Research
Exercise
March 19, 2026
Who Benefits Most? Moderating Factors for Running-Induced Disc Adaptations in People with Chronic LBP

Introduction
In an earlier research review, we discussed the ASTEROID randomized controlled trial (RCT) by Neason et al. (2024), which explored the safety and efficacy of running as a treatment for chronic non-specific low back pain (LBP) in adults aged 18-45. It compared a 12-week progressive run-walk interval training program to a waitlist control group. The study found significant reductions in pain intensity and disability within the running group compared to controls, although the observed between-group improvements were not enough to be considered clinically relevant. The trial, however, confirmed the intervention’s safety and feasibility, with minimal adverse events and high adherence, challenging the stigma that running is unsafe for people with LBP. This provided a basis for future studies to optimize running-based interventions for people with chronic LBP.
Mostly, people think that running can cause harm, especially by increasing the demands on the spine and intervertebral discs (IVDs). The ASTEROID trial, however, confirms that chronic LBP is not worsened in people participating in such a running program.
Emerging evidence from animal and in vitro studies even suggests that mechanical loading can influence disc biology through mechanotransduction. Cross-sectional data show that runners tend to have healthier discs. However, to date, only two RCTs have examined exercise effects on IVDs, and the results are inconsistent, partly due to poor adherence and heterogeneous interventions.
As the feasibility of running was confirmed earlier, the follow-up question of the authors from the ASTEROID trial was whether it was feasible for everybody to participate. The current study, therefore, is a pre-planned secondary analysis that dives into pre-defined subgroups to examine whether patient factors (such as baseline IVD status, sex, or body mass index) and intervention factors (such as speed, volume, and surface) moderate the effects of the running program on IVD health in adults with non-specific CLBP. Because we don’t know how to dose loading (volume, speed, surface), and because it is also unclear whether degenerated discs can still adapt positively, this study addresses a key gap in understanding running-induced disc adaptations. It questions which patient and exercise factors influence whether running improves disc health? The results will help determine if some patients benefit more from the running intervention than others, and guide the mode of exercise prescription for IVD health.
Methods
This was a pre-planned secondary analysis of the ASTEROID (A 12-week run-walk intervention) randomised controlled trial (RCT), which we covered in a previous research review. The RCT included adults aged 18–45 years with chronic non-specific low back pain (LBP) for at least 3 months, who were not regular runners and were injury-free in the lower limbs. They followed a 12-week, progressive run-walk interval training program, prescribed by an exercise physiologist and delivered via the Runkeeper app. Participants completed three weekly 30-minute sessions, with starting levels (15-, 30-, or 45-second run intervals) based on an initial 2-minute treadmill run test. The program was unsupervised but included weekly or bi-weekly video calls for support and guidance.
They were compared to a control group, which was a waitlist control. The control participants were asked to manage their LBP as usual and avoid running, and were offered the program after 12 weeks. Primary outcomes were pain intensity and disability, assessed at baseline, 6, and 12 weeks. The study also examined the safety of the running intervention.
This secondary analysis had the purpose to identify patient and intervention factors that moderate the effects of a running program on intervertebral disc (IVD) health in adults with non-specific chronic low back pain (CLBP). IVD health was defined by the structural and functional integrity of the disc, characterized by preserved hydration, disc height, and collagen composition.
The primary outcome, IVD health, was assessed using whole-disc T2 Magnetic Resonance Imaging (MRI) at the levels from T11/T12 to L5/S1. The measurements were obtained at baseline, 6, and 12 weeks. Higher T2 values indicate higher hydration and better IVD health. The participant’s habitual physical activity was assessed using the International Physical Activity Questionnaire (IPAQ). Pain was assessed using the 100-point VAS scale and disability was recorded using the Oswestry Disability Index (ODI).

