
Tendinopathy has a multifactorial etiology that is not well understood. Risk factors are often separated into extrinsic factors, so those acting on the body from the outside and intrinsic factors, so all factors acting from within the body. In their narrative review, Peter Malliaras & Seth O’Neill (2017) discuss 3 different classes of risk factors. They are looking at:
- Load-related (extrinsic) factors
- Biomechanical (intrinsic) factors
- Other individual and systemic factors (which can be classified as intrinsic) as well.
Load-related extrinsic factors
1) Load: Stretch-shorten cycle loads
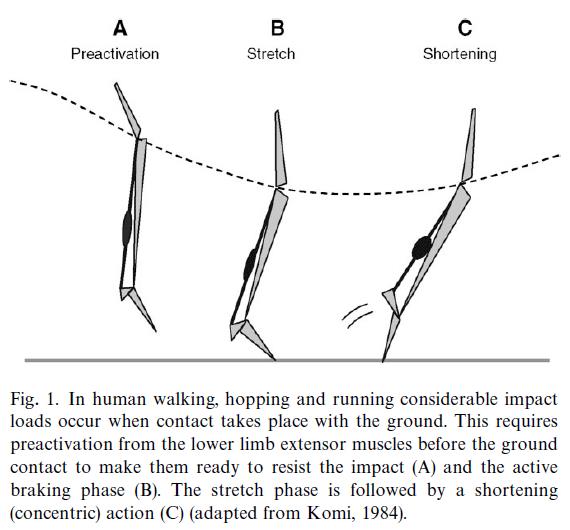
Repetitive stretch-shortening cycles of the muscle-tendon unit such as walking and running for Achilles tendinopathy or jumping for patellar tendinopathy are associated with tendinopathy. The tendon load may only be able to explain part of the story. In running and submaximal hopping the Achilles, tendon load is reported to be 6-8 times and 8-10 times bodyweight respectively, while the load during maximal isometric plantarflexion contraction is only 3.5 times body weight.
On the other hand, the load on the patellar tendon during squatting is similar to a spike jump take off with 4.8 times bodyweight and 5.2 times bodyweight respectively. The crucial difference between fast+high load activities and slow +high load activities like in rehab is the tendon strain rate. While in squatting it is about 1-2 times bodyweight per second, it is as high as 40 times bodyweight per second in a spike jump take-off. This probably explains why tendinopathy is associated with repetitive stretch-shortening cycles while slow and heavy loading is not.
2) Compression:
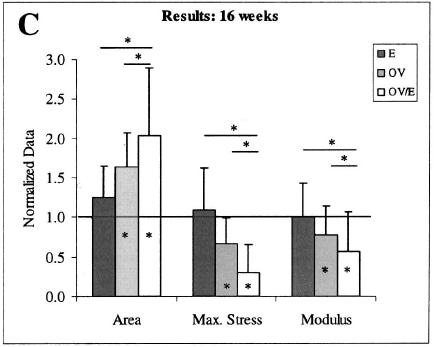
A classic study by Soslowky et al. (2002) manipulated mice so that one group had an enlarged acromial roof (group E), another group was overloaded by downhill running (group OV) and a third group had both external compression and overload combined (Group OVE/E). The results of that trial showed that compression alone did not lead to pathology, but a combination of compressive and tensile loads was more damaging than tensile loads alone.
Compression alone does not lead to pathology, but a combination of compressive and tensile loads
3) Change in load

