Rotator Cuff Related Shoulder Pain | Diagnosis & Treatment

Clinical Presentation & Examination
More than 80% of shoulder pain is classified as rotator cuff-related shoulder pain (Ostör et al 2005). According to the 2022 clinical guidelines, rotator cuff tendinopathy encompasses subacromial pain syndrome, rotator cuff-related shoulder pain, subacromial impingement syndrome, subacromial bursopathy, long head biceps tendinopathy, and partial thickness rotator cuff tear (Lafrance et al 2022). In this article, RCRSP is seen as an overlapping diagnosis, and synonymous with rotator cuff tendinopathy.
To classify as one of these conditions pain should be broadly over the deltoid and upper arm region. The pain will be activity-related and worse with overhead or behind-the-back reaching. Pain in the neck, reproduction of shoulder pain with neck movements, and distal neurovascular symptoms reduce suspicion. Changes in occupation and participation – rather than nature alone – might raise the index of suspicion.
When doing your clinical examination, there should be no significant loss of passive range of movement, particularly in external rotation. Familiar pain should be reproduced with resisted abduction and/or lateral rotation. Assessment of sleep, nutrition, alcohol, physical activity, and smoking should be done with the promotion of change where relevant (Littlewood et al 2019).
Orthopedic tests
Most diagnostic tests for the shoulder are unreliable or not validated and combining provides little use for clinical practice (Hegedus et al 2012). However, in the clinical practice guideline by Lafrance and colleagues, there are several recommendations — although caution is required. These are seen in the bullet points below.
Use the following tests to confirm or rule out a diagnosis of tendinopathy or full-thickness rotator cuff tear.
Combinations to confirm a diagnosis:
· Full-thickness supraspinatus tear: Jobe/Empty Can + Full Can + External Rotation Lag Sign
· Full-thickness infraspinatus tear: External Rotation Lag Sign
· Full-thickness subscapularis tear: Lift-off + Belly Press or Belly Press + Bear Hug
· Rotator cuff tendinopathy/Partial tear: Painful Arc Test
