When can I return to run? Do you recognize that question of your ACL reconstructed patient in your clinic? How confident are you to make an informed clinical decision to return your athletes to running? In this blog, I will present a short overview of the why, what, and how of return to running after ACL reconstruction.

Dr. Bart Dingenen
When can I return to run? Do you recognize that question of your ACL reconstructed patient in your clinic? How confident are you to make an informed clinical decision to return your athletes to running? In this blog, I will present a short overview of the why, what, and how of return to running after ACL reconstruction.
Why is return to running important?
Currently, we consider ACL rehabilitation as a continuum (Dingenen & Gokeler 2017). We start with the end in mind. Each exercise, set, rep or decision we take during rehabilitation can be considered as a small step in the direction of the end goal, return to performance. Appropriate running mechanics are the foundation for more advanced high-intensity and multidirectional movement competencies that need to be developed further across the rehabilitation. Or how would you expect to create acceleration, deceleration, change direction, and agility mechanics in your journey towards athletic performance?
Appropriate running mechanics are the foundation for more advanced movement competencies
As such, return to running is an important milestone within the whole process for the patient as well for the treating physical therapist, not only from a physical but also from a psychological point of view. “Check, I can run again!” After numerous weeks of recovering from the consequences of the injury and reconstruction such as pain, swelling, range of motion limitations, muscle atrophy, and doing exercises focusing on foundational movement patterns, your patient is typically looking forward and eager to return to run, finally! But when can they return to run? To be able to answer this question, we should first answer another question: What is running?
What is running?
When making task-based progressions across the rehab process, we should understand the biomechanical requirements of running. Let’s get back to the basics. During running, alternate periods of acceleration and deceleration occur during running, typically referred to as absorption and generation (Novacheck 1998). Simply stated, you land alternately on one limb. Wow, really? Yes! Saying this might sound too logical, but still, you don’t want to know how many times patients try to return to run after their wonderful “rehabilitation” of underloaded double-leg squats. Oh yes, on a Bosu-ball, I almost forgot to mention. Should it be surprising that these athletes return unsuccessfully to running?

The ground reaction forces during each of these steps equal approximately 2-3 times body weight. Next to these higher peak loads, your athlete will be subjected to rates of loading and cumulative loadings which are typically far beyond what they were prepared for. Again, should it be surprising that these athletes return unsuccessfully to running?
The muscles developing the highest peak loads during normal running are especially the calves and the quads (Dorn 2012). Unfortunately, a significant strength deficit is typically present at the time to return to run (and even return to sport later on) in these muscles, especially in those with underloaded rehabilitation for these specific muscle groups. “But my training is at least functional” … Mmm, and what about isolated strength training to prepare your athlete for the demands of the tasks you want to target? Quads and calves should be the key priorities. Again, should it be surprising that these athletes return unsuccessfully to running?
What are the typical deficits or problems during running after ACL reconstruction?
Sagittal plane knee kinematics and kinetics appear to be most affected during running after ACL reconstruction at short- (3 months), mid-and long term (up until at least 5 years after ACL reconstruction) (Pairot-de-Fontenay et al. 2019). More specifically, combined results of a systematic review reported strong evidence for:
- Lower peak knee flexion angle
- Lower internal knee extension moment
- Lower rate of internal knee extension moment
in the involved limb during the stance phase of running after ACL reconstruction compared to both contralateral and control limbs (Pairot-de-Fontenay et al. 2019).

Quadriceps and hamstring strength asymmetries, and knee function, but not surgical techniques, were proportional to both knee kinematics and kinetics during running after ACL reconstruction (Pairot-de-Fontenay et al. 2019). Even though a cause-effect relationship cannot be extracted from studies looking at correlations, the role of (eccentric) quadriceps strength and rate of force development has been acknowledged in relation to the aforementioned biomechanical alterations (Spencer et al. 2020, Alzakerin et al. 2021). Interestingly, time after reconstruction alone seems not to be sufficient to restore knee biomechanics during running. Cyclic repetition of running with these biomechanical alterations might be one of the factors leading to future knee symptoms and knee osteoarthritis.
