
Research
Exercise
June 18, 2026
Stepwise Gluteus Maximus Activation for Chronic Mechanical Low Back Pain: Is It Worth the Effort?

Introduction
A decrease in strength in the gluteus maximus muscles can be involved in low back pain. Some authors suggest that poor neuromuscular control and activation can result in dysfunctional lumbopelvic stabilization. As the glute max is thought to be a crucial link in lumbopelvic stability, its role for efficient load management and transfer across the spine during dynamic movements seems to be of utmost importance. Delayed or ineffective activation has been associated with movement compensations and higher spinal stress. The authors emphasize that a program targeted at the activation of the gluteus maximus could overcome the problem of ineffective load transfer in the region of the pelvis and lower back. Therefore, this study aimed to investigate the effect of a stepwise gluteus maximus activation program designed for patients with chronic mechanical (nonspecific) low back pain.
Methods
A single-blinded, parallel-group randomized controlled trial was conducted, including participants who were referred by orthopedic physicians and screened by an experienced physiotherapist. The definition of chronic mechanical low back pain was based on mechanical pain behaviour: symptoms increased with movement or prolonged posture and improved with rest, without any evidence of neurological involvement or systemic diseases.
Participants were randomly allocated to either:
Control group: Those who received conventional physiotherapy only. This consisted of flexibility exercises for back and hip muscles, a hot pack for 10 minutes, and high-frequency TENS for 15 minutes over the most painful area.
Intervention group: This group performed the stepwise gluteus maximus activation program plus the same conventional treatment. The stepwise activation program was based on the “Powers’ program” and included eight progressive phases.
- Phases 1–3 focused on gluteus maximus activation
- Phases 4–5 on strengthening
- Phases 6–8 on functional/ballistic application.
Exercises were progressed using yellow, green, and blue resistance bands. Participants performed three sets of 10 repetitions, and progression depended on completing the required repetitions and holds with good performance. Both groups received four weeks of three sessions per week, totalling 12 sessions.
Outcomes were measured before and after the intervention. Primary outcomes were pain captured by the VAS scale and disability measured using the Oswestry Disability Index. Secondary outcomes were gluteus maximus strength assessed with a handheld dynamometer and functional performance using the single-limb triple hop test and single-limb crossover hop test.
Results
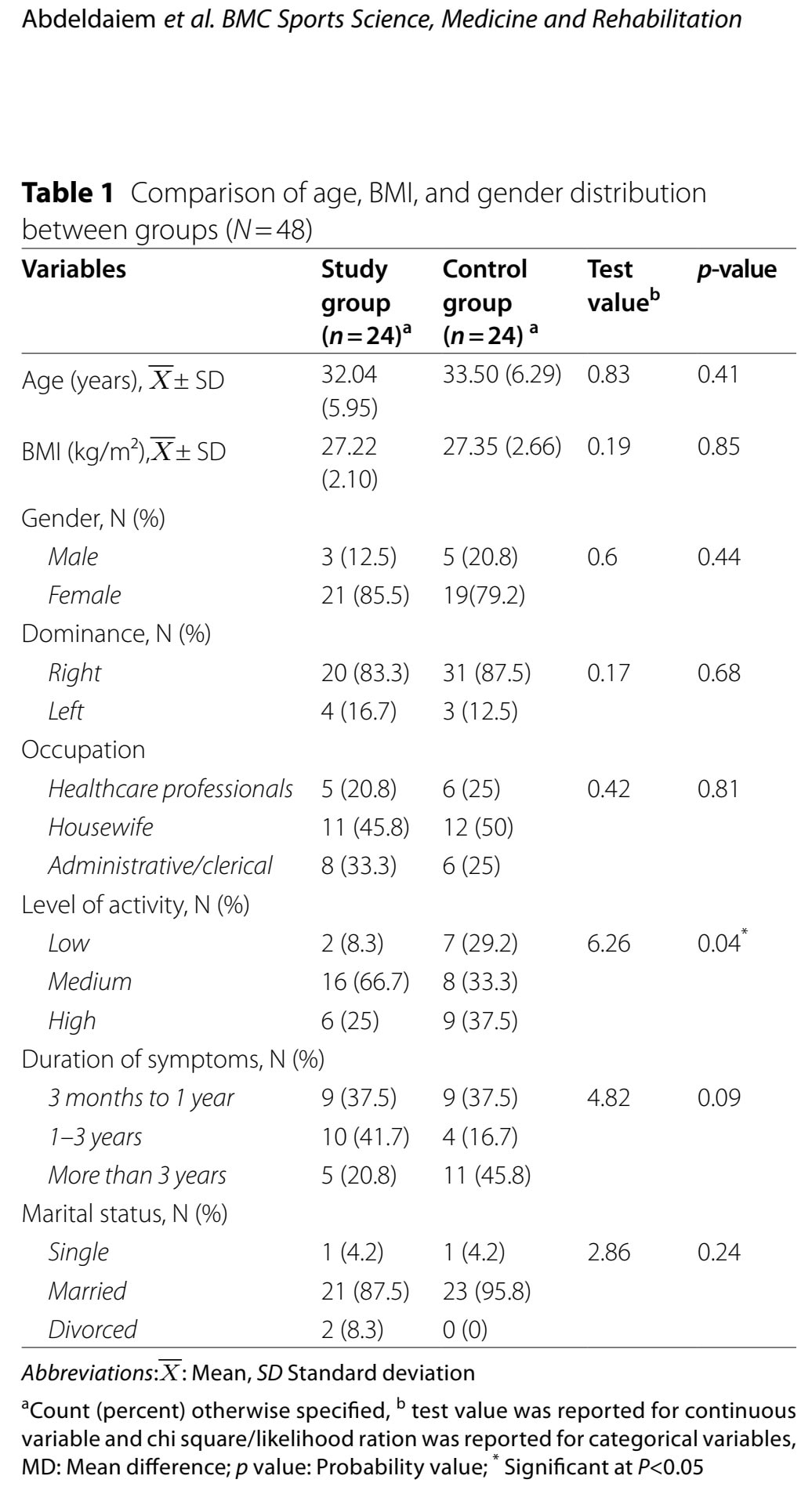
Forty-eight participants with chronic mechanical low back pain were analyzed after four participants dropped out. Baseline characteristics were comparable, except for the level of activity; a group difference emerged.