Tests to rule out a diagnosis:
· Full-thickness supraspinatus, infraspinatus, or subscapularis tear: none
· Rotator cuff tendinopathy/partial tear: painful arc test or Hawkins-Kennedy test
To perform these tests, watch the following videos closely:
Jobe test/empty can test:
Full can test:
External rotation lag sign:
Lift off test:
Belly press test:
Bear hug test:
Painful arc test:
Hawkins-Kennedy test:
Other orthopedic tests for RCRSP are:
Imaging
Medical imaging is usually not needed, except when you are suspicious of a more sinister pathology during the history taking. Outside of this exclusion use, imaging results will not change non-surgical management in RCRSP (Littlewood et al 2019).
Imaging can be useful when the patient experiences shoulder trauma, when there’s a suspicion of a full-thickness tear, or when non-surgical management isn’t going according to plan. Consider using ultrasound as opposed to MRI since it is cheaper, often quicker, and has similar diagnostic properties for tears. It is important to discuss the diagnostic values and interpretation of the imaging results with the patient (Lafrance et al 2022).
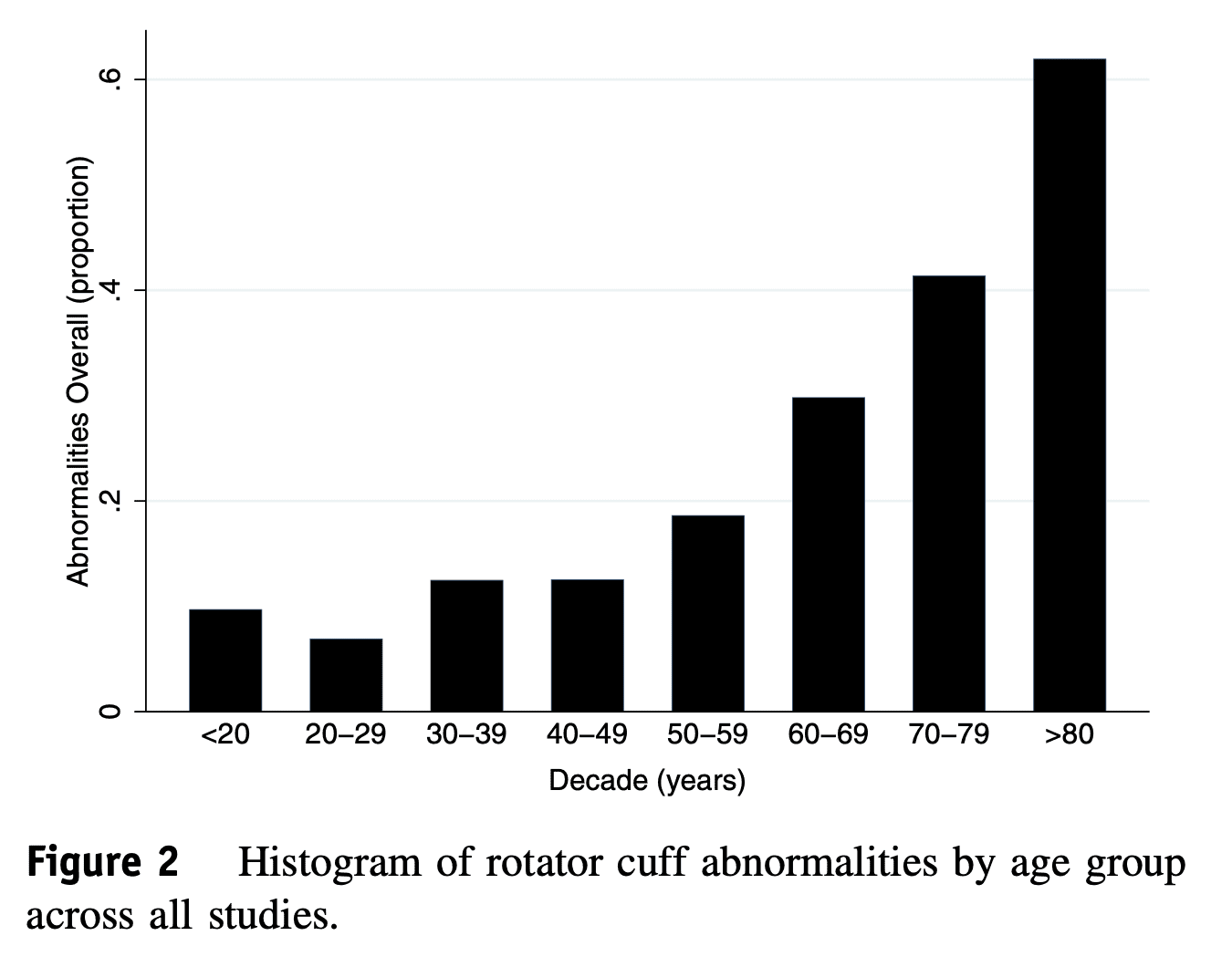
If your patient already got an MRI or ultrasound, know that ‘abnormalities’ are normal, even in asymptomatic individuals. Be aware of this when interpreting imaging results. Teunis et al (2014) investigated this. The following image gives an overview of rotator cuff abnormalities per age group.
Differential diagnoses
- Rotator cuff full-thickness tear
- Glenohumeral osteoarthritis
- AC joint pain
- Frozen shoulder
- Shoulder instability
- Parsonage-Turner syndrome
LEVEL UP YOUR ROTATOR CUFF DISORDER KNOWLEDGE – FOR FREE!

Treatment
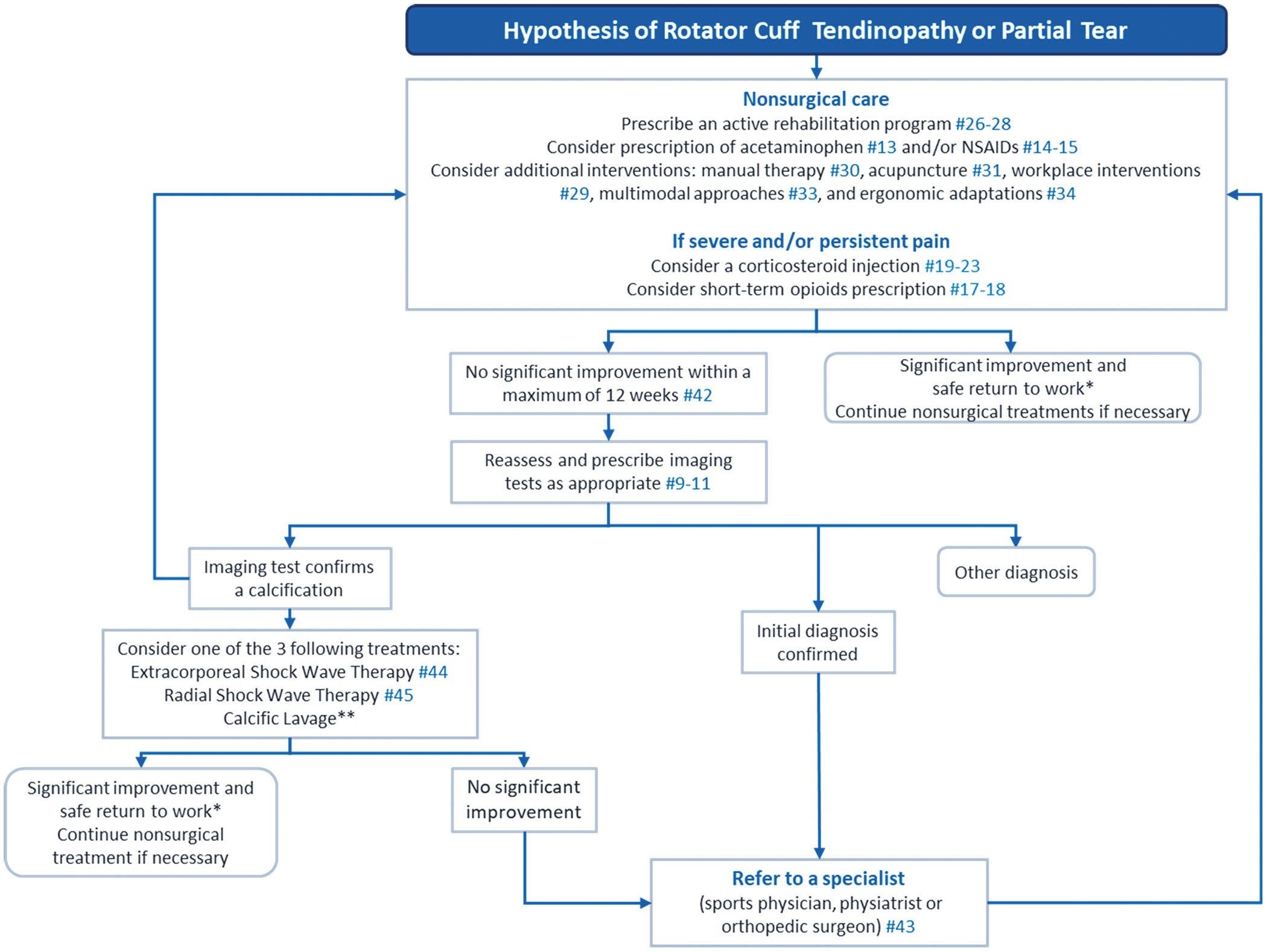
The guidelines recommend the following treatment pathway for individuals suffering with RCRSP:
Education
How can you explain what’s going on to your patients? You could tell them that there’s an issue with the muscles and tendons of the shoulder. They lack strength, capacity, tolerance, and fitness; making them complain when you lift your arm.
Medication
