Hip Osteoarthritis | Diagnosis & Treatment

Hip Osteoarthritis | Diagnosis & Treatment for Physiotherapists
Introduction
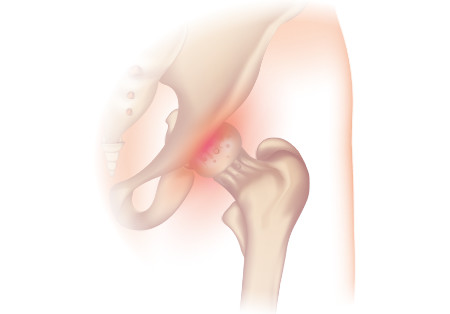
According to Felson et al. (2005) A classical feature of osteoarthritis is histological changes in the quality and thickness of joint cartilage. A decrease in joint cartilage leads to hypertrophy of the subchondral bone and osteophyte formation at the edges of the joint surfaces. Another consequence is chronic inflammation of the synovial tissue. All of these changes lead to irregular joint surfaces, bony enlargement, possible thickening of the joint capsule, and eventually hydrops. The resulting decrease in joint space is visible on radiographic imagery, which is why we also speak of “radiological osteoarthritis”.
Pain is the most evident limiting factor in osteoarthritis. As previously mentioned, the pathophysiology describes a loss of cartilage but nociceptors are missing in joint cartilage.
We know that a decrease in joint cartilage occurs also in those without clinical symptoms (radiological osteoarthritis).
Nociceptors are present in tissues surrounding the hip joint such as the joint capsule, ligaments, or the synovium. These nociceptors get triggered by the inflammation that occurs.
Osteoarthritis can occur post-traumatically, as a process of aging, and in other inflammatory conditions affecting the quality of joint cartilage.
Epidemiology
Hip osteoarthritis is less common than knee osteoarthritis. For the peak incidence between the age of 78-79, Felson et al. (1998) report an incidence of 600/100.000 person-years for females and 420/100.000 for males with hip osteoarthritis.
The point prevalence of osteoarthritis in the Netherlands in 2007 was 24,5/1000 in males and 42,7/1000 in females. Around the world, the prevalence is reported at 0,85% (Cross et al. 2014)
LEVEL UP YOUR DIFFERENTIAL DIAGNOSIS IN RUNNING RELATED HIP PAIN – FOR FREE!