Both groups improved significantly over time in pain, disability, gluteus maximus strength, and hop-test performance, as can be seen in the within-group improvements. However, the main between-group MANOVA was not statistically significant, indicating that no between-group differences were found.
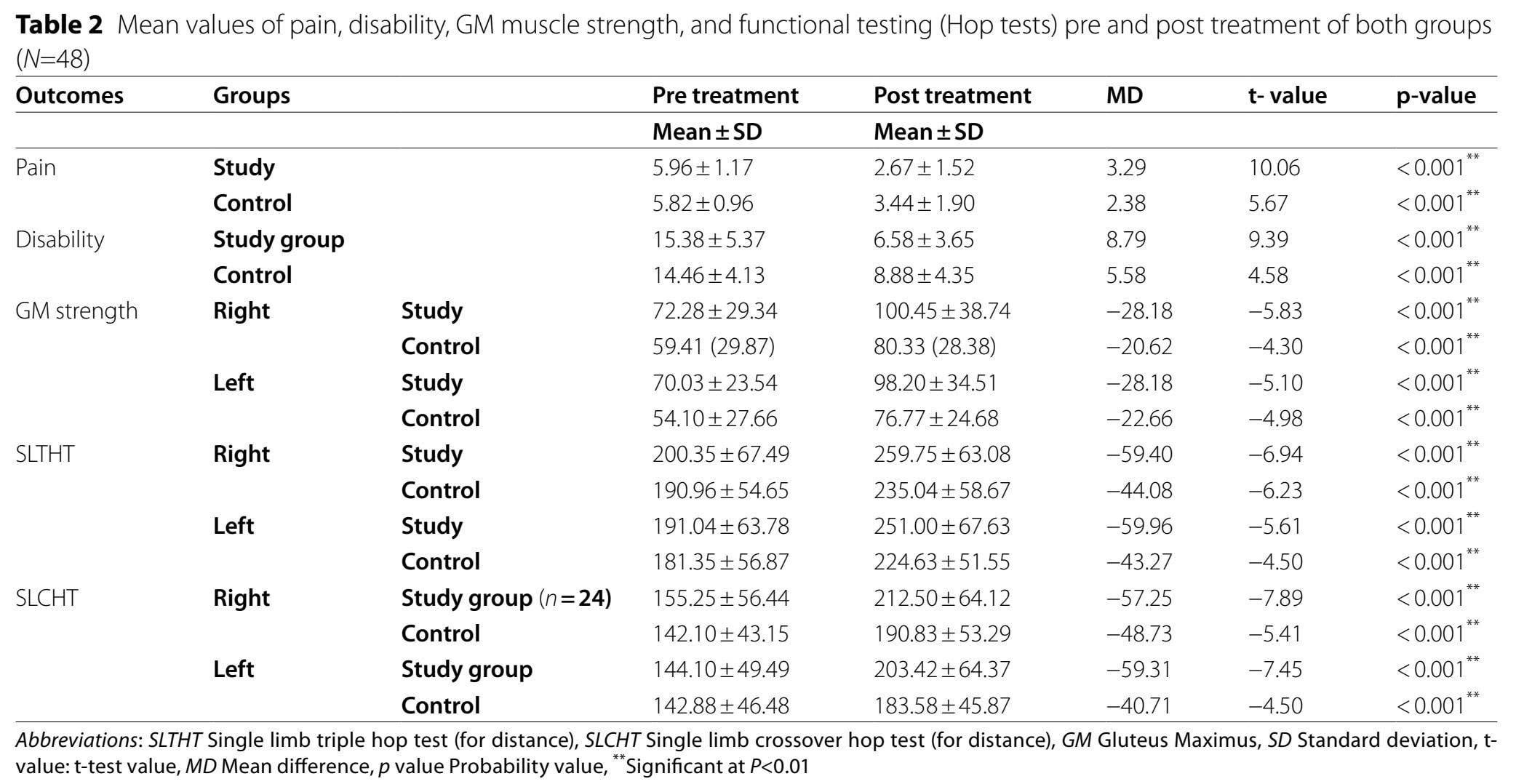
Table 3 shows the between-group comparisons after treatment for each outcome, computed separately using individual ANOVAs. In other words, it examines whether the study group (Powers’ program + conventional treatment) performed differently from the control group (conventional treatment only) at the end of the intervention. The only between-group findings that reached significance in follow-up analyses were right and left gluteus maximus strength.
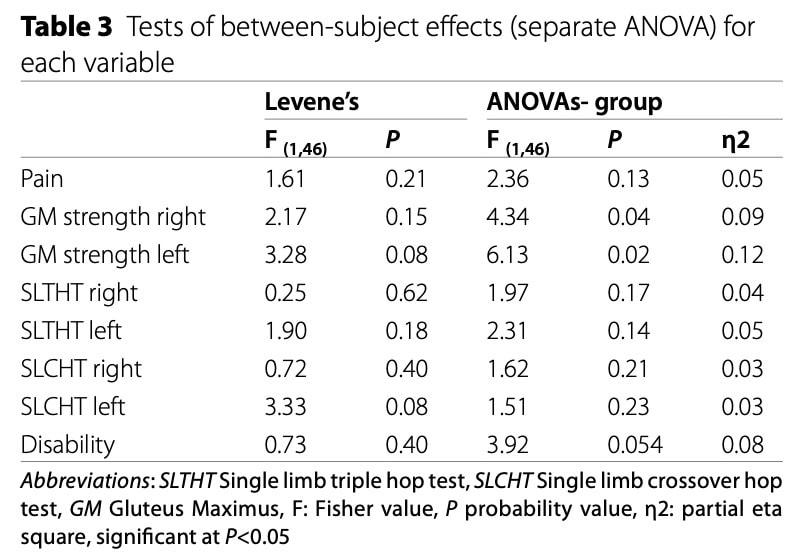
This is a major caveat: The overall MANOVA was not significant (p = 0.40). Normally, the MANOVA analysis is performed first to determine whether the groups differ across the set of outcomes as a whole. Since that test was negative, interpreting the individual ANOVAs becomes problematic because performing multiple separate tests increases the risk of finding a significant result simply by chance (Type I error)
In practical terms, adding Powers’ did not clearly outperform conventional care for pain, disability, or functional hop performance over four weeks.
Questions and thoughts
So, based on the results, is a stepwise gluteus maximus activation program for chronic low back pain worth the effort? It appears not, because when we look at the primary outcome analysis of pain and disability.