With medications, most recommendations are based on indirect evidence (Lafrance et al 2022), and corticosteroid injections may reduce pain in the short term but increase the risk of retearing and revision after surgery (Puzzitiello et al 2019).
Surgery
If surgery is necessary, repairing the cuff is an option. However, it is important to consider prognostic factors associated with an increased disability after surgery, such as a large tear, lower preoperative strength, low patient expectations, diabetes, obesity, and a sedentary lifestyle (Lafrance et al 2022). A Cochrane review shows high-quality evidence against the use of decompression surgery in rotator cuff disease (Karjaleinen et al 2019).
Exercise & manual therapy
There is strong evidence to suggest that exercise therapy is the way to go for RCRSP. This can be combined with manual therapy (Pieters et al 2020, Franco et al 2019). A treatment program for at least 12 weeks is suggested (Lafrance et al 2022).
Currently, the optimal dose and further specifics are unknown so further elaborations are hard to make (Lafrance et al 2022, Puzzitiello et al 2019). However, a consensus statement by Littlewood et al (2019), suggests the following:
It is essential to follow a comprehensive exercise program for at least 12 weeks for the best prognosis. The preferred treatment for rotator cuff injuries is loading through progressive exercise, including the kinetic chain, and working to fatigue with an acceptable symptom response. Exercising on alternate days is sufficient, and heavy loading or plyometrics may require two to three sessions per week. Three exercises are usually enough and should address personal functional limitations. While exercises can provoke pain, they should be continued as long as symptoms settle sufficiently.
Shockwave (ESWT)
If an ultrasound or MRI confirms calcification of the rotator cuff tendons and the patient remains refractory to initial nonsurgical management, shockwave or an arthroscopic lavage can be considered (Lafrance et al 2022). However, a Cochrane systematic review contradicts the shockwave statement (Surace et al 2020) and the lavage is supported by low-quality evidence (Lafrance et al 2019).
References