Don’t miss Femoral Stress Fractures in the Female Runner - How to uncover the most common red flag in female runners you don't want to miss
Case study
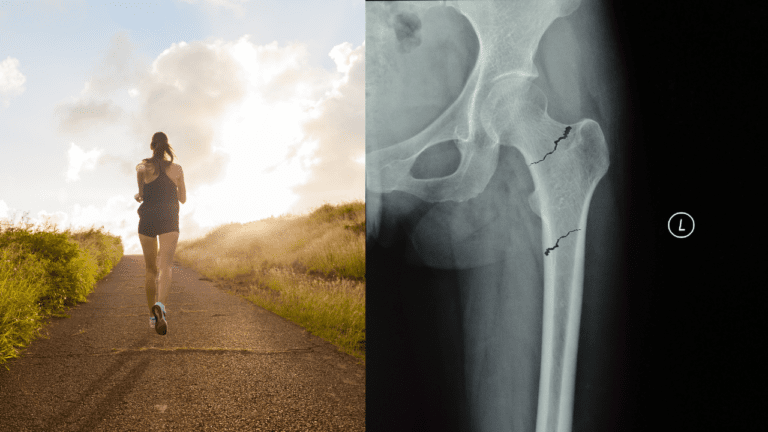
A 28-year-old woman presents to the physiotherapy clinic with a 3-week history of left groin and anterior thigh pain that has progressively worsened while training for her first half-marathon. She has reduced her training schedule to two sessions a week due to her pain and is currently unable to run beyond 15 minutes.
What is the ONE condition that you don’t want to miss in this runner?
A stress fracture is caused by repeated sub-optimal loading on a bone over time as opposed to a single severe impact. Stress fractures in the hip and pelvis region (femoral neck, pubis, sacrum, and ischium) are more common in female runners and should not be missed, as a possible differential diagnosis of hip and groin pain. Femoral stress fractures account for around 11% of all stress fractures in the athletic population.
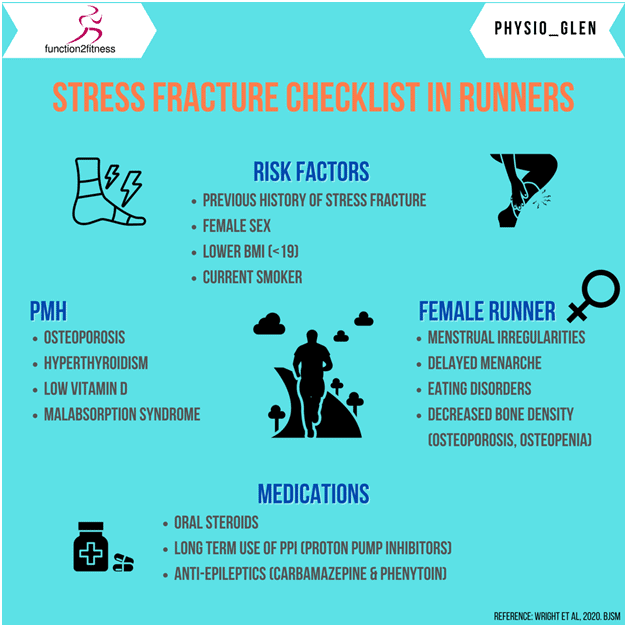
Risk Factors
There are multiple risk factors for the development of stress fractures within the athletic population. The key risk factors for stress fractures are highlighted below, as a checklist.
Clinical Presentation
In female runners, a history comprising of amenorrhea reduced calorie intake, and previous bone stress injuries should raise the suspicion of a stress fracture (Lodge et al. 2021). Most runners usually present with vague symptoms about the hip and groin region. Typically, the pain is diffuse around the groin, anterior hip and can radiate to the proximal thigh region. Tenderness is rarely elicited, even with severe stress fractures. The pain typically worsens with impact activities and worsens over time. In advanced cases, it may progress to night pain and even limping during walking (Petrin et al. 2016).
Femoral neck stress fractures are more concerning due to the risk of complete fracture, specifically for tension-type fractures on the superior neck. Compression fractures on the inferior neck are considered to be at much less risk of progression to complete fracture.
In female runners, a history comprising of amenorrhea reduced calorie intake, and previous bone stress injuries should raise the suspicion of a stress fracture
The risk of developing avascular necrosis following a displaced femoral neck fracture can be as high as 45% (Bachiller et al. 2002) and therefore, early recognition and management are crucial in the running population.
Physical Tests
The single-leg hop test is sensitive for a stress fracture, although it should be used cautiously in runners with severe symptoms. Two useful tests which I use with runners in the clinic, with suspected femoral stress fractures are the fulcrum test and patellar percussion test, which are described below.
Fulcrum Test
Patellar Pubic Percussion Test
Imaging
A plain radiograph cannot reliably exclude a stress fracture. Also, plain radiograph often appears normal in the initial stages despite clinical signs and symptoms suggestive of a stress fracture (Groves et al. 2005).
MRI is the gold standard for confirmation of a stress fracture. The advantage of MRI is that it can detect ‘bone stress response’ often weeks, before visible changes are noted on radiographs (Pegrum et al. 2012), thereby enabling early intervention. Alternative imaging modalities for the diagnosis of stress fractures include bone scintigraphy.
Running Rehab: From Pain to Performance
Improve Performance, Reduce Injury Risk and Optimise running economy in your patients!
Conclusion
Female runners are at increased risk for stress fractures in and around the hip. Clinicians should have a high index of suspicion for stress fractures as the cause of hip and groin pain in the long-distance female runner. The insidious onset of a vague, poorly localized pain is particularly concerning. A positive hop test combined with no specific tenderness raises particular concern for a stress fracture, which must be ruled out with imaging. Plain film X-rays are insufficient for early diagnosis and MRI imaging is recommended. Worsening hip pain in a runner and inability to bear weight should raise concern for serious hip pathology and prompt an urgent orthopedic referral.
Download our FREE FORM on Screening for Stress Fractures Checklist by Clicking HERE!
This blog article is taken from our Running Rehab – From Pain to Performance Online Course. To learn more about the management of runners with injuries, including initial rehab, load management, strength training, and running re-training, check our comprehensive online Running Rehab Course with access to all information related to the rehab of running injuries.
Thanks a lot for reading!
Cheers,
Benoy
References