Potential moderators were examined:
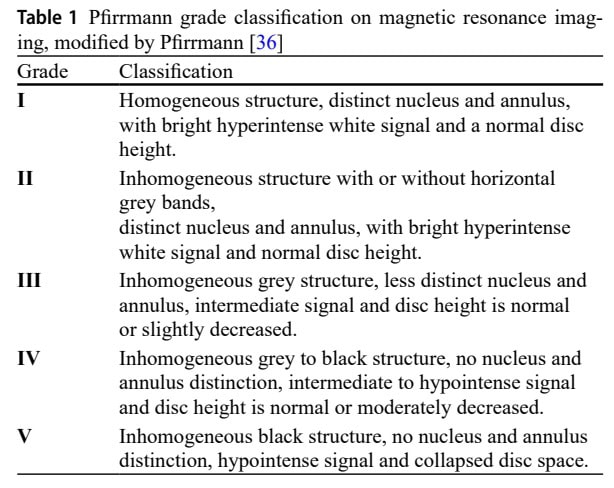
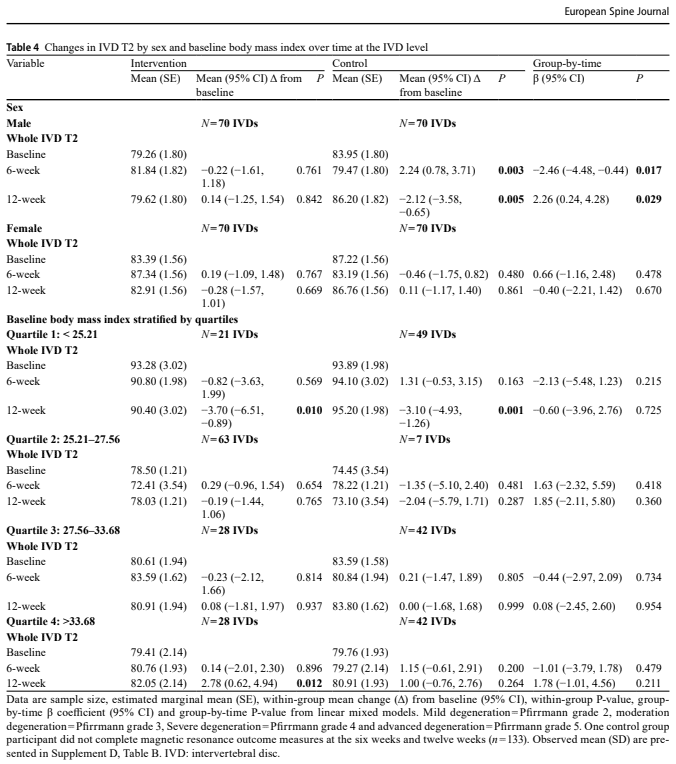
- Patient Factors: Baseline degeneration (Pfirrmann grade; aggregated Pfirrmann score), sex (male, female), and Body Mass Index (BMI). The Pfirrmann grade is a classification system to visually assess the degree of (IVD) degeneration using MRI. It grades the discs from one (healthy) to five (severe degeneration) based on changes in IVD structure, the distinction between the nucleus and annulus, signal intensity brightness, and disc height. The Pfirrmann grading was one of the patient factors used in the study to classify baseline IVDs into subgroups (normal, mild, moderate, severe, and advanced degeneration) for analysis.
