Iliotibial Band Syndrome | Diagnosis & Treatment for Physios

Iliotibial Band Syndrome | Diagnosis & Treatment for Physios
Introduction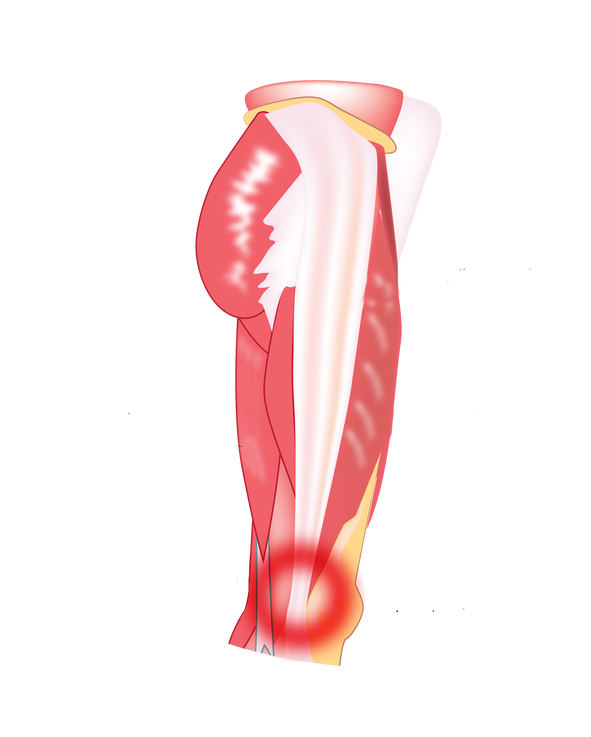
The literature handles different definitions of Iliotibial Band Syndrome (ITBS), which is sometimes referred to as Iliotibial Band Friction Syndrome, runner’s knee, or tractus iliotibialis syndrome (TITS). It is the most common running injury of the lateral side of the knee (Ellis et al. 2007) and the second most common overuse syndrome of the knee joint, after patellofemoral pain syndrome (Aderem et al. 2015).
There is an extensive body of research on the etiology of ITBS but no consistent definition of the underlying pathological mechanism of injury can be given. The most recent explanation is the combination of an impingement of the distal iliotibial tract at the lateral femoral epicondyle during repetitive flexion – specifically at around 30° of knee flexion. Additionally, compression of the highly innervated fat pad contributes to nociception (Baker et al. 2016, Taunton et al. 2002, Fredericson et al. 2000, van der Worp et al. 2012, Farrel et al. 2003, Ellis et al. 2007, Fairclough et al. 2006, Fairclough et al. 2007).
The question remains why the irritation occurs in the first place. Several studies investigated the role of intrinsic risk factors, such as glute strength and knee extensor/flexor strength, as well as extrinsic factors, such as the specific aspects of training (van der Worp et al. 2012).
Aderem et al (2015) report on modifiable and non-modifiable factors where the previously mentioned factors are modifiable and features such as anatomical leg length difference or a more prominent lateral femoral epicondyle are non-modifiable.
Epidemiology
ITBS rarely occurs in sedentary people and is most often seen in physically active individuals. The incidence and prevalence of running-related injuries (RRI) occurring during races or training varies between 25% and 65% of which ITBS is estimated to make up 5% – 14% of cases. Detailed and accurate reporting on the incidence is difficult as many studies do not only report on the incidence of ITBS and the characteristics of this group but report the incidence of all knee injuries (van der Worp et al, 2012).
LEVEL UP YOUR DIFFERENTIAL DIAGNOSIS IN RUNNING RELATED HIP PAIN – FOR FREE!

Treatment
So before we discuss what you can do to rehab ITBS, let’s first look at what you shouldn’t do: As the ITB cannot lengthen, stretching is not a useful treatment option. Neither is foam rolling which – contrary to popular belief – does not release or break down adhesions. Given that ITBS is probably a compression injury, these 2 treatments might actually make matters worse.
So what should we do instead? When it comes to rehab for runners, we will have to focus on the following 3 main components, which were proposed by Willy & Meira (2016). These are:
- Peak loads, which will be addressed by heavy slow resistance training
- Energy storage & release, which we will train with plyometric exercises and
- Cumulative loads will be addressed by a graded return to running including running retraining.
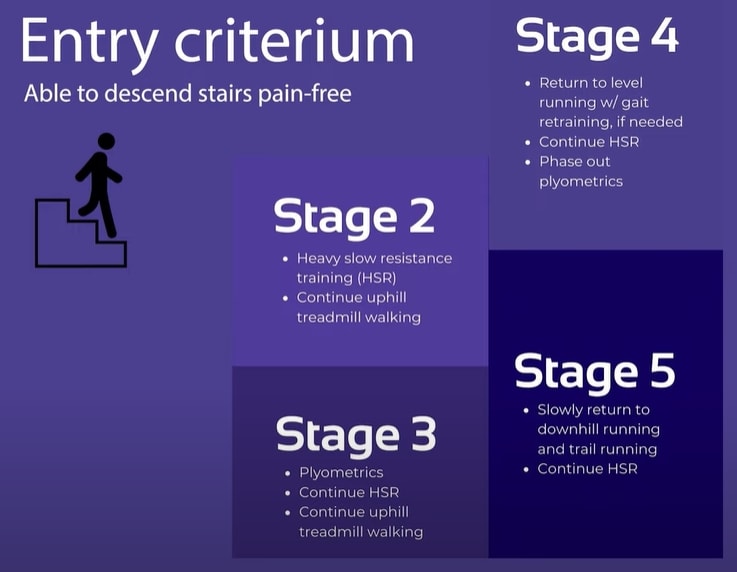
Our colleague Tom Goom has suggested the following 5 stage to progress ITB rehab in runners, which includes the 3 main components of rehab as well:
Stage 1 – The Pain Dominant Phase: Decrease irritability (without sacrificing capacity)
How do you know that your patient is in stage 1? These are patients that have often ceased running completely and who experience pain when descending stairs and with fast walking.
