
Research
Diagnosis & Imaging
April 15, 2026
Screening for Sleep Dysfunction Related to Musculoskeletal Pain - Part 1: Exploring the Physiotherapist's Role in Assessment

Introduction
In 2020, the American Physical Therapy Association published a position statement where the role of the Physiotherapist in screening for sleep disorders was recognized. While we know that poor sleep quality can predispose someone to musculoskeletal pain and vice versa, we don’t have many tools in our toolbox to counter this bidirectional relationship. Therefore, the current authors wrote a clinical commentary to help physiotherapy practitioners assess and address sleep dysfunction pragmatically. In Part 1, we outline how to screen for sleep dysfunction in musculoskeletal conditions.
Methods
The study we review here today is a clinical commentary, and with that being said, you must be aware that this does not reflect experimental studies like we use to review.
Therefore, there is no statistical analysis, no participants were included, and no intervention was delivered. Rather, the authors employed a pragmatic way of helping us screen for and address sleep dysfunctions in clinical practice. To do that, the existing literature was reconciled with clinical guidelines and prior frameworks.
Results
The authors present a stepwise sleep screening model.
In step 1, the authors outline a general sleep screening consisting of 3 questions.
- How many hours of sleep do you typically get?
- Do you feel well rested during waking hours?
- Would you say your overall sleep quality is: very good, fairly good, fairly bad, or very bad?
Gaining information about the amount of and quality of sleep before starting the subjective exam can help guide more specific questioning. If the person reports sleeping less than 7 hours, not feeling well-rested, or rates their sleep as fair or very poor, the clinician should ask if the person’s musculoskeletal pain condition is impacting their sleep in step 2.
Step 2 holds an important differentiation: is sleep dysfunction driving the musculoskeletal pain complaint, or is the pain a driver for poor sleep? While it may seem unimportant to consider this difference at first, it would be more relevant to act when an underlying sleep problem is identified that may be driving pain.
- Is sleep disturbed because of pain?
- Or did sleep issues exist before pain onset?
Knowing this, we get to understand better whether we would have to proceed with addressing the musculoskeletal pain or the sleep dysfunction itself.
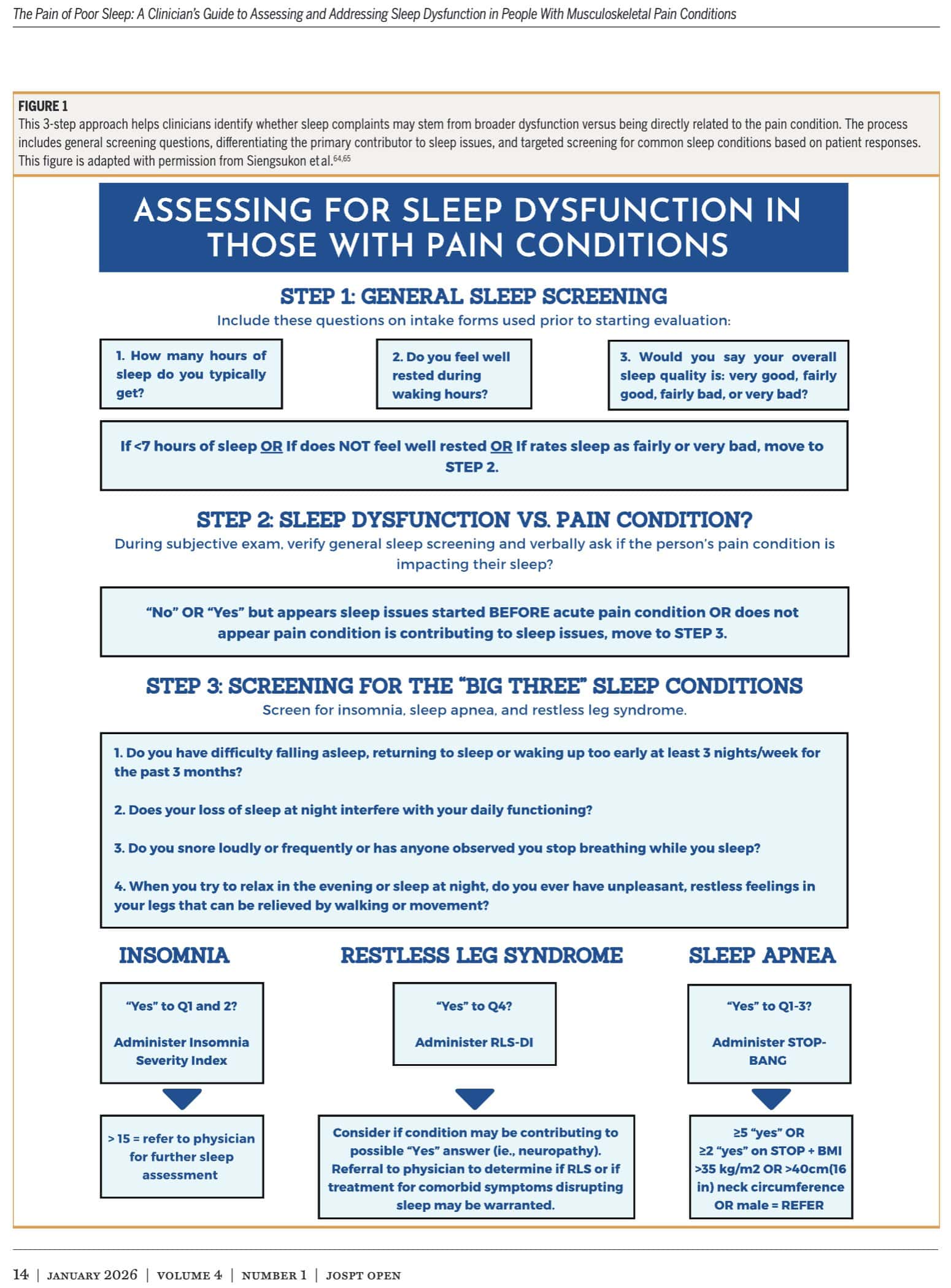
In Step 3, screening for the “big three” sleep conditions is advocated. The “big three” sleep disorders encompass insomnia, sleep apnea, and restless leg syndrome.