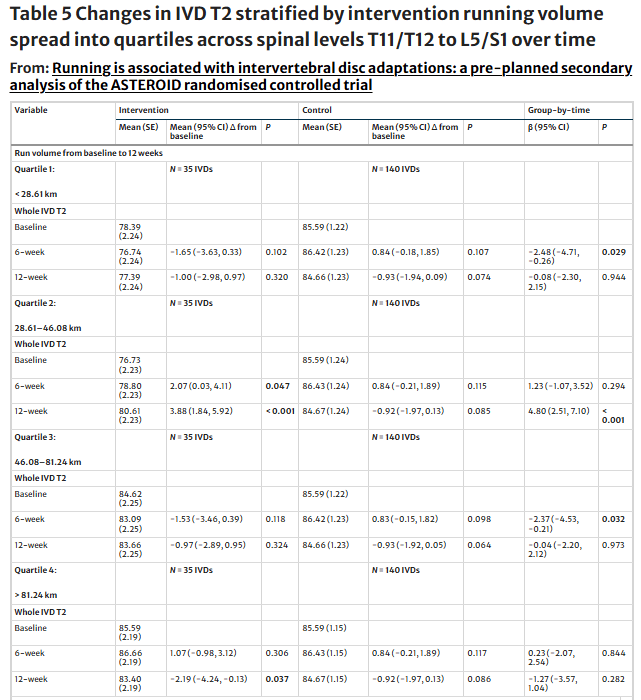
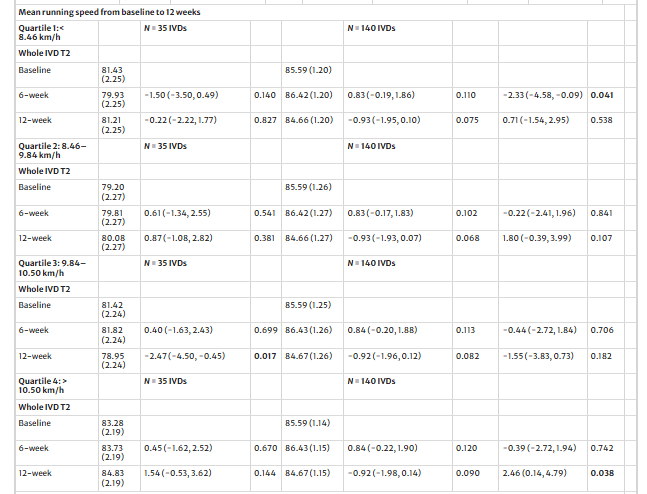
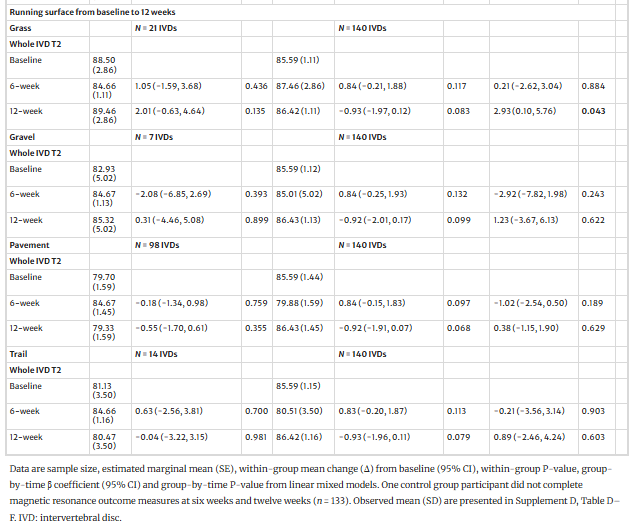
- Intervention Factors: Cumulative running volume, mean running speed, and dominant running surface (grass, gravel, pavement, or trail) were assessed using the free Runkeeper application. Cumulative running volume and mean running speed were stratified into IVD quartiles for analysis from baseline to 12 weeks. All intervention moderators were compared with the control sample.
Results
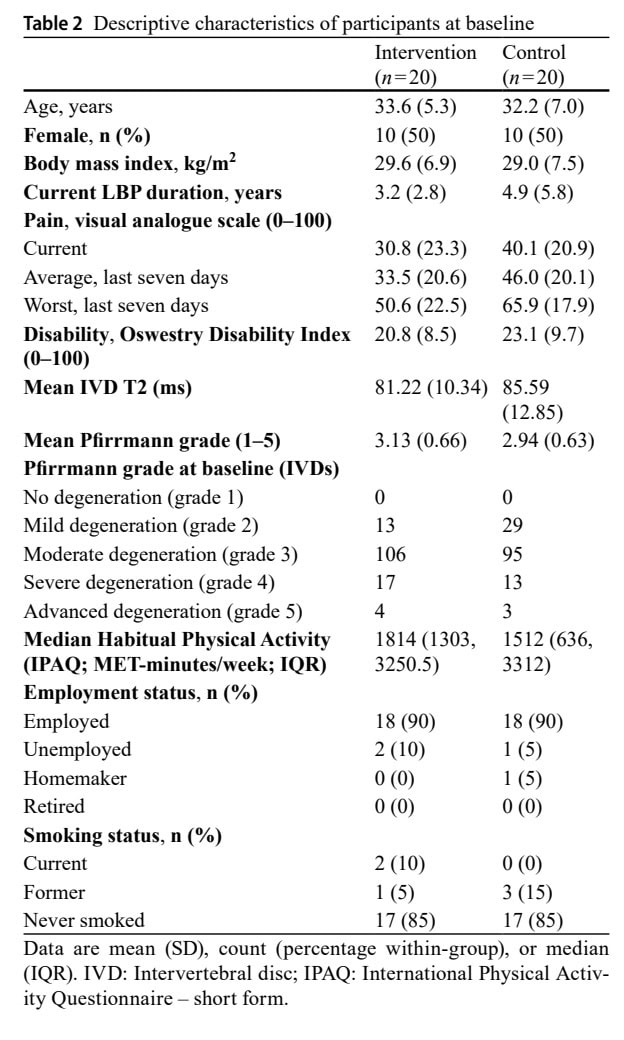
Forty adults with chronic nonspecific low back pain were included. The sample was equally divided into males and females.
