Research
Diagnosis & Imaging
April 24, 2026
Carpal Tunnel Syndrome Diagnosis: Hand Pain and Sensory Deficits – Latest Evidence from Clinical Practice Guidelines - Part 1: Examination and Diagnosis

Introduction
Hand pain and sensory deficits are often challenging presentations in physiotherapy practice. This newly released clinical practice guideline provides updated insights into the assessment and management of extremity pain, building on the previous 2019 guidelines. The hand and upper limb can be particularly complex due to their intricate anatomy, which may leave clinicians feeling uncertain when evaluating and treating conditions such as carpal tunnel syndrome.
This review aims to present the latest evidence, including validated clinical tests, questionnaires, and diagnostic procedures, to support physiotherapists in navigating the often complex presentations of hand pain and sensory deficits, and to strengthen confidence in clinical decision-making. This research review is the first in a two-part series for Physiotutors, focusing on the clinical presentation and assessment of hand pain and sensory deficits for carpal tunnel syndrome diagnosis. The second article will explore outcome measures and intervention strategies.
Methods
This clinical practice guideline (CPG) update for the non-surgical management of carpal tunnel syndrome (carpal tunnel syndrome ) was developed by content experts appointed by the American Physical Therapy Association (APTA) Orthopedics and APTA Hand and Upper Extremity.
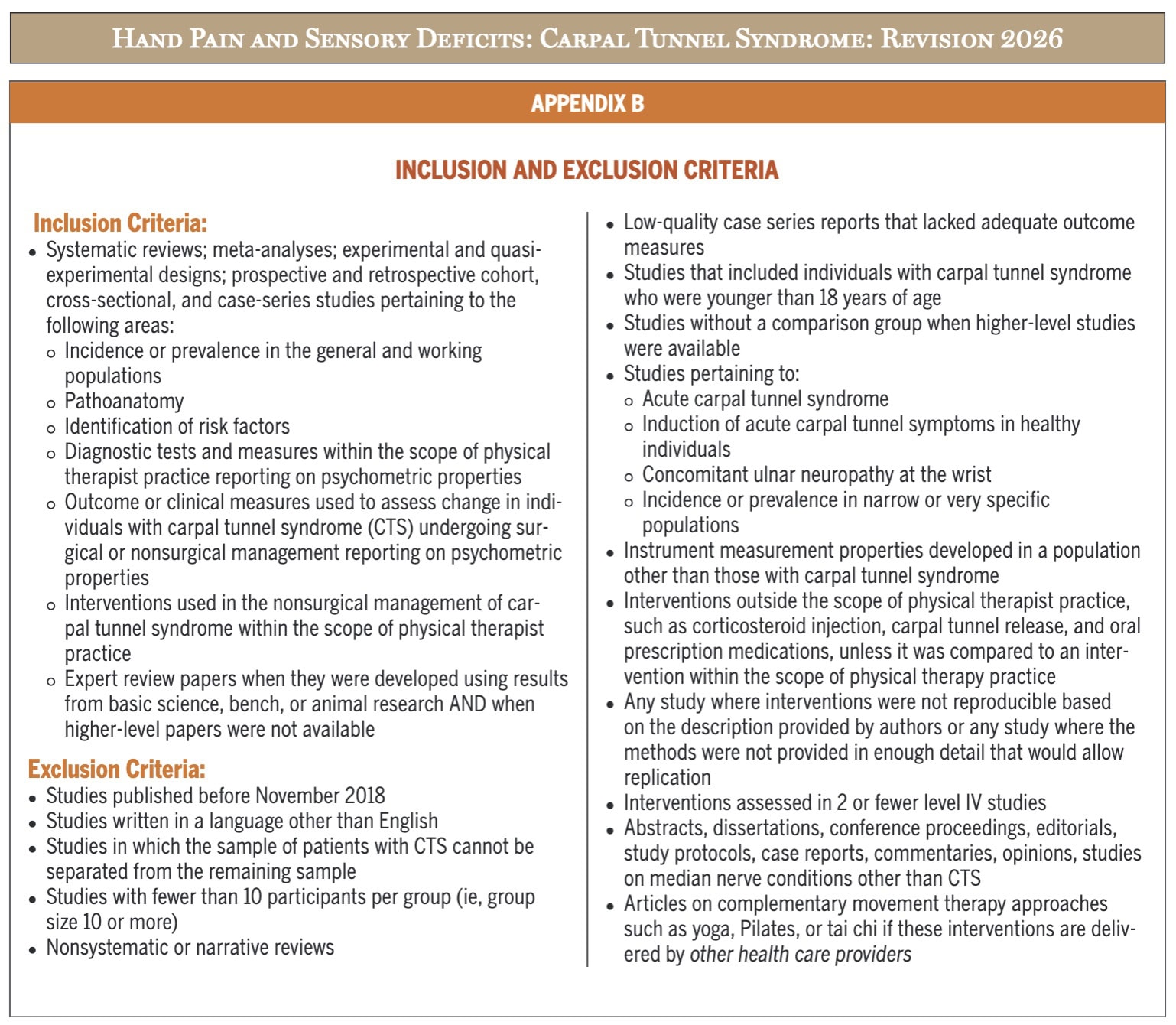
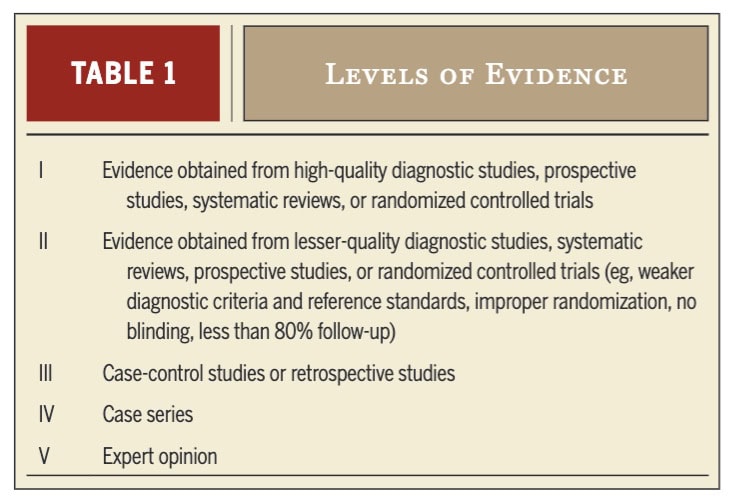
