Research
Diagnosis & Imaging
March 30, 2026
It’s Not All About The Surgery: Preoperative Muscle Condition and Lumbar Discectomy Outcomes

Introduction
Lumbar disc herniations occur frequently and sometimes require surgical management. We’ve all come across that patient in whom the surgery seemed perfect, but still, they did not reach a fully functional recovery. Or that patient who had a relapse of their pain after a lumbar discectomy. Emerging findings have proposed a link between the condition of key lumbar muscles before the operation and postoperative outcomes, calling for the need for a synthesis of the existing literature. Therefore, the current study took a closer look at preoperative muscle condition and lumbar discectomy outcomes.
Methods
This systematic review and meta-analysis was conducted according to the PRISMA guidelines and registered in PROSPERO. Studies investigating adult participants with imaging-confirmed lumbar disc herniation who underwent lumbar discectomy or decompression surgery were included when a preoperative assessment of the lumbar paraspinal muscles took place. On this imaging, an assessment of fatty infiltration, atrophy, or other graded indicators of muscle degeneration had to be determined. Eligible studies also included at least one postoperative clinical outcome.
Studies were excluded in case of other lumbar conditions present (such as isolated lumbar spinal stenosis, spondylolisthesis, infection, fracture, etc), rather than “pure” lumbar disc herniation.
The authors pooled multivariable-adjusted Odds Ratios (ORs) for dichotomous outcomes (recurrence/reoperation and chronic LBP), and pooled unadjusted mean differences (MD) for continuous functional outcomes using random-effects models.
Results
Thirteen observational studies, including a total of 4,371 patients, were included in the systematic review and meta-analysis. The studies were published between 2018 and 2025. All studies assessed preoperative paraspinal muscle fatty infiltration using magnetic resonance imaging (MRI).
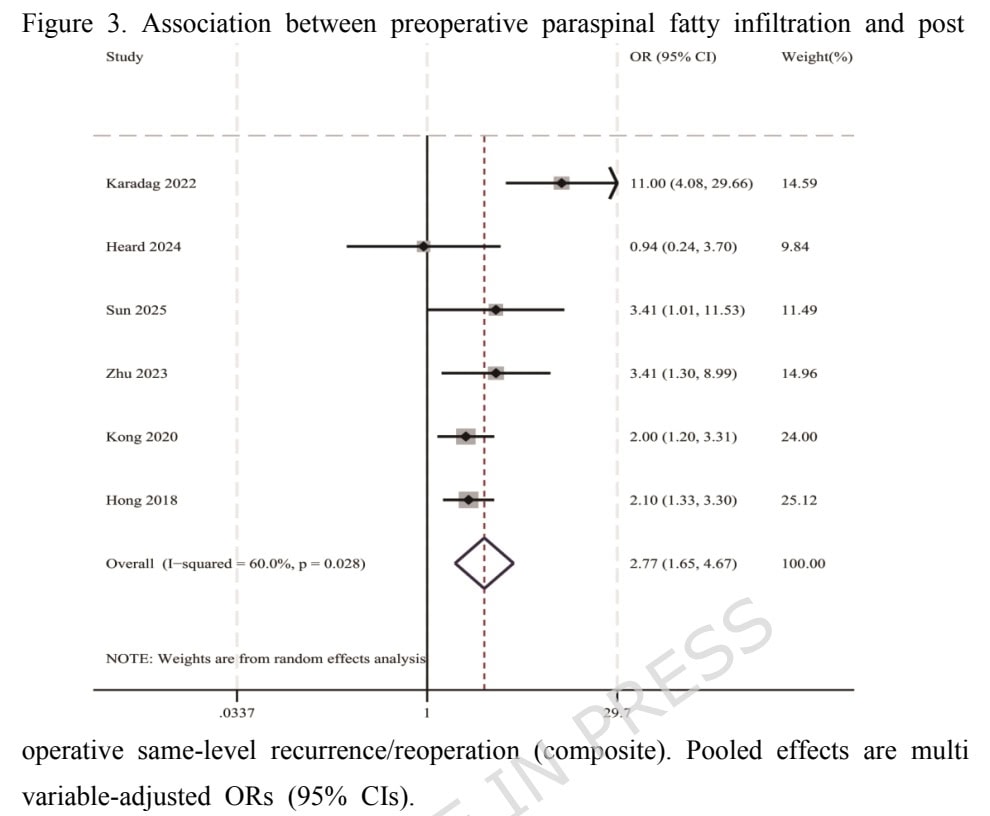
Six studies were included in the meta-analysis for the outcome of same-level recurrence or reoperation (n= 2,352 patients). All studies compared recurrence risk between patients with higher preoperative paraspinal fatty infiltration/degeneration and those with no or mild degeneration. The random-effects meta-analysis showed a significant association between more severe preoperative paraspinal fatty infiltration and a higher risk of same-level recurrence or reoperation with a pooled OR = 2.77 (95% CI: 1.65 to 4.67).