The analysis of patient factors showed that when IVDs were stratified by baseline Pfirrmann grade, IVDs with mild degenerative changes negatively moderated the between-group IVD T2 changes at 6 weeks, but not at 12 weeks.
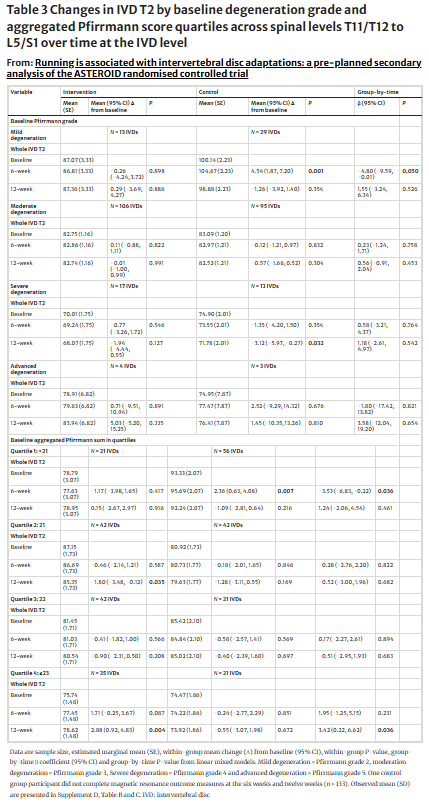
Aggregated Pfirrmann scores were also stratified into quartiles, yielding 4 groups that represent increasing levels of degenerative changes. At 6 weeks, At six weeks, aggregated Pfirrmann<21 (quartile one) negatively moderated between-group IVD T2. At 12 weeks, aggregated Pfirrmann≥23 (quartile four) positively moderated between-group IVD T2. No other quartile or time point revealed between-group changes.
Looking at the intervention factors, cumulative running volumes between 28.6 and 46.1 km positively moderated between-group IVD T2 at 12 weeks. Whereas cumulative running volumes less than 28.6 km or between 46.1 and 81.2 km, negatively moderated IVD T2 between-group, however, only at six weeks. Six- to 12-week running volumes less than 14.8 km positively moderated IVD T2 between-group at 12 weeks only.
Mean running speeds from 10.5 to 11.7 km/h positively moderated between-group IVD T2 at 12 weeks. Whereas mean running speeds between 4.4 and 8.5 km/h negatively moderated IVD T2 at six weeks only. Running on grass positively moderated between-group IVD T2 at 12 weeks.
Questions and thoughts
One of the first questions I had when reading this paper was why the authors focused on the intervertebral disc in this chronic nonspecific low back pain sample. The nonspecific low back pain itself assumes that no underlying serious driver is causing the pain, such as a tumor, infection, or fracture. Yet, it does not mean the patient’s spine lacks any anatomical variation or changes.
The authors also highlighted this in their discussion, but they still argue two valid reasons for conducting this research.
- A Highly Prevalent Co-Finding: Research shows that individuals with CLBP—even the non-specific kind—are more likely to have IVD changes (often called “degeneration” on MRI) compared to people who don’t have pain. The study is investigating this highly prevalent association and references a systematic review of 2015
- The authors hypothesize that the IVD, as a mechanically loaded tissue, retains the capacity to adapt and improve its hydration and composition in response to a physical stimulus such as running. By studying this, the researchers shift the focus from the IVD as a static source of pathology to a dynamic structure with potential for positive adaptation.