The authors conducted a systematic review of the literature published between November 2018 and May 2025. Articles were independently screened by two reviewers using predefined inclusion and exclusion criteria (detailed in Appendix B), and any disagreements were resolved by a third reviewer. Data extraction and assessment of the level of evidence were also performed by two reviewers, using criteria adapted from the Oxford Centre for Evidence-Based Medicine, and studies were organized from highest to lowest quality.
Recommendations were developed based on the strength and relevance of the evidence, as well as consideration of benefits, risks, and clinical applicability, and were agreed upon by the full development group. Measures were taken to ensure transparency and minimize bias, including the declaration of conflicts of interest and maintaining independence from funding bodies. The guideline was further reviewed by a broad panel of experts, stakeholders, and the public to ensure accuracy and completeness. Published in 2026, the guideline will be reassessed in 2031 or earlier if new evidence becomes available.
Results
This Part 1 will focus on the findings regarding prevalence and incidence, carpal tunnel syndrome pathogenesis, clinical course, risk factors, and examination. The next review to be published next week will discuss the treatment strategies.
Prevalence and incidence
Carpal tunnel syndrome affects approximately 14.4% of the global population, with higher prevalence reported in high-income countries and among individuals with diabetes (up to 39%). It is more common in women than men, particularly in middle age, and incidence varies by occupation, being significantly higher in manual workers compared to clerical workers.
