Greater Trochanteric Pain Syndrome | Diagnosis & Treatment
Greater Trochanteric Pain Syndrome | Diagnosis & Treatment
Introduction
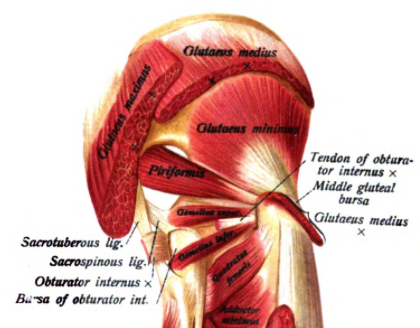
Gluteal tendinopathy or greater trochanteric pain syndrome (GTPS) describes lateral hip pain originating from irritation of the tendons of the gluteus medius and minimus. It used to be called trochanteric bursitis though the nomenclature has changed as more evidence from radiological, histological, and surgical studies emerged that showed non-inflammatory changes to the tendons rather than inflammation of the bursa (Grimaldi et al. 2016).
Generally speaking, tendons that experience normal and regular load are in a state of homeostasis; slightly greater than normal load will lead to a net anabolic biological response which results in increased tensile strength and favors the tendon’s load-bearing capacity.
A sedentary person may not induce these net anabolic responses through regular tendon loading and being overweight requires more load-bearing capacity, which may induce catabolic biological responses and reduce the tensile strength of the tendons.
On the other hand, a very active person who repeatedly puts the tendon under loads much greater than normal without adequate recovery time hinders the tendon to adapt appropriately and can lead to the development of tendinopathy (Magnusson et al. 2010).
Epidemiology
Gluteal tendinopathy is considered to be the most common tendinopathy of the lower extremity and is most prevalent in women over the age of 40 (Albers et al. 2014, Segal et al. 2007). Typical patients tend to be rather sedentary and overweight, though the condition can also be encountered in athletic populations, specifically runners (Del Buono et al. 2012).
LEVEL UP YOUR DIFFERENTIAL DIAGNOSIS IN RUNNING RELATED HIP PAIN – FOR FREE!








