Carpal Tunnel Syndrome | Diagnosis & Treatment

Carpal Tunnel Syndrome | Diagnosis & Treatment
Introduction & Epidemiology
The Carpal Tunnel is a passageway for the tendons of the flexor digitorum profundus & superficialis, flexor policis longus, and the median nerve enclosed by the hamate, trapezium, trapezoid, and capitate bone as well as the flexor retinaculum spanning from the trapezium to the hamate. 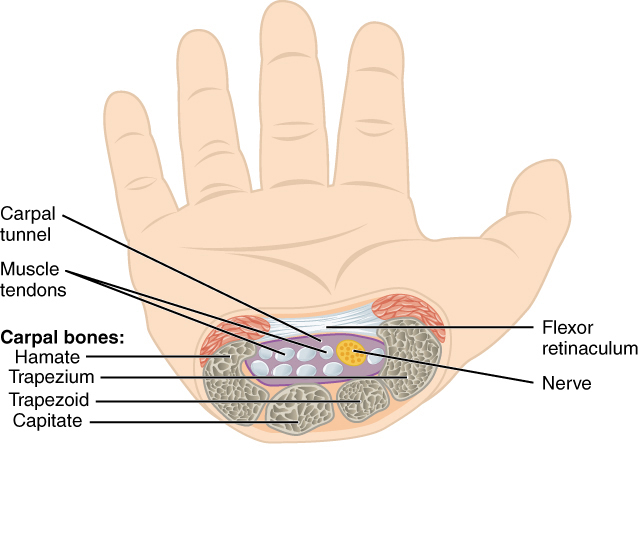
Carpal Tunnel Syndrome (CTS) is a syndrome or cluster of symptoms relating to pathology within the carpal tunnel and involves pain, neurological symptoms, and functional impairment of the hand.
Epidemiology
CTS or median nerve entrapment at the wrist is the most common entrapment neuropathy of the upper limb. The reported prevalence rate among women is 3% and 2% among men. Reports on the incidence vary from 324-542/100.000 in women to 166-303/100.000 in men (Atroshi et al. 1999, Gelfman et al. 2009).
It typically occurs between the age of 40-60 with a peak prevalence at 55 (Atroshi et al. 1999). Among pregnant women, the prevalence goes up to 62% (Ablove et al. 2009).
Pathophysiological mechanism
Oftentimes, the symptoms present in patients with occupations that involve repetitive and forceful hand tasks. This may result in swelling of the tendons narrowing the carpal tunnel and compromising the median nerve. Practically anything that can cause such narrowing may be a possible cause of CTS (Bekkelund et al. 2003, Kamolz et al. 2004, Middleton et al. 2014):
- Trauma: radial fracture, hemorrhage, carpal bone luxation
- Tumors: lipoma, ganglion, osteophytes
- Swelling of tendons
- Arthritis
Furthermore, there are risk factors associated with peripheral nerve pathologies such as CTS. These are pregnancy, obesity, hypothyroidism, renal failure, diabetes, and rheumatoid arthritis (Geoghegan et al. 2004).
Clinical Presentation & Examination
Signs & Symptoms
The cardinal signs of CTS are pain, paresthesia, and loss of motor control in the distribution of the median nerve. This includes pain, tingling, numbness in the thumb, index, and middle finger as well as the lateral part of the ring finger. Furthermore, weakness of the thumb, loss of grip strength, and varying degrees of loss of function, which is worsened nocturnally, are seen in CTS (Middleton et al. 2014).
It is also not uncommon that the symptoms occur bilaterally though this does not have to occur concurrently (Bagatur et al. 2001).
Physical Examination
Carpal Tunnel Syndrome may appear similar to radiculopathy in the distribution of cervical nerve roots C6 & C7. The differentiating factor is not only provocative testing of the cervical spine versus tests for CTS that we cover below, but an affected median nerve shows weakness and atrophy of the thenar and first two lumbrical muscles, which are innervated by C8-T1.
The most common tests are the Phalen’s test and the Tinel sign at the wrist. Wainner et al. (2005) have proposed a clinical prediction rule for the diagnosis of CTS. Watch the videos below to learn more.
Other common orthopedic tests to assess carpal tunnel syndrome are:
WATCH TWO 100% FREE WEBINARS ON SHOULDER PAIN AND ULNA-SIDE WRIST PAIN




