De Quervain's Tenosynovitis | Diagnosis & Treatment

De Quervain’s Tenosynovitis | Diagnosis & Treatment
Introduction
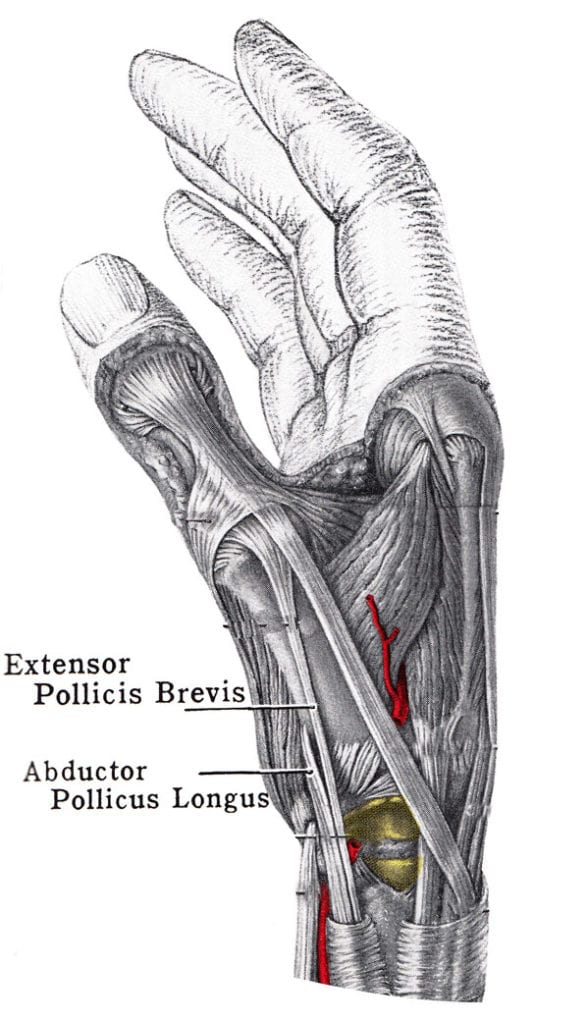
De Quérvain’s disease or de Quérvain stenosing tenosynovitis involves irritation of the tendons of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) within the first dorsal compartment of the hand as they pass through a swollen extensor retinaculum (Adams et al. 2015).
It is commonly assumed that repetitive overload of the wrist and thumb is the cause of the disease. This includes activities involving repetitive ulnar deviation such as hammering, cross-country skiing, or lifting (Moore 1997, Adams et al. 2015).
Risk factors for the condition include:
- Female gender
- Age 35 – 55
- Pregnancy or postpartum and lactation
- Arthritic changes of the first metacarpal
- Diabetes, rheumatoid arthritis, gout
Epidemiology
The prevalence of the condition in the general population is estimated at 5/1000 persons in males and 13/1000 persons in females. It predominantly occurs in women between the age of 35 – 55 and mostly during or after pregnancy. The latter may have to do with higher estrogen receptor-β expression (Shen et al. 2015).
Furthermore, there seems to be a correlation between degenerative conditions such as arthritis of the first metacarpal and de Quérvains disease (Stahl et al. 2013, Andreu et al. 2011).
Clinical Presentation & Examination
Signs & Symptoms
The hallmark symptom is pain at the radial side of the wrist. This is aggravated during activities that involve ulnar deviation (with a closed fist). Thumb function is also limited due to pain. Furthermore, swelling may be present around the radial styloid process (Goel et al. 2015).
Examination
Typically, the history and physical presentation of the condition provides enough diagnostic value. There are two diagnostic tests described in the literature.
The Finkelstein test is the hallmark test to diagnose de Quervain’s tenosynovitis although no values and validity are known. So the clinical value of this test is questionable.
To perform the test Dawson et al. (2010) recommend a three-stage process that is well tolerated and able to diagnose de Quervain’s tenonitis accurately. To perform the test, have your patient’s affected extremity extended so that the wrist remains at the edge of the treatment table the arm is positioned with the ulnar aspect of the forearm on the table, and the ulnar aspect of the hand hanging off of the edge. The forearm is maintained in neutral.
In the first step, the patient’s pain is assessed with gravity-assisted gentle active ulnar deviation at the wrist. This version is suitable for patients who present in the acute phase. This test is positive if the patient reports pain aggravation at the tip of the styloid process.
If version one does not elicit pain, gently apply a deviation force to the hand which results in an increased passive stretch across the first dorsal compartment. Again, this test is positive if the patient reports aggravated pain over the styloid process.
If the second step is still not provoking, we will perform the original version described by Finkelstein et al. which is suitable for patients in the chronic stage that are unlikely to experience substantial pain in the first two steps. In this third step, grasp the thumb and then passively flex it into the palm.
A positive test result is recorded if the patient experiences increased pain over the tip of the styloid process. Performing the test in this stage manner is hypothesized to create fewer false positive results as it is less provocative than the Eichhoff test which is often confused with the Finkelstein test.
In the literature, there’s a lot of confusion regarding the original version of the Finkelstein test. Elliot et al. (1992) state that over the last three decades an error in performing Finklestein’s test has crept into the English literature in textbooks and journals. This error can produce a false positive and if relied upon a wrong diagnosis can be made leading to inappropriate surgery. The error that has crept into the literature is actually Eichhoff’s test. Because no validity studies have ever been conducted for this test its clinical use is questionable.
To perform this test have your patient extend his affected extremity and rest it on the treatment table so that the wrist is hanging off the table. Then, ask him to make a fist with the thumb inside his fist, stabilize the forearm on the table and gently deviate the wrist towards the ulnar side.
This test is positive if your patient experiences pain over the tendons of the extensor pollicis brevis and abductor pollicis longus which both form the medial base of the anatomical snuffbox.
Due to its very provocative nature, Eichhoff’s test can cause a lot of false positives which is why we recommend rather to perform the original version of the Finkelstein test.
WATCH TWO 100% FREE WEBINARS ON SHOULDER PAIN AND ULNA-SIDE WRIST PAIN