The most common cause for tendinopathy is training errors involving sudden changes in load. This encompasses any fluctuations in intensity, frequency, or duration of exercise or a combination of all three. For this reason, tendinopathy is often seen in athletes in the pre-season after a holiday break. As mentioned before, important is a change in energy storage type of loads as they stress the tendon the most. When taking patient history in patients in who you suspect tendinopathy ask for hill or speed sessions, marathon, or similar events if they have bought a sports watch or Fitbit which motivated them to push harder, preseason breaks, or a change in shoes or training surface
4) Load parameters
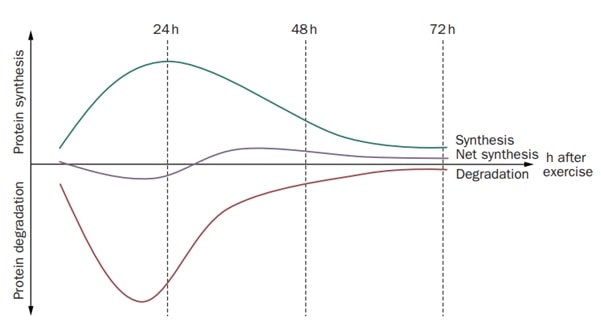
Higher Load duration, intensity, and frequency are associated with patellar pain and Achilles tendinopathy. This fits the evidence of Magnussen et al. (2010) who have found that repeated intense loading without sufficient recovery may be a risk factor for tendon pathology. Be aware, that this association is not consistent however and that a change in load may be a confounder in this relationship.
5) Biomechanical and neuromuscular factors (intrinsic factors):
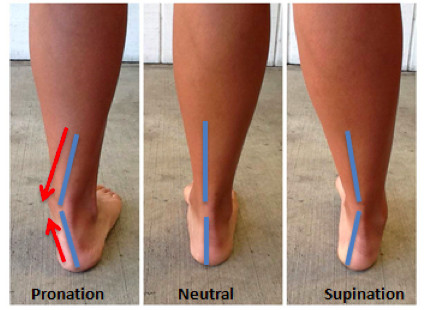
Individual biomechanics, including movement kinetics and kinematics, foot posture, flexibility, neuromuscular capacity, and structural anatomy may influence tendinopathy risk. However, the relationship between biomechanics and the development of tendinopathy is a mess. If you want to have a look at individual articles, we are highly recommending you start with this narrative review of Malliaras & O’Neill (2017).
In general, it seems that extremes in biomechanics might be risk factors worth paying attention to during rehab. For example, both increased and decreased dorsiflexion are described as risk factors in the development of Achilles tendinopathy. The same is true for increased as well as decreased hamstring flexibility for patellar tendinopathy.
The link between neuromuscular changes and pain is even less clear. Comparable to other body regions and pathologies cross-sectional students don’t allow us to say if neuromuscular impairments such as decreased strength are a consequence of pain or if they are a risk factor leading to tendon pain.
For our rehab, this means the following: while a good loading program is necessary for all patients, interventions to target biomechanical factors and neuromuscular changes might be necessary for some patients who are at the extreme ends of the spectrum. Similar to other body regions and with all the individual variation in posture and movement between individuals it’s difficult to really say which posture or movement is “faulty”.
At last, if we do assume to have found a biomechanical or neuromuscular factor the question is if we are able to change those factors by therapy.
6) Individual and systemic factors (intrinsic factors):

Multiple systemic factors have been linked with tendinopathy including age, high cholesterol, adiposity, and genetics. These systemic risk factors are thought to reduce the capacity of the tissue to tolerate load, gradually altering tendon capacity so that an extra walk, a quick dash across the road, or a day spent gardening may be sufficient to overload the tendon triggering symptoms. Systemic factors might also play a greater role in the case of bilateral involvement or in tendinopathy where load seems to play a smaller role such as in pes anserinus tendinopathy. Furthermore, these systemic factors combined with biomechanics might be able to explain why under similar loading conditions some athletes develop tendinopathy and others don’t. Finally, cognitive and emotional factors such as anxiety, illness beliefs, and fear-avoidance behavior can influence a person’s pain experience and should not be disregarded.
The envelope of function by Scott Dye beautifully summarizes the risk factors involved in the etiology of tendon pain:
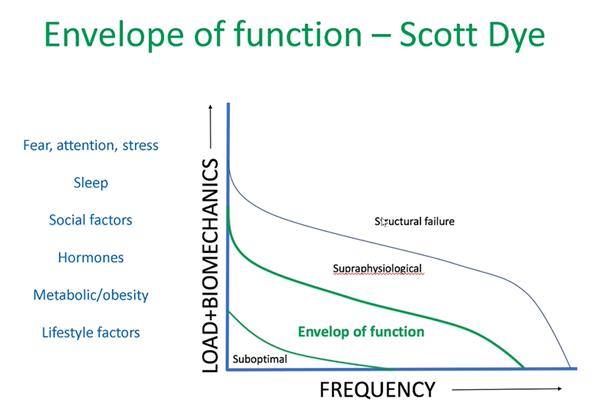
So the envelope of function is the load/frequency distribution that defines the safe or homeostatic range of load acceptance. So if the combination of load and frequency exceeds your envelope of function it will lead to pathology. It’s also interesting to see that suboptimal loading may lead to disuse effects, which we know is especially a problem in tendons. Peter Malliaras adds that biomechanics can directly influence the load in this graph. On the side systemic and individual factors will all have an influence on an individual propensity to develop pain.
THE BIG 3 – ADVANCED REHABILITATION OF HAMSTRING, QUADRICEPS, AND CALF MUSCLE- AND TENDON INJURIES
Claim your seat on our online course “The Big 3 – Advanced Rehab of of Hamstring, Quadriceps & Calf muscle and Tendon Injuries” To Improve your Rehab, Reduce Injury Risk and Optimize Return to Play!
Alright, this was our blog on risk factors for tendinopathy. We hope you enjoyed reading it! If you love tendons and would like to learn more about the topic, check out our video on 7 absolutely crucial facts about tendons you didn’t know. As always, thanks for reading!
References









{kind=link}