Thoracic Outlet Syndrome | Diagnosis & Treatment for Physios
Clinical Picture & Examination
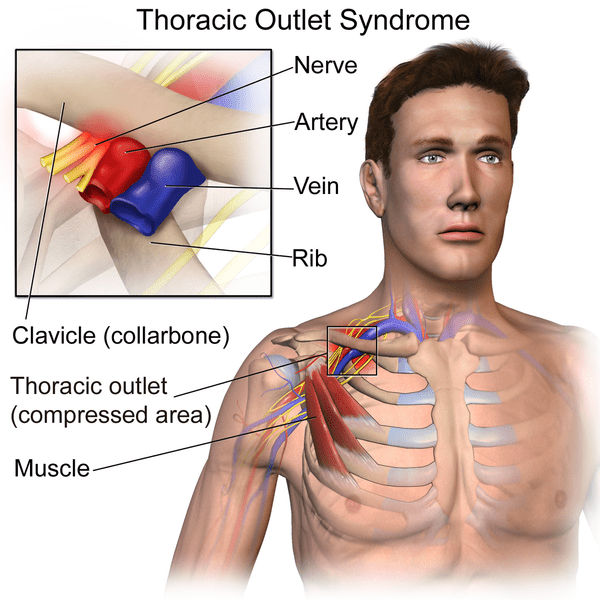
It is essential that the clinician carefully considers and at least attempts to clinically differentiate, where possible, exactly which component of the neurovascular complex is being affected and precisely where it is being compressed. This will dictate not only which further investigations are required, but may well impact on what is the most appropriate treatment strategy. In reality, this is often easier said than done (Watson et al. 2009). Unfortunately, there is no test or investigation that is able to consistently prove the diagnosis of TOS.
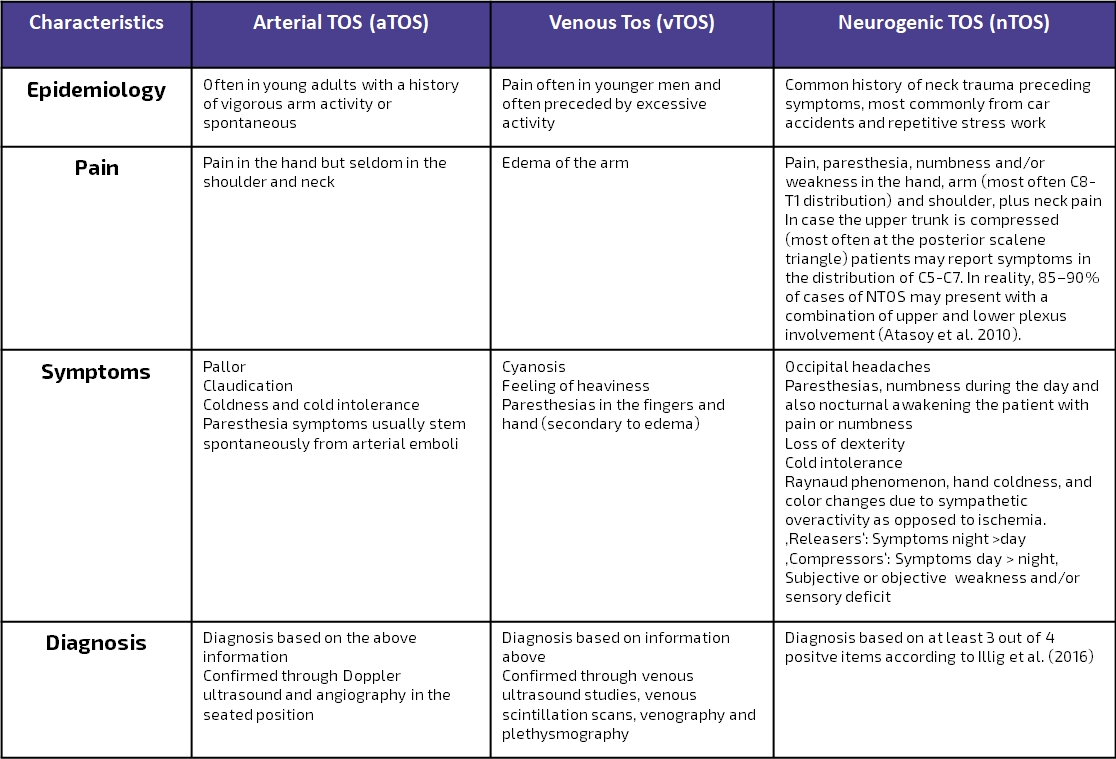
The following table is a modern adaption of Hooper et al. (2010) and presents an overview of the presentation of venous, arterial, and neurological TOS:
Due to the confusion around a clear definition of nTOS, Illig et al. (2016) of the Society for Vascular Surgery published reporting standards for TOS with the primary aim to provide a clear and consistent understanding and definition of what constitutes a diagnosis of nTOS. Watch the video below, to learn more about the consensus criteria:
Examination
In the following, we will explain how to use physical examination to confirm or reject the 3 criteria that you may have found during patient-history taking following the suggestions from Illig et al. (2016). The fourth criterion – a test injection – is outside of the scope and not feasible for a physiotherapist. The diagnosis of nTOS is confirmed if all 3 remaining items are positive:
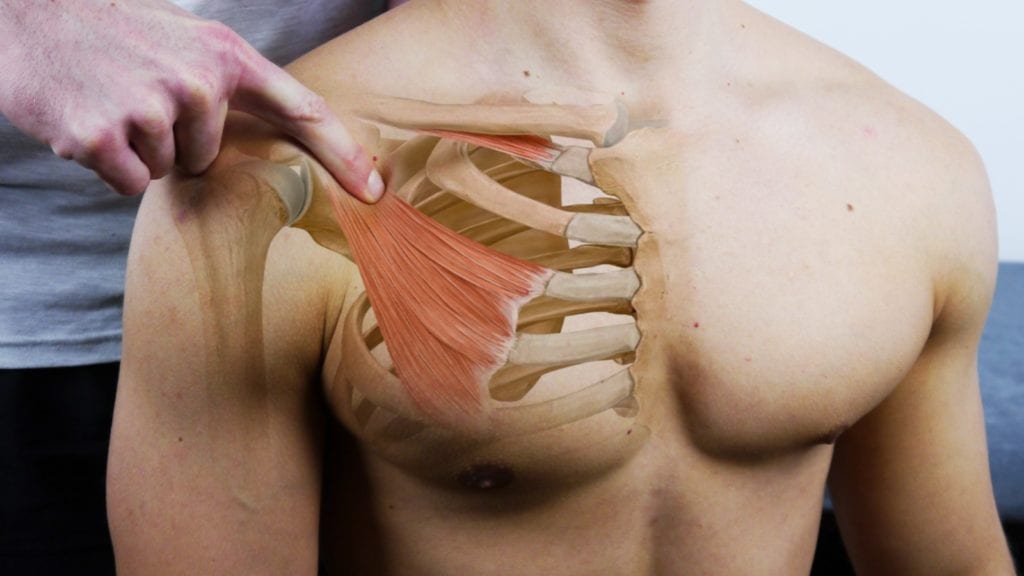
1) Local findings can be confirmed by tenderness upon palpation of the scalene triangle and pectoralis minor insertion.

2) Positive Peripheral Findings
Upper limb tension testing is sensitive for irritation of the neural tissue including cervical roots, brachial plexus, and peripheral nerves as well as for patients with arm pain syndrome. It has been advocated for the diagnosis of neurogenic TOS with reported high sensitivity. The test appears to be excellent for screening for sensitization of the neural tissue in the cervical spine, brachial plexus and upper limb but is not specific for one area. The test is recommended as part of the examination and for its usefulness in treatment that includes neural mobilization (Hooper et al. 2010).