Pathogenesis
Carpal tunnel syndrome is primarily driven by increased pressure within the carpal tunnel, leading to median nerve ischemia, intraneural edema, and eventually fibrosis of the nerve and surrounding structures. Fibrotic changes, particularly in the tenosynovium, can further compress the nerve and reduce available space, contributing to symptom development. These processes are thought to reflect a low-grade chronic inflammatory response, with evidence showing involvement of both small and large nerve fibers. Imaging studies (e.g., ultrasound) commonly demonstrate enlargement of the median nerve and altered blood flow, especially in early stages. Systemic inflammation may also play a role by impairing nerve microcirculation and promoting fibrosis through immune-mediated mechanisms. Additionally, fibrosis can reduce normal nerve mobility within the carpal tunnel. However, it remains unclear whether inflammation and fibrosis are causes or consequences of nerve compression.
Clinical course
Carpal tunnel syndrome typically presents with numbness, paresthesia, and pain in the median nerve distribution, often beginning with nocturnal symptoms and functional complaints such as dropping objects. As the condition progresses, patients may develop weakness of the thenar muscles, leading to reduced grip and pinch strength, and in severe cases, visible thenar atrophy and loss of thumb opposition. Advanced or prolonged compression can result in significant functional impairment, sometimes irreversible even after surgical release. Carpal tunnel syndrome may present acutely (e.g., following trauma, inflammation, or pregnancy) but more commonly has a gradual onset. Although often classified as mild, moderate, or severe, clinical grading based solely on symptoms remains difficult.
Pain is a prominent feature in many patients and can negatively impact quality of life, with a substantial proportion experiencing moderate to severe or neuropathic pain. Greater pain severity is associated with longer symptom duration, sensory deficits, thenar weakness, and psychosocial factors such as pain catastrophizing, anxiety, and depression. Some individuals also exhibit symptoms extending beyond the median nerve distribution, suggesting possible central sensitization, although its clinical assessment remains challenging, and evidence is mixed. Psychosocial factors appear to influence symptom severity and may affect outcomes, particularly following surgery, while physical activity may have a protective effect on pain and mental health. Overall, carpal tunnel syndrome presents as a multifactorial condition with a variable clinical course influenced by both peripheral and central mechanisms.
Diagnosis, testing, and classification
Carpal tunnel syndrome diagnosis remains challenging due to the absence of a true reference standard. Electrodiagnostic (EDX) testing is commonly used to assess large myelinated nerve fiber function, detect demyelination or axonal loss, and differentiate carpal tunnel syndrome from other neuropathies. However, it does not capture small fiber function or all sensory symptoms. Severity classification based on EDX lacks standardization, and some symptomatic patients may have normal results yet still benefit from treatment. Diagnostic ultrasound (US) complements assessment by identifying structural changes, particularly enlargement of the median nerve, though its role in severity grading remains inconsistent.
Carpal Tunnel Release
While many patients are managed conservatively, a substantial number undergo carpal tunnel release (CTR), a common and generally effective surgery, though access varies widely across countries due to differing wait times. Clinical decision-making regarding referral for surgery is complex and should integrate subjective history and objective findings, as no clear thresholds exist. Factors such as thenar atrophy, long symptom duration, persistent or severe symptoms, and prior treatment failure may guide consideration for surgical referral.