Four questions are to be answered:
- Do you have difficulty falling asleep, returning to sleep, or waking up too early at least 3 nights per week for the past 3 months?
- Does your loss of sleep at night interfere with your daily functioning?
- Do you snore loudly or frequently, or has anyone observed you stop breathing while you sleep?
- When you try to relax in the evening or sleep at night, do you ever have unpleasant, restless feelings in your legs that can be relieved by walking or movement?
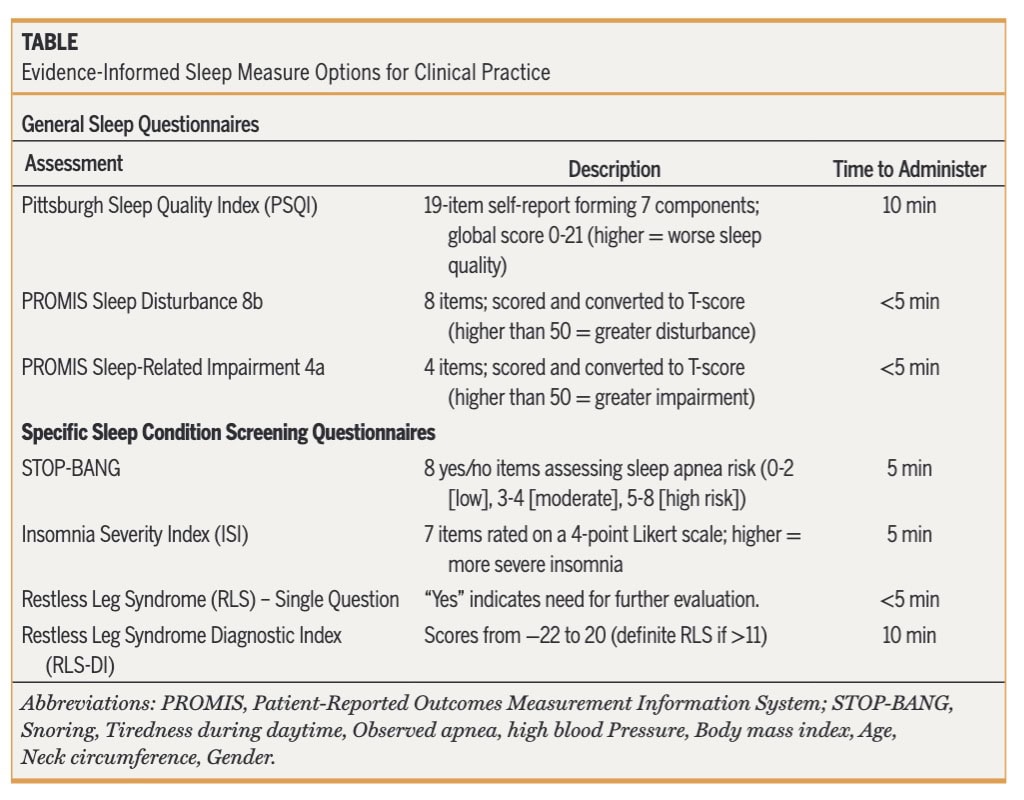
When the first 2 questions are answered with “yes”, it is advised to let the patient fill out the Insomnia Severity Index. A score of 15 or higher indicates clinical insomnia and warrants referral.