ACL Injuries: From Theory to Practice
This first-of-its-kind online course offers an incredible continuing education opportunity for clinicians who manage patients with ACL injuries
How can you evaluate your patient?
Yes, I know, this is the question you were interested in. Unfortunately, there is currently only very limited literature available to guide our clinical decisions. Most studies are predominated by personal opinions.
In a scoping review by Rambaud et al. (2018), including 201 studies from 1981 to 2016, time was the most frequently reported criterion for return to running. A median of 12 weeks postop was reported. However, it was unclear how many patients had exacerbations of symptoms, sustained new injuries, or presented with altered biomechanics in the short or long term. Fewer than 1 in 5 studies reported clinical, strength, or performance-based criteria (which were almost always self-selected by the authors).
More recently, Pairot de Fontenay et al. (2021) evaluated the predictive value of potential predictors of short-term success in 35 participants with an ACL reconstruction with a hamstrings autograft. The return to running was considered successful when the participants completed a return to run program consisting of 10 running sessions in 14 days at self-selected speed without any exacerbation of symptoms.
Potential predictors included:
- The International Knee Document Committee (IKDC) subjective knee form;
- ACL Return to Sport after Injury questionnaire (ACL-RSI);
- Quadriceps and hamstring strength, evaluated isometrically with a belt-stabilized handheld dynamometer, sitting on a table in 90° hip and knee flexion;
- Step-down endurance test;
- The modified Star Excursion Balance Test
The results of this study showed that the IKDC score was the only significant predictor of short-term success. Patients who scored >64/100 on the IKDC were 3-times more likely to tolerate the reintroduction of running without adverse reactions. A higher score might reflect a greater global capability (a mix of psychological, physical, and social factors) for the patient to tolerate load. The limitations of this study are the relatively limited sample size, the very short-term evaluation of only symptoms, and the self-selected speed of the participants.
Similarly, Iwame et al. (2021) evaluated 83 ACL reconstructed patients and found that quadriceps strength (evaluated with isokinetic strength assessment) divided by body weight was independently associated with return to run 3 months after surgery. The cut-off score here was 1.45 Nm/kg. When I was reading this study, I had two concerns:
1/ Their definition of successful jogging: Participants were instructed to start to run and gain speed as quickly as possible without any pain or feelings of anxiety. Those who ran with a mean velocity >9km/h were considered successful. Those with a mean velocity of <9km/h were unsuccessful. Again, information on biomechanics was not available in this study.
2/ Considering that athletes can achieve around 3Nm/kg quadriceps strength (often used as a “normal” value), 1.45Nm/kg is quite low to return to run (<50%). Lower than the overall clinical prescription of around 70% limb symmetry index (LSI). However, interpretation of these values in this study group is difficult as the sports level of the patient group was not clearly defined. Currently, we don’t know how much is enough, but 1.45Nm/kg seems to be rather low for athletes to return to run.
It is well accepted that quadriceps strength deficits persist longer in athletes with graft types directly affecting the extensor mechanism, compared to for example hamstrings grafts and allografts (Brinlee et al. 2022). Therefore, the return to run may be further delayed for those athletes with bone-patellar tendon-bone (BPTB) and quadriceps grafts. Similarly, other associated injuries and/or operative procedures (e.g. meniscus or cartilage) will further delay the return to run. Most of these patients with associated injuries can hardly walk normally at 4 to 6 weeks. How would you expect they can run appropriately a few weeks later?
In summary, the current research leaves us as clinicians with a certain amount of uncertainty. Some studies have evaluated the relation with the “success” of return to run, but the definition of a successful return to running is debatable. Given the evidence indicating biomechanical deficits during running, the addition of a biomechanical evaluation seems the logical next step. In the following section, a short overview of examples of return to running criteria being proposed in the literature is presented to assist you in your clinical decision-making in daily practice. Future studies must define whether we could or should use other criteria.
