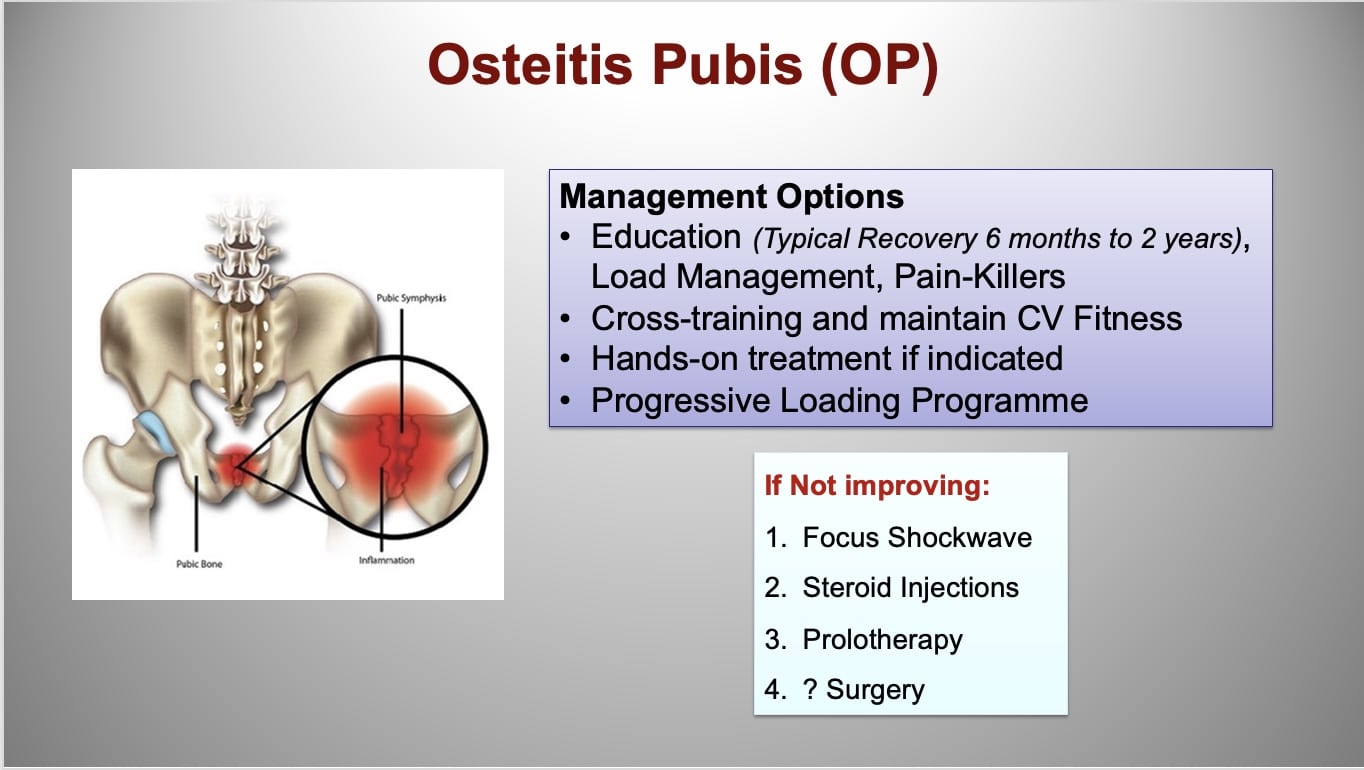
Rehab Programme (Progressive Loading)
Core and lumbopelvic exercises and progressive adductor strengthening are key components of the rehabilitation program. In cases of concomitant pelvic floor dysfunction, pelvic floor therapy may also be considered. The use of compression shorts may be useful in some patients for pain control.
Focus Shockwave for Bone Regeneration
Focus shockwave is a well-established treatment modality for bone stress injuries (Moretti et al. 2009). In a recent RCT, it has shown that focus shockwave significantly reduced pain in athletes with osteitis pubis and enabled return to play within 3 months of injury (Schoberl et al. 2017).
To learn more about the evidence-based application of shockwave in the clinical population, click HERE.
Injection Therapy for Pain Relief
In chronic cases not responding to rehab or FOCUS shockwave, injection therapy such as corticosteroid and prolotherapy could be useful for pain relief (Choi et al. 2011).
Surgery as Last Resort
Multiple surgical procedures have been described in the literature, ranging from simple debridement to symphyseal joint fusion. The majority of surgical interventions are considered salvage procedures with limited efficacy and are solely reserved for the most recalcitrant cases.
For further information, watch this podcast with Matthew Boyd (Osteitis Pubis: Pubic Bone Pain in Runners):
To learn more about the management of runners with injuries, including initial rehab, load management, strength training, and running re-training, check our comprehensive online Running Rehab Course with access to all information related to the rehab of running injuries.
I cover the management of Osteitis Pubis and other difficult running-related injuries in detail on my ONLINE RUNNING COURSE with runners and also on getting back to running, following hip and groin injuries.
Thanks a lot for reading!
Cheers,
Benoy
References
Beatty, T. (2012). Osteitis pubis in athletes. Current sports medicine reports, 11(2), 96-98.