In this phase, the patient should reduce excessive overload by activities that further provoke the ITB. At the same time, we do not want a complete cessation of activities and keep their general activity level as high as possible.
In concrete, a patient should cease running – especially trail or downhill running – but switch over too fast treadmill walking with an inclination of around 8 to 10 degrees. If this is also not possible, the patient should explore if cycling with a low saddle or swimming are pain-free alternatives.
The following exercises are low-load options that focus on strengthening the hip abductors and extensors:
- Clamshells
- Side-lying abduction
- Thomas Exercise / ITB Excursion Exercise: 10x10s holds
Stage 2 – The Load Dominant Phase
The load dominant phase is entered as soon as the patient is able to descend stairs pain-free.
Stage 2: HSR training to address peak loads running
They then enter stage 2 which mainly focuses on heavy, slow resistance training. While uphill treadmill walking is continued, the exercises from stage 1 are further progressed:
- Side-lying abduction 🡪 Side planks
- Thomas Exercise 🡪 Single leg bridges
- Fire hydrants
- Split Squats (Training leg is the trailing leg, shift as much weight to the back leg)
- Side lunges against a resistance band
3 sets of 10-12 repetitions progressed to 4 sets of 6-8 with increased resistance/weight and near muscular failure on the last rep. These heavy-slow resistance exercises should be performed 3 times a week until a return to running is achieved in stage 5. The same is true for uphill treadmill walking which can be ceased as soon as running can be resumed.
Stage 3: Plyometrics to address energy storage and release during running
When rehabbing a patient with ITBS it’s important to realize that the ITB acts similar to a tendon in a way that it stores and releases energy during running as mentioned in a study by Eng et al. (2015). For this reason, we will have to train the ITB function to deal with energy storage and release activities without the cumulative load we get from running. The fact that the ITB works like a tendon should also make us wonder why many approaches are trying to decrease stiffness and lengthen it. If there is one thing we know of tendons is that they need to be stiff to be efficient as spring and lengthening – like in Achilles tendon ruptures – renders them inefficient. To confirm this A study by Friede et al. (2020) showed that physiotherapy improved outcomes in patients with ITBS and actually increased ITB stiffness by 14%. Examples of plyometric exercises progressed from easy to more advanced are:
Plyometrics Beginners
- Mini Squat jumps
- Reverse Lunge + Hop
- Lateral skaters (with bands or step)
- Tempo run with elastic bands
Plyometrics Advanced
- Split Jumps
- Squat jump to single–leg landing
- Single leg hopping forwards and backward
Stage 3 is used as a rather short (~1 week) bridge from stage 2 to stage 4
Stage 4: Return to level running + gait retraining
As soon as stage 4 is entered, the plyometric exercises are phased out in the second or third week.
Running should be re-introduced in a graded manner. To give you a concrete plan on how to build up running download our “From the Couch to 5K” running plan for free. This pdf is one of many useful documents from our running rehab online course.
A good idea is to gradually lower the inclination angle of the treadmill from 8-10 degrees to 5 degrees until the runner is able to run on level ground or outside again. There are a couple of biomechanical factors that can be targeted by mirror re-training. Be aware that gait modifications should be specific to the runner in front of you and don’t apply to every case:
- Increased step width: While cross-over gait usually puts more strain on the ITB, running with a wider gait reduces compression. You can train this by giving the patient cues like “Don’t cross over the line” after you have drawn a line with chalk in the middle of the treadmill.
- Increase the knee window: This means that there is space between the knees when you analyze their running pattern from a posterior view. A cue to achieve a bigger knee window could be to tell your patient “Don’t let your knees kiss” or you could put some tape on the outside of both knees and tell the patient to “push the markers apart”.
- If the patient presents with a pelvic drop also called the Trendelenburg sign, you could put markers on their iliac crest and cue them to “keep the markers level”.
- Increase cadence: Increase the cadence by about 5-10% which can be achieved by a metronome for example and reduces the peak load on the knee as well as peak hip adduction.
Running retraining is especially important as a study by Willy et al. (2012) showed that glute strengthening does change running mechanics. In the same study, they confirmed that mirror gait retraining on the other hand is effective for improving running mechanics.
Stage 5: Return to downhill running and trail running
In this last stage 5, the runner should gradually increase his running volume. Trail and downhill running can be gradually added on separate days before they are combined in a session.
Okay, so first of all a quick shout out to running experts Rich Willy, Tom Goom, and Benoy Mathew for valuable input for this post.
Would you like to learn more about Iliotibial band syndrome? Then check out the following resources:
- Iliotibial Band Syndrome – Facts or F(r)iction?
- Online Sports Conference 2022
- Foam Rolling – Sense & Non-Sense
- Running a Half-Marathon with ITB Pain
- Successful Return to Running Webinar
References
Illustration adapted from: http://www.bodyheal.com.au/blog/iliotibial-band-syndrome-symptoms-causes-treatment