In short, they aren’t claiming that running is fixing the cause of the pain, but rather that it can improve a highly correlated structural factor that might be contributing to the overall clinical picture, and they want to know the optimal “dose” for this positive adaptation. Therefore, they want to examine if IVD changes act as a moderator for the effect of exercise. They are asking: “Does this running program work better, worse, or the same for a patient with severe degeneration compared to a patient with mild degeneration?” This shifts the focus from asking “Is the IVD the cause of pain?” to “Is the state of the IVD the key to how we prescribe exercise?
Talk nerdy to me
The study used linear mixed models with random effects for both participant and spinal level, which appropriately accounts for repeated measures and clustering of multiple discs within individuals, increasing statistical robustness. An intention-to-treat approach was applied, preserving randomisation and reducing bias, although subgroup (quartile) analyses likely reduced power and increased risk of type I error. Adjustment for individual baseline characteristics did not change the results of any primary analyses.
Because this was a secondary analysis of a feasibility RCT, the current results can give insights for further research, but are not conclusive (yet). The moderator analyses were exploratory, meaning the significant findings (e.g., optimal running volume or speed) should be interpreted as hypothesis-generating rather than definitive. Notably, intradiscal loading was not directly measured, so conclusions about mechanotransduction remain inferential.
Clinically, this raises questions about whether observed T2 changes truly reflect meaningful biological adaptation or transient fluid shifts within the disc. Better IVD health status was defined by the authors, but it doesn’t automatically mean that someone just got rid of their CLBP. Also, the authors acknowledge that, although positive IVD changes were observed in the intervention group, these did not yield statistically significant differences between the runners and the control group.
The run-walk intervention was designed to be conservative, resulting in a wide variation in mean running speeds (4.4 to 11.7 km/h) and cumulative running volumes (1.8 to 109.8 km). While this provided an opportunity for subgroup analysis, it reflects high variability in the actual ‘dose’ of running.
BMI did not appear to moderate changes in IVD T2 at any time point, suggesting that body mass may not meaningfully influence how discs respond to this type of graded running load in individuals with CLBP. This is somewhat surprising given prior evidence linking higher BMI to increased spinal loading, and may indicate that the relatively low running volumes in this study were insufficient to expose BMI-related differences. In contrast, sex showed a time-dependent moderating effect: males demonstrated a negative effect at 6 weeks but a positive effect at 12 weeks compared to controls, whereas females showed no significant moderating effect. However, the authors note that early negative changes in males were likely driven by changes within the control group, raising the possibility that these findings reflect variability rather than a true physiological difference. For clinicians, this suggests that sex-specific responses to loading remain unclear and should not yet drive different exercise prescriptions, while BMI alone may not be a key factor when prescribing low-to-moderate running interventions for disc health.
Take-home messages
Degeneration level matters: Those with more degenerative changes in their IVDs (highest quartile) showed improved IVD health at 12 weeks, whereas those with mild degeneration showed a negative effect at 6 weeks, which was not sustained at 12 weeks. Together, this suggests that more degenerative changes at baseline may hold more capacity to improve.
Running volume shows a “sweet spot”: Based on the current analysis, the optimal range would lie between 28.6–46.1 km over 12 weeks, which is approximately 2.4–3.8 km/week. Too little or too much showed a U-shaped relationship between load and adaptation, with negative effects, mainly at 6 weeks.
Running speed and surface matters: Best outcomes were achieved with running speeds between 10.5–11.7 km/h. Running on a grass surface also yielded a positive IVD effect. BMI did not show any moderating effect.
This was a small (n=40), secondary subgroup analysis with multiple comparisons, meaning the study was not adequately powered to detect moderator effects. The use of quartiles further reduced subgroup sizes, increasing the likelihood that some statistically significant findings (e.g., “optimal” running volume or speed) may be due to chance rather than true physiological effects. As a result, conclusions about running-induced disc adaptations should be interpreted cautiously, as these findings are hypothesis-generating rather than prescriptive, and it would be premature to base specific clinical loading guidelines on them without confirmation from larger, adequately powered trials.
Reference
100% FREE POSTER PACKAGE
Receive 6 High-Resolution Posters summarising important topics in sports recovery to display in your clinic/gym.