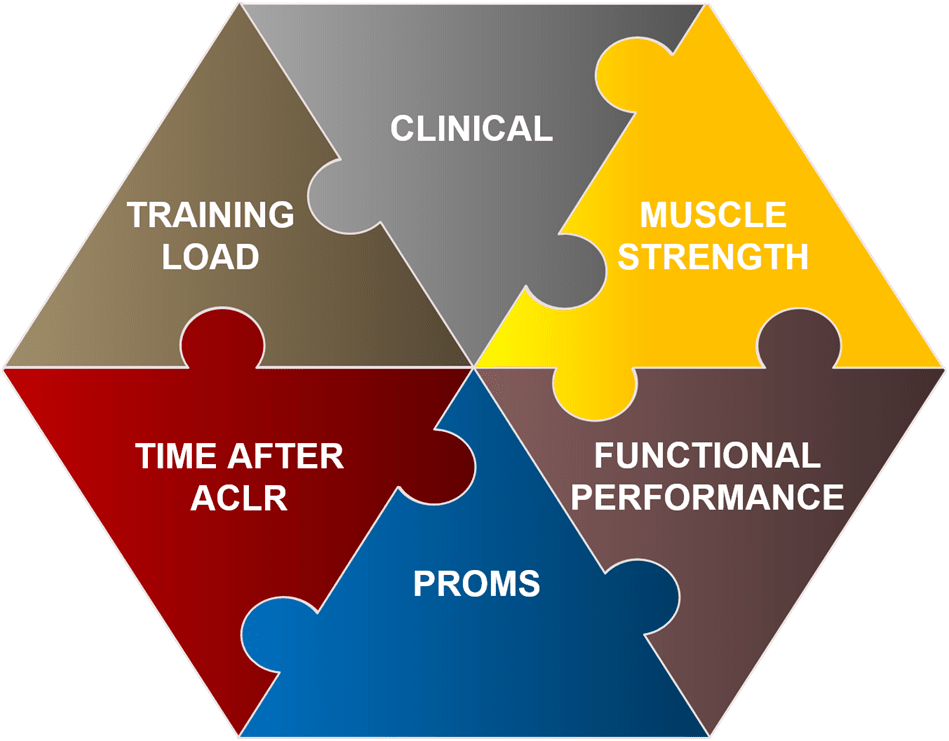
1. Clinical criteria
- Pain < 2/10 NPRS
- No effusion or trace
- Knee flexion 95% LSI
- Full knee extension (Rambaud et al. 2018)
Note: Return to run with an unhappy knee is not a good idea. Make sure the knee has calmed down before initiating higher load activities.
2. Muscle strength criteria
- Isolated strength evaluation quadriceps: LSI > 70%
- Quadriceps/body weight > 1.45Nm/kg. As noted, this value is probably too low for athletes. Taking into account the 70% calculation, this could be around 2.1 Nm/kg, but we currently don’t know how much is enough.
- Single-leg leg press > 1.25x body weight (Buckthorpe et al. 2020)
- Seated calf raise > 1.5x body weight (O’Neill et al. 2019)
- Heel raise endurance > 25 repetitions;
Notes:
- It could be argued that an appropriate amount of reactive strength is also needed to run efficiently, but this has not yet been studied so far in relation to ACL reconstructed patients and return to running.
- How strict you should be in achieving criteria can also be dependent on the individual level of sport and on the speed of return to running.
3. Functional performance-based criteria
- Qualitative performance during single leg squat, single leg landing and gait pattern.
- Quantitative based: being able to land repetitively on one leg to evaluation single-leg landing capacity: How many? 30? (Herrington et al. 2013)
4. Patient-reported outcome measures (PROMS)
IKDC > 64 (Pairot de Fontenay et al. 2021).
5. Time after ACL reconstruction
As previously indicated, we don’t know whether 12 weeks is enough, but if we would apply more strictly the strength-based criteria, most athletes will by definition be slower in their return to running. Personally, I like this approach better where we take a longer time to continue strength training before progressing to more dynamic activities such as running in the ACL rehab process. At the same time, the knee joint will have more time to recover from a biological perspective.