There are several provocation tests for TOS that are designed to stress one of the 3 possible intervals for entrapment. These are:
- Roos / Elevated Arm Stress Test (All 3 intervals)
- Cyriax Release Test (All 3 intervals)
- Adson Test (Posterior Scalene Triangle)
- Eden Test (Costoclavicular Space
- Wright’s Test in 180°(Costoclavicular Space)
- Wright’s Test in 90° (Retropectoralis minor space)
3) Absence of other likely diagnoses
The physical examination of TOS is frequently long and complex as the clinician needs to examine the entire upper limb and cervical spine. Not only is a neurological examination required, but frequent peripheral nerve entrapment tests also need to be performed. In a substantial number of patients initially diagnosed with TOS, either radiculopathy or neuropathy is the eventual diagnosis. In more than 60% of patients referred to vascular surgeons for a TOS surgery, an alternate diagnosis was established (McGillicuddy et al. 2004). So the diagnosis of TOS should be only considered after the exclusion of cervical radicular syndrome and peripheral neuropathy. If you are unsure how to diagnose cervical radicular syndrome and how to distinguish it from peripheral nerve entrapment, we’d like to refer you to the chapter on cervical radicular syndrome.
There are many causes of similar pain symptoms, including rotator cuff tears, subacromial bursitis, adhesive capsulitis (so-called frozen shoulder), glenohumeral impingement syndromes, and lateral epicondylitis (tennis elbow). None of these, however, will manifest neurological abnormalities. Thus, a neurological evaluation will narrow this diagnosis to radiculopathy, neuropathy, or TOS (McGillicuddy et al. 2004). In the following video we will explain which characteristics distinguish TOS from similar diagnoses like cervical radicular syndrome of C6-8 and median or ulnar neuropathy:
MASSIVELY IMPROVE YOUR KNOWLEDGE ABOUT LOW BACK PAIN FOR FREE