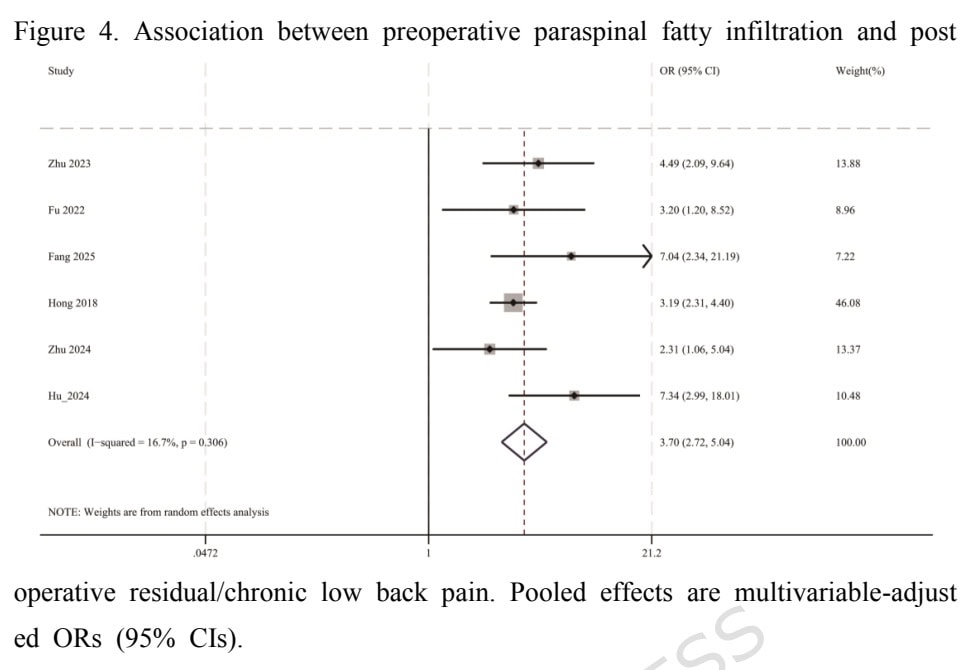
The meta-analysis on the association between paraspinal muscle fatty infiltration and residual or chronic low back pain included 6 studies. A significant association was found with a pooled OR = 3.70 (95% CI 2.72 to 5.04).
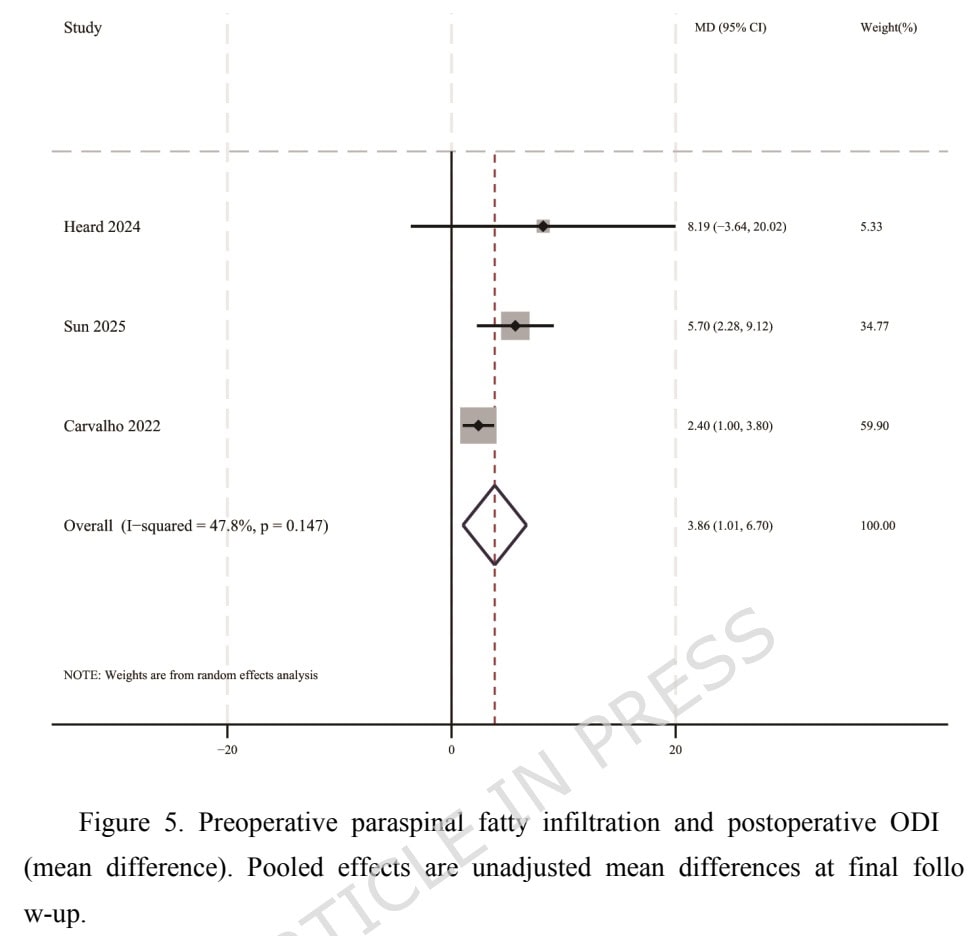
The association between the paraspinal muscle fatty infiltration and poor outcomes after surgery was examined by 3 studies. All studies used the Oswestry Disability Index (ODI). The association was significant with the pooled MD = 3.86 points (95% CI 1.02 to 6.70).