Strength also improved in the control group, despite the fact that these patients did not perform any exercises other than flexibility ones. So, instead of framing a significantly greater difference in a secondary outcome, the authors could have also pointed out that 4 weeks of receiving heat and TENS yielded the same improvements in pain and disability compared to the stepwise activation program for the gluteus maximus. As you can see, framing is an important pitfall to watch out for in scientific studies. The greater improvement in the secondary outcome of gluteus maximus strengthening may be relevant, if not a type I error, but this study can not claim this based on the selection of another primary outcome. It can only help to direct future studies to include gluteus strength as a primary outcome measure, before any confirmation can take place.
Another possibility, in my opinion, is that since people got guided and likely got some support and affection from the treating physiotherapist, they got encouraged to increase their activation and participation in movement and exercise along the way. The observed strength difference could reflect a true training effect, a chance finding due to multiple comparisons, or nonspecific effects associated with receiving additional supervised exercise. Nevertheless, no weights were added to the exercise, which may be okay for people starting exercise after being affected by their chronic LBP, to overcome the risk of them fearing the exercises. But after 4 weeks, progressions in exercise difficulty, for example, using weights, are probably indicated.
Needless to say, it would be amazing if a 4-week intervention could be efficacious for people who experience chronic low back pain, but this hypothesis is somewhat optimistic. As the majority of people in this study were affected for more than 1 year, these are probably more on the spectrum of chronic pain-related changes than pure nociceptive input. Moreover, no measures of kinesiophobia, or pain catastrophizing, were obtained, although highly relevant in this chronic pain population. Lastly, the conventional care definition of passive therapy for chronic low back pain in this study seems outdated.
A clinically important question is whether all patients with chronic mechanical low back pain need gluteus maximus strengthening, or whether only a subgroup with clear hip-extension weakness, poor lumbopelvic control, or reduced gluteal capacity would benefit.
Another question is whether hop tests are the best functional outcome for this population. They are demanding, lower-limb dominant tests and may not directly reflect daily low back pain disability. It would also be useful to know whether participants actually moved differently after the program. The study measured strength and hop distance, but unfortunately, not kinematics, muscle activation timing, lumbar motion, or load transfer.
Talk nerdy to me
The authors concluded that adding a stepwise activation program to conventional care is a worthwhile intervention, as the strength of the gluteus maximus increased more in the intervention group than in the control group. Yet, this was a secondary outcome, and more importantly, a conclusion of a series of one-way ANOVAs on each of the outcomes after the non-significant MANOVA concluded no difference in the primary outcome. No correction for multiple outcomes has been conducted, and most strikingly, the authors use the within-group improvement to frame the efficacy of the training group.
Interestingly, the authors emphasize that the study group exceeded published minimal clinically important difference (MCID) thresholds for pain and disability. However, MCID is generally intended to evaluate whether a change is meaningful within an individual patient, not whether one intervention is superior to another. Since both groups improved over time and no significant between-group differences were found for pain or disability, exceeding MCID thresholds does not establish superiority of the stepwise activation program. In this context, the MCID findings are better interpreted as evidence that participants improved during treatment, rather than evidence that the gluteus maximus activation program was more effective than conventional care alone.
Perhaps the most surprising aspect of the paper is that the authors conclude that disability improved more in the intervention group, despite their own between-group analysis failing to reach statistical significance for disability (p = 0.054). Disability was one of the primary outcomes, yet the statistical analysis did not support a between-group difference. This makes the wording of the conclusion difficult to reconcile with the presented results.
The most striking conclusion the authors made is that adding the stepwise gluteus maximus activation program to the conventional intervention provided higher improvement in gluteus maximus strength and disability, compared to the conventional intervention alone. Yet, disability was never significant in their analyses, and that is striking to see that conclusion coming through a peer-reviewed journal.
Take-home messages
Adding a stepwise gluteus maximus activation program to “conventional” physiotherapy did not clearly improve pain, disability, or functional performance beyond usual care over four weeks, despite what the authors concluded. The study failed to demonstrate that adding a stepwise gluteus maximus activation program produced greater improvements in pain or disability than the conventional intervention alone. The study framed a within-group improvement from a post-hoc secondary analysis after a nonsignificant main effect as a worthwhile improvement. Yet, we can not support this conclusion when looking at the data in front of us. The intervention was only delivered for about 4 weeks to a chronic pain population, and the lack of biopsychosocial interventions is likely insufficient.
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Download this FREE home exercise program for your patients suffering from headaches. Just print it out and hand it to them for them to perform these exercises at home
