Elbow Assessment

Learn
Elbow Assessment
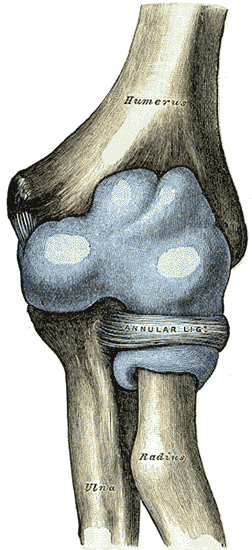
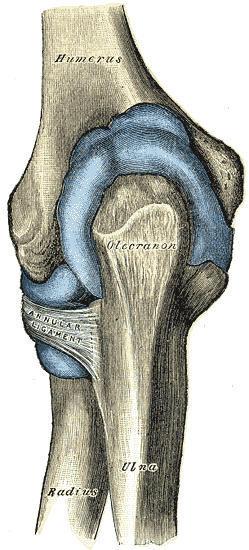
The elbow joint consists of three different bones enclosed in a single capsule: the humerus, the ulna, and the radius.
The humeroulnar joint is a simple hinge joint, which only allows flexion and extension between the trochlea notch of the ulna and the trochlea of the humerus.
The humeroradial joint is a ball-and-socket joint with the concave socket on the radius and the convex side on the capitulum of the humerus.
At last, the proximal radioulnar joint is a pivot joint that enables rotation of the forearm, called pronation and supination.
Epidemiology
The point prevalence of elbow pain in the general (Dutch) population is 7.5%. The authors also report a 12-months prevalence of 11.2% with chronic pain in 5.3% of cases. Throughout the age groups, the prevalence of elbow pain increases gradually until it peaks in the age group between 45-64 years of age after which it drops only slightly. Regarding sexes, women have a slightly higher prevalence throughout all age groups compared to men (8.7% vs. 6.2%) (Picavet et al. 2003).
Course
Bot et al. (2005) conducted a prospective cohort study in 181 patients with elbow complaints in general practice. They found the following outcomes:
Elbow pain has an unfavorable prognosis with only 13% reporting full recovery at 3 months follow-up and a low 34% after 12 months.
At the same time, 90% of patients reported at least some improvement after 1 year follow-up.
The average baseline pain score of 5.3 (±2.1) decreased by 1.3 (±2.3) points at 3 months and 2.1 (±2.6) points at 12 months. At the same time, baseline disability with a score of 34.6 (±20.4) decreased by 6.3 (±16.2) points at 3 months and by 11.9 (±21.2) points after 1 year.
The 1-year recurrence was as high as 54%.
Prognostic factors
In the prospective cohort study of Bot et al. (2005) the following factors were associated with a negative prognosis for recovery (pain and disability) at 3 and 12 months follow-up:
– Longer duration of complaints before consulting the GP
– Having additional musculoskeletal comorbidity
– Usage of the coping strategy ‘retreating’
– Less social support (at 3 months only)
– History of elbow complaints (at 12 months only)
– ‘Worrying’ as a coping style (at 12 months only)
Red flags
Fractures
Radial head fracture or fracture of the olecranon after trauma resulting in constant pain at rest/night, pain at palpation, axial loading, vibration
You can use the elbow extension test to screen for elbow fractures:
Dislocation
Fall on the outstretched hand, trauma, deformity (appears elongated or shortened) (Waymack et al. 2018)
Osteochondritis dissecans/loose bodies
Repetitive trauma, crepitation, locking, decrease in active and passive range of motion (van Sonhoven et al. 2009, Ligon et al. 2014)
Distal biceps tendon ruptures
Prolonged (cortico)steroid use, activities like weightlifting and bodybuilding, trauma with audible and painful pop, swelling and ecchymosis, weakness in flexion, supination (Thomas et al. 2017)
A test you can use for the assessment of distal biceps tendon ruptures is the Hook test:
Distal triceps tendon ruptures
Prolonged (cortico)steroid use, activities like weightlifting and bodybuilding, trauma with audible and painful pop, swelling and ecchymosis, inability to actively extend the elbow (Thomas et al. 2017)
Tract anamnesis:
Referred pain from the organ systems usually refers to more proximal locations like the trunk, hip, or shoulder. For this reason, there is no tract, which has to be considered as a possibility to display as elbow pain.
Apart from red flags that warrant (urgent) referral to a specialist or GP, other sources of pain referral have to be considered.
Mainly radicular pain from the cervical spine should be excluded during the anamnesis and physical examination.
Basic Assessment
After visual assessment of the elbow including palpation, you should assess active range of motion in the affected and unaffected elbow.
Watch the following video to learn which movements should be assessed and look for pain during motion, restricted range of motion as well as compensation.
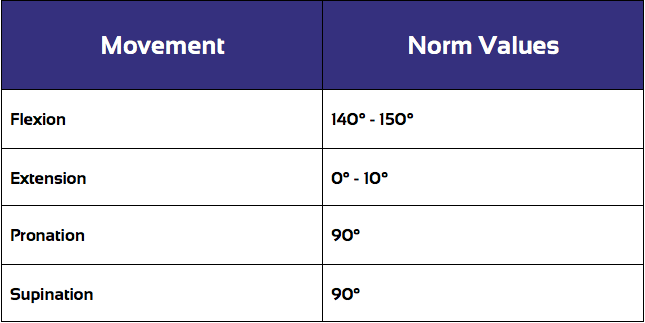
In order to be able to judge a limited range of motion, the affected elbow should be compared to the unaffected side. On top of that, compare the observed ROM to the standard values in different directions. These are:
AROM assessment is then typically followed by Passive Range of Motion Assessment (PROM) which you can watch with a click on the following video:
During PROM assessment, it’s important to compare the range of motion as well as the end-feel of the affected elbow with the unaffected side.
Another part of the basic assessment is functional assessment. You should ask your patient to perform the activities that he is having problems with daily living.
This way, you might be able to observe for awkward movement, pain during movement, and compensating strategies similar to AROM assessment.
As the last step resisted isometric testing can be useful in order to stress the muscles that cross the elbow joint including the respective tendons.
The following video shows you how to perform isometric testing:
In the following learning units, we will further specify which underlying pathologies can present in the elbow joint and how to assess them.
Specific Pathologies in the Elbow
There are several pathologies that are commonly seen in the elbow area. For more information, click on the respective pathology (content will be added in the near future):
- Posterolateral Rotatory Instability (PLRI)
- Collateral Ligament Injury
- Epicondylalgia (Tennis and Golfer’s Elbow)
- Proximal Biceps Tendon Ruptures
- Distal Biceps Tendon Ruptures
- Ulnar Nerve Entrapment
References
Ligon CB, Gelber AC. Elbow loose bodies. The Journal of rheumatology. 2014 Jul 1;41(7):1426-7.
Thomas JR, Lawton JN. Biceps and triceps ruptures in athletes. Hand clinics. 2017 Feb 1;33(1):35-46.
Accredited online physiotherapy courses
- Built by the experts at Physiotutors
- Best price per CEUs/CPD Points
- Accredited in the Netherlands, Belgium, Germany, USA, UK, & Australia
- Learn anywhere, any time, and at your own pace!





Download the free Physiotutors app now!