Questions and thoughts
Lumbar discectomy is a type of surgery where nerve roots are decompressed, and it is performed in patients with radicular pain whose symptoms persist or recur despite adequate conservative management, leading to the question of what constitutes adequate management. In patients with lumbar disc herniation, conservative management should be the first-line approach unless serious neurological deficits are present, as recommended by a consensus statement from the World Federation of Neurosurgical Societies (WFNS) Spine Committee. This recommendation is based on a systematic review and expert agreement, highlighting that most patients improve without surgery, with spontaneous regression occurring in 60–90% of cases.
They argue that effective conservative care combines activity modification, pharmacological support, particularly NSAIDs for short-term pain relief, and physiotherapy. Within physiotherapy, extension-based exercises and postural strategies appear beneficial, while prolonged bed rest and passive treatments show limited value. The Committee also points out that interventions such as injections may provide short-term symptom relief but do not improve long-term outcomes. Overall, they argue that a multimodal, active rehabilitation approach offers the best chance for recovery in the majority of patients. If, only after trying conservative care when no deteriorating neurological symptoms appear, the patient is still not getting better, only then can surgical options be explored.
The relationship between paraspinal muscle fatty infiltration and poor outcomes, documented by the Oswestry Disability Index (ODI), showed a significant association, with the pooled MD = 3.86 points (95% CI 1.02 to 6.70). Although significant, we must acknowledge that the minimal clinically important difference (MCID) was not attained, as this MCID is reported to range between 10 and 12.8 points. A recent study found that at 3 months post-lumbar discectomy, the MCID for the ODI is significantly lower when anchored to improvement in leg pain (6 points) than in back pain (15 points), indicating that smaller ODI improvements are deemed meaningful when leg symptoms are the focus. In light of these findings, the current study may have had some patients with improved ODI function and some without, but we can assume that the target improvement score for patients with radicular pain complaints in their leg may lie somewhat lower than previously thought.
Talk nerdy to me
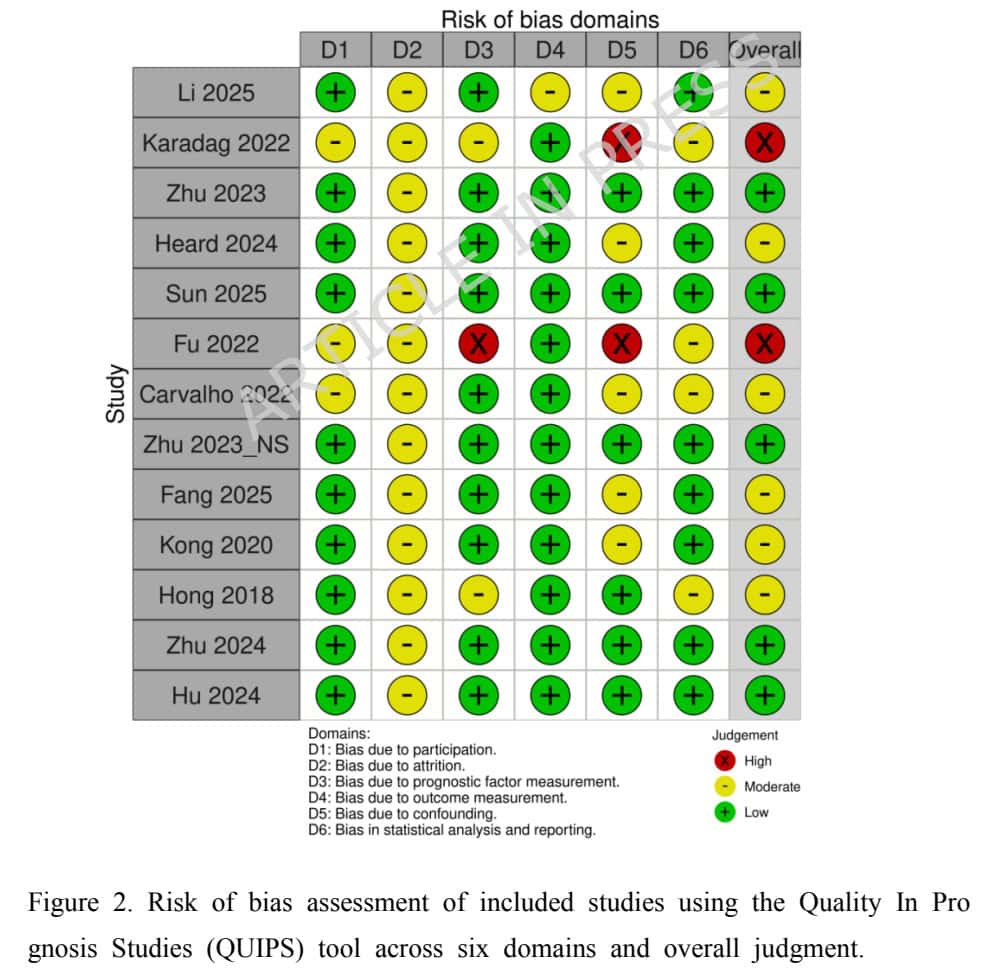
Six of the thirteen studies were low risk of bias, five were rated as moderate risk, and two as high risk of bias. Most of the studies were downgraded because of inadequate control for confounding variables and the insufficient reporting of follow-up/attrition. As we know, pain is not a simple equation, and therefore, only considering paraspinal muscle fatty infiltration as a contributor to postoperative outcomes is too narrow. Yet, due to the mostly retrospective designs of the studies included, confounding factors may have been missed or not consistently measured across studies. For example, psychological factors such as kinesiophobia, baseline symptom severity, smoking status, etc. All these factors may have a spell on postoperative outcomes, and when not balanced across the meta-analysis, the observed effect may be influenced.
