Achilles Tendon Rupture | Diagnosis & Treatment
Achilles Tendon Rupture | Diagnosis & Treatment
Introduction & Pathophysiology
The Achilles tendon is the biggest and strongest tendon in the human body. It is formed by the tendons of the soleus and gastrocnemius muscles and 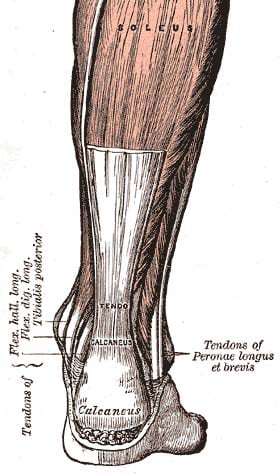 inserts at the calcaneus. The tendon is exposed to loads that are four to seven times a person’s body weight when walking and running (Giddings et al. 2000).
inserts at the calcaneus. The tendon is exposed to loads that are four to seven times a person’s body weight when walking and running (Giddings et al. 2000).
A rupture of the Achilles tendon usually occurs during athletic activities when heavy loads are placed on the tendon as occurs during acceleration or jumping (push-off). So the mechanism of injury can be (Arner et al. 1959):
- Weight-bearing push-off with extended knee
- Sudden, unanticipated dorsiflexion of the ankle
- Forceful dorsiflexion of the plantarflexed foot
When the tendon ruptures, this usually occurs between 3-6 cm proximal to the calcaneal insertion (Moon et al. 2017).
Epidemiology
Achilles tendon ruptures are mostly seen in high-impact sports and occur more often in the male population. A study in Denmark reports an increase from 25.95/100.000 persons in 1994 to 31.13/100.000 in 2013 (Ganestam et al. 2016).
The literature lists a couple of risk factors that may predispose an individual to ruptures of the Achilles tendon (Jarvinen et al. 2005, McQuillan et al. 2005, Seeger et al. 2006, Kraemer et al. 2012)
These are:
- Tendon degeneration
- Poor tendon vascularity
- Corticosteroid use
- Fluoroquinolone use
- Previous contralateral rupture







