Posterolateral Rotatory Instability of the Elbow (PLRI) | Diagnosis & Treatment

Posterolateral Rotatory Instability of the Elbow (PLRI) | Diagnosis & Treatment
Introduction & Epidemiology
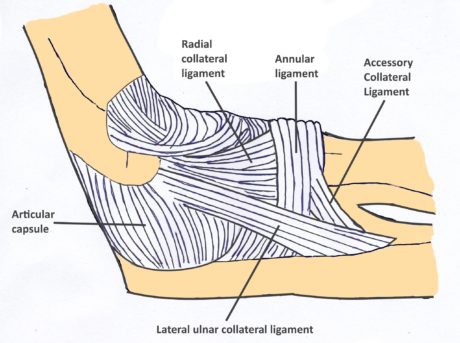
 The elbow is the second most often dislocated joint in the body after the shoulder. PLRI is the most common form of elbow instability as the result of disruption of the lateral collateral ligament complex. This leads to posterolateral rotatory subluxation of the ulna and radius.
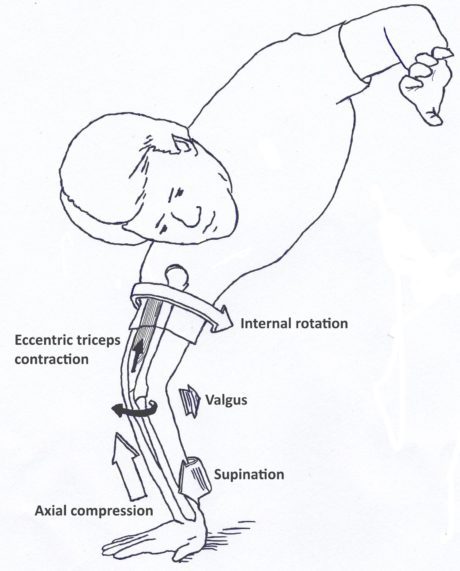
The elbow is the second most often dislocated joint in the body after the shoulder. PLRI is the most common form of elbow instability as the result of disruption of the lateral collateral ligament complex. This leads to posterolateral rotatory subluxation of the ulna and radius.It typically occurs as a result of a fall on the outstretched hand, generating an axial load, valgus force, and an external rotation movement about the forearm with respect to the humerus.
This causes the radial head and proximal ulna to subluxate posterolaterally away from the humerus in a rotatory fashion detaching or tearing the lateral collateral ligament (LCL) complex (Camp et al. 2017).
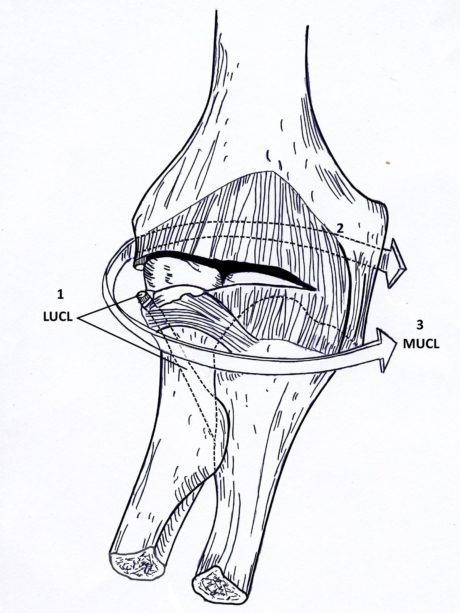
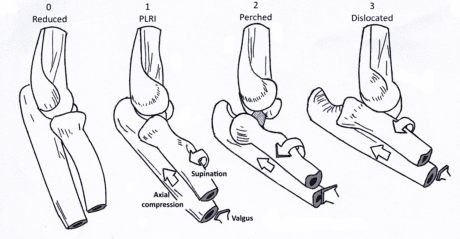
The severity of PLRI can be divided into three stages (Camp et al. 2017):
1. Detachment or tearing of the LCL complex
2. Perched dislocation: Greater anterior displacement, progression of tissue disruption anteriorly and posteriorly around the elbow to the medial side
3. Full dislocation: Tissue disruption involves the medial collateral ligament, which is typically peeled off the bone
With further displacement, the dislocation forces continue to detach or tear the common flexor-pronator origin, resulting in a grossly unstable elbow (described as stage 3c).
Next to trauma, PLRI can also be associated with tennis elbow or iatrogenic injury from prior lateral elbow surgery. It may also present as a tardy PLRI caused by cubitus varus from malunion of a childhood supracondylar humerus fracture (Camp et al. 2017).
No data on incidence or prevalence are currently described in the literature for elbow instability.
Clinical Presentation & Examination
Signs & Symptoms
Patient history will often disclose prior elbow trauma with a subluxation or dislocation event or previous lateral elbow surgery (Singleton et al. 2004).
Patients often complain about lateral elbow pain with activities that place the elbow into extension and supination. This can for example be pushing on armrests to get up from a chair or a prone push-up motion. Furthermore, the elbow pain may be accompanied by mechanical symptoms such as clicking, locking, or snapping that is most prominent at around 40° of flexion as the arm extends (Fedorka et al. 2016).
In contrast, patients with chronic PLRI usually have a full range of motion without pain.
Camp et al. (2017) mention three broad categories of PLRI presentation:
-
- Majority of patients: Mechanical symptoms of instability after elbow trauma with dislocation, subluxation, or fracture-dislocation. These patients complain of clicking, snapping, or a clunk. Patients might notice a bump and/or a dimple if the elbow has a tendency to subluxate for more than a few seconds. Some patients might even be able to subluxate the radius under their own volition.
- Patients present with lateral elbow pain, often without mechanical symptoms, and a history of tennis elbow or lateral elbow surgery. Oftentimes, these patients have had cortisone injections for their tennis elbow, which might have a causal relationship with the development of instability.
- Tardy PLRI: Altered elbow mechanics cause gradual attenuation of the LCL complex. This can often be the case in patients with cubitus varus from a childhood supracondylar malunion and patients with dysplasia or hypoplasia of the coronoid.
Physical Examination
To begin your assessment, elbow mechanics and alignment, especially for cubitus varus, should be examined. According to Camp et al. (2017), the Posterolateral Rotatory Drawer Test is the most reliable and sensitive test for PLRI as it can be performed in anesthetized and awake patients. However, no study has yet validated this claim.
The Lateral Pivot-Shift Test can be difficult to perform in awake patients due to inadequate relaxation or discomfort. For this reason, the test is scored positive in the case of Apprehension.
For this reason, the test is also called Lateral Pivot-Shift Apprehension Test. The Pivot-Shift Test has been validated by Regan et al. (2006) who found a sensitivity of 100% in anesthetized subjects and 37,5% in awake patients with unknown specificity values.
Apprehension by the (awake) patient, therefore, indicates a positive test and usually occurs at around 20-40° of elbow flexion.
The subluxation can be reduced with a clunk (in patients who can completely relax).
Other common orthopedic tests to assess posterolateral rotatory instability of the elbow are:
WATCH TWO 100% FREE WEBINARS ON SHOULDER PAIN AND ULNA-SIDE WRIST PAIN