For example, smoking status was only variably included as a confounder across the 13 studies. In epidemiological terms, if a study on preoperative muscle condition and lumbar discectomy outcomes does not adjust for smoking, it cannot definitively say that the muscle quality is the reason for the failure. It might just be that poor muscle and poor surgical outcomes are both “downstream” effects of a smoking habit. The authors acknowledged this and proposed to use fatty infiltration as a prognostic phenotype variable, rather than as a distinct prognostic factor. In this light, we can look at fatty infiltration as a negative prognostic phenotype variable that fits within a “red flag” cluster of patients who are overweight, smokers, not sufficiently active, who may have less potential for optimal postoperative outcomes, regardless of how well the surgery was performed.
Definitions of fatty infiltration differed acrosee studies and this variance may be reflected in the confidence intervals. Yet, sensitivity analyses were conducted and showed that the pooled estimates were robust for all outcomes. For recurrence/reoperation, excluding any single study yielded pooled ORs ranging from 2.14 to 3.11, with consistent direction and 95% CIs that did not cross 1. For residual/chronic low back pain, pooled ORs remained between 3.34 and 4.22 after excluding any study, and results remained statistically significant. For functional outcomes (continuous measures), the pooled effect estimates after excluding each study individually all remained above the null value, suggesting that the functional outcome results were not driven by any single study.
Take-home messages
Preoperative muscle condition in lumbar discectomy is associated with postoperative outcomes. Those with preoperative fatty infiltration in the paraspinal muscles have a greater risk of achieving less favorable postoperative outcomes.
The strong association between preoperative muscle condition and lumbar discectomy outcomes means that patients with severe FI are significantly more likely to:
- Need another surgery or have the disc problem return (recurrence/reoperation).
- End up with long-term, residual, or chronic low back pain.
- Have a poorer overall functional recovery.
Therefore, some patients need more than just surgery, they need intensive, counseling and rehab to address the negative cluster of inactivity and poor muscle quality. This may help preoperative counseling and management of surgery expectations on one side, but can also help engage in proper postoperative rehab and exercise participation on the other hand.
Acknowledgement of the prognostic associations as guides, needs us mentioning the limitation that fatty infiltration itself is not proven to be the single cause of poor postoperative outcomes.
Reference
100% FREE POSTER PACKAGE
Receive 6 High-Resolution Posters summarising important topics in sports recovery to display in your clinic/gym.