When Questions 1 to 3 are answered with “yes”, the STOP-BANG questionnaire can be used to screen for obstructive sleep apnea. It stands for:
- Snoring
- Tiredness during daytime
- Observed apnea
- High blood Pressure
- Body mass index > 35
- Age > 50 years
- Neck circumference (> 40cm)
- Gender (male)
Each “Yes” is given a point. A score of 3 or less can help rule out the presence of obstructive sleep apnea with a sensitivity of 77%, as highlighted by the authors. If it is suspected, referral is warranted for further evaluation.
When question 4 is answered positively, the authors advocate administering the Restless Leg Syndrome Diagnostic Index (RLS-DI). The RLS-DI consists of 10 items, and scores range from −22, representing no restless legs, to 20, representing definite restless legs. A score >11 is indicative of restless legs syndrome. Then we would have to figure out whether the musculoskeletal condition is contributing to the restless legs, for example, neuropathic pain. Referral to a physician for a diagnosis is warranted.
Questions and thoughts
One important aspect of implementing this pragmatic approach into practice is the patient-therapist relationship, as sleep dysfunctions may need to be addressed through some behavioral changes. In Part 2, we will focus on addressing sleep dysfunction in musculoskeletal pain management.
Sleep diaries may be a useful adjunct for objectifying the sleep disturbances, and the authors recommend their use over a week or two. But it must be said, these diaries are subjective and prone to recall bias and variability in accuracy. Also, compliance when the diaries have to be filled over a longer period of time is often not optimal. When administering a sleep diary, the Consensus Sleep Diary can be used; it is a free, expert-developed tool proven to be valid and reliable.
Commercially available wearable devices can also be used to give insights into the sleep patterns of patients with musculoskeletal pain and sleep problems. Being practical and more accessible than the gold standard polysomnography, nearly everyone can track their nightly sleep. Yet, it must be acknowledged that not every wearable device has been validated against the gold standard, and as such, we must remain cautious. Furthermore, the accuracy in detecting different stages of sleep is highly variable between devices. So, the use of wearable devices to track sleep can give an indication of sleep patterns, but it is recommended to use them alongside other assessment methods, such as sleep diaries.
If you detect sleep dysfunction related to musculoskeletal pain onset in a patient, you can use the proposed framework to refer for further investigation of the sleep pattern. We as physiotherapists are not responsible for diagnosing sleep dysfunctions, but we can help screen for them. Apart from the specific sleep screening questionnaires, a more general sleep assessment can be started. The authors recommend the use of the Pittsburgh Sleep Quality Index (PSQI) and the 4- or 8-Item PROMIS Sleep Disturbance Questionnaire. With respective times to administer these questionnaires reported to be under 5 minutes, the PROMIS seems to be worth including in practice to get a general idea of sleep in your patient.
Talk nerdy to me
Of course, this pragmatic approach is prone to some limitations, with the most obvious being the risk of introducing bias, as no systematic review process took place. So we don’t know how studies got included or excluded. It is like looking from the authors’ perspective, and inherently, that will already influence the pragmatic approach as presented. Do they see many people with sleep disorders or not? Are they in specialized care, with access to specialized tools and measurements?
The good part is that the clinical commentary focused on a pragmatic approach to help us in clinical practice. It doesn’t shift our scope of practice to become sleep experts; it is designed to help screen for sleep disorders related to musculoskeletal pain and act if necessary by referring.
Because this is a clinical commentary, the level of evidence is inherently lower than that of randomized controlled trials or systematic reviews. The methodology does not include a systematic search strategy, predefined inclusion criteria, or risk-of-bias assessment, which introduces the possibility of selection bias. In other words, the authors may have preferentially included studies that support their proposed framework, without transparently demonstrating how evidence was selected or weighted.
A strength of this approach is its high generalizability to clinical practice. The authors successfully translate complex and multidisciplinary evidence, spanning sleep medicine, psychology, and pain science, into a pragmatic, stepwise framework that can be readily implemented in physiotherapy practice. In summary, this paper provides a clinically valuable, theory-informed framework, but its conclusions should be interpreted with caution due to the lack of direct empirical validation, absence of systematic methodology, and reliance on secondary evidence.
Take-home messages
Sleep is not just a symptom; it actively drives pain and recovery. When patients report sleep disturbances, rather than just documenting that, we should go further and screen for potential underlying drivers of musculoskeletal pain conditions. The current framework helps us determine whether sleep dysfunction is present and, if so, to what extent. The framework itself is proposed as a screening tool, not a diagnostic tool. If sleep dysfunction is identified and considered as a factor underlying the development of or persistence of the musculoskeletal pain condition, we should refer the patient for further assessment by sleep experts.
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Watch this FREE video lecture on Nutrition & Central Sensitisation by Europe’s #1 chronic pain researcher Jo Nijs. Which food patients should avoid will probably surprise you!