6. Training load criteria
Make sure you include a progressive running preparation period before starting to run. Skipping variations could offer a good loading stimulus to prepare for running with progressive magnitude of loading, rate of loading, and cumulative loading (McDonnell et al. 2019). When returning to running, we also use a progressive start to run program. While returning to run, it is also essential to evaluate running biomechanics (spatiotemporal characteristics, kinematics, and kinetics). Don’t panic if the first run is not perfect. They have to get used to running as well.
To conclude, we can say return is an important step within ACL rehabilitation. Don’t rush, take your time, train hard, consistent, and smart before progressing to more dynamic activities. By guiding your training prescription with regular testing, the risk for setbacks is probably lower.
Hopefully, this overview can help to guide the decision to return to running in your clinic!
All the best,
Bart
References
Alzakerin HM, Halkiadakis Y, Morgan KD. Med Sci Sports Exerc. 2021. Force and Rate Metrics Provide Return-to-Sport Criterion after ACL Reconstruction.
Brinlee AW, Dickenson SB, Hunter-Giordano A, Snyder-Mackler L. Sports Health. 2021. ACL Reconstruction Rehabilitation: Clinical Data, Biologic Healing, and Criterion-Based Milestones to Inform a Return-to-Sport Guideline.
Buckthorpe M, Della Villa F. Sports Med. 2020 50(4):657-678. Optimising the ‘Mid-Stage’ Training and Testing Process After ACL Reconstruction.
Dingenen B, Gokeler A. Sports Med. 2017 Aug;47(8):1487-1500. Optimization of the Return-to-Sport Paradigm After Anterior Cruciate Ligament Reconstruction: A Critical Step Back to Move Forward.
Dorn TW, Schache AG, Pandy MG. J Exp Biol. 2012 Jun 1;215(Pt 11):1944-56. Muscular strategy shift in human running: dependence of running speed on hip and ankle muscle performance.
de Fontenay BP, van Cant J, Gokeler A, Roy JS. J Athl Train. 2021. Reintroduction of running after ACL reconstruction with a hamstring graft: can we predict short-term success?
Herrington L, Myer G, Horsley I. Phys Ther Sport. 2013 Nov;14(4):188-98. Task based rehabilitation protocol for elite athletes following Anterior Cruciate ligament reconstruction: a clinical commentary.
Iwame T, Matsuura T, Okahisa T, Katsuura-Kamano S, Wada K, Iwase J, Sairyo K. Knee. 2021 Jan;28:240-246. Quadriceps strength to body weight ratio is a significant indicator for initiating jogging after anterior cruciate ligament reconstruction.
McDonnell J, Zwetsloot KA, Houmard J, DeVita P. Gait Posture. 2019 May;70:414-419. Skipping has lower knee joint contact forces and higher metabolic cost compared to running.
Novacheck TF. Gait Posture. 1998 Jan 1;7(1):77-95. The biomechanics of running.
O’Neill S, Barry S, Watson P. Phys Ther Sport. 2019 May;37:69-76. Plantarflexor strength and endurance deficits associated with mid-portion Achilles tendinopathy: The role of soleus.
Pairot-de-Fontenay B, Willy RW, Elias ARC, Mizner RL, Dubé MO, Roy JS. Sports Med. 2019 Sep;49(9):1411-1424. Running Biomechanics in Individuals with Anterior Cruciate Ligament Reconstruction: A Systematic Review.
Rambaud AJM, Ardern CL, Thoreux P, Regnaux JP, Edouard P. Br J Sports Med. 2018 Nov;52(22):1437-1444. Criteria for return to running after anterior cruciate ligament reconstruction: a scoping review.
Spencer A, Davis K, Jacobs C, Johnson D, Ireland ML, Noehren B. Clin Biomech (Bristol, Avon). 2020 Feb;72:58-62. Decreased quadriceps force steadiness following anterior cruciate ligament reconstruction is associated with altered running kinematics.