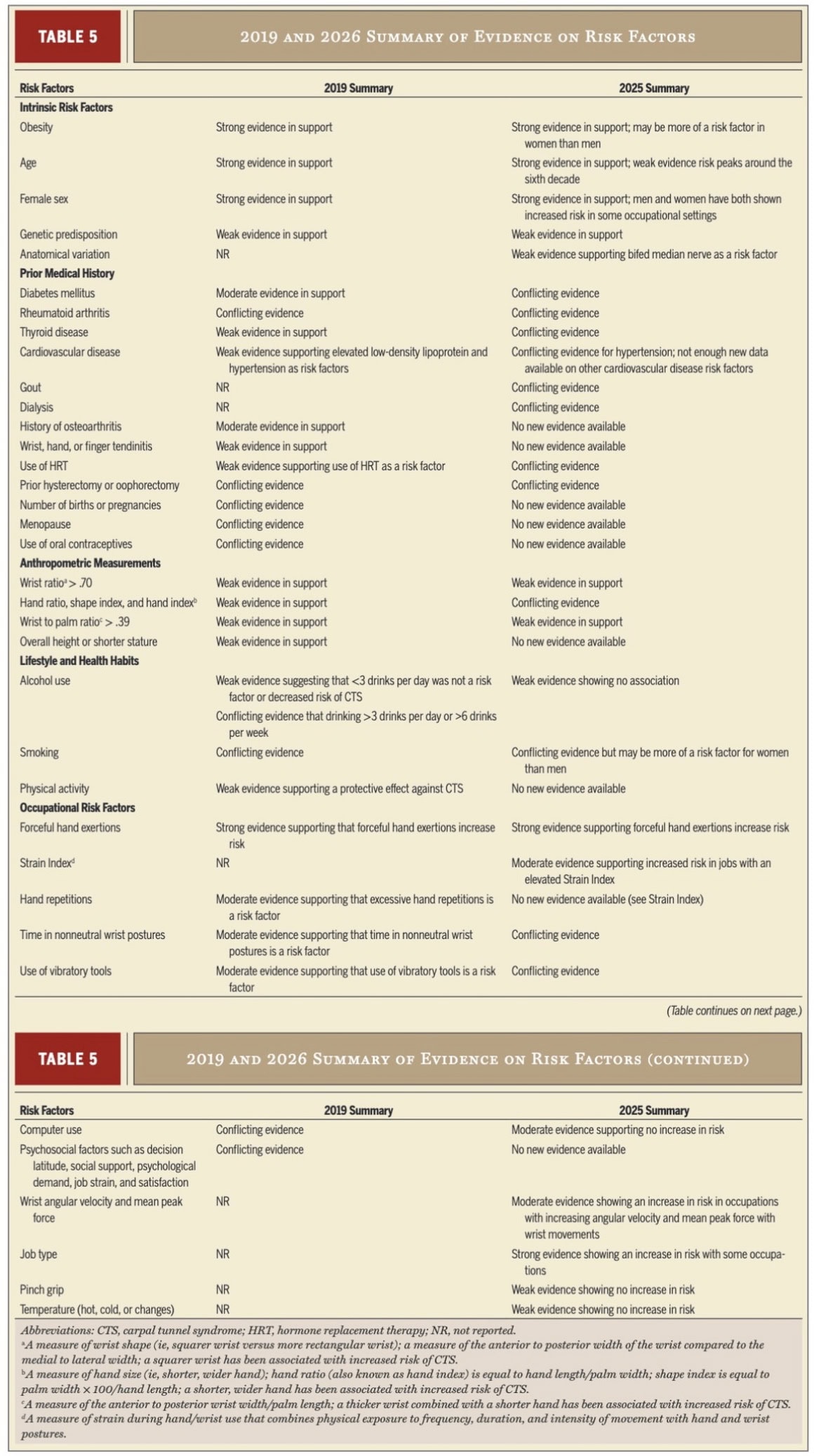
Risk factors
Risk factors are presented in Table 5. The most important ones are:
- Obesity
- Female sex
- Age
- occupational forceful hand exertions
- Job types such as farming, manual labour, and manufacturing
Examination
The examination of patients with suspected carpal tunnel syndrome aims to differentiate carpal tunnel syndrome from similar conditions, identify impairments, and determine suitability for nonsurgical management. Due to the absence of a carpal tunnel syndrome diagnosis gold standard, clinicians must integrate findings from a detailed subjective history and objective examination, including screening for proximal nerve involvement and multiple compression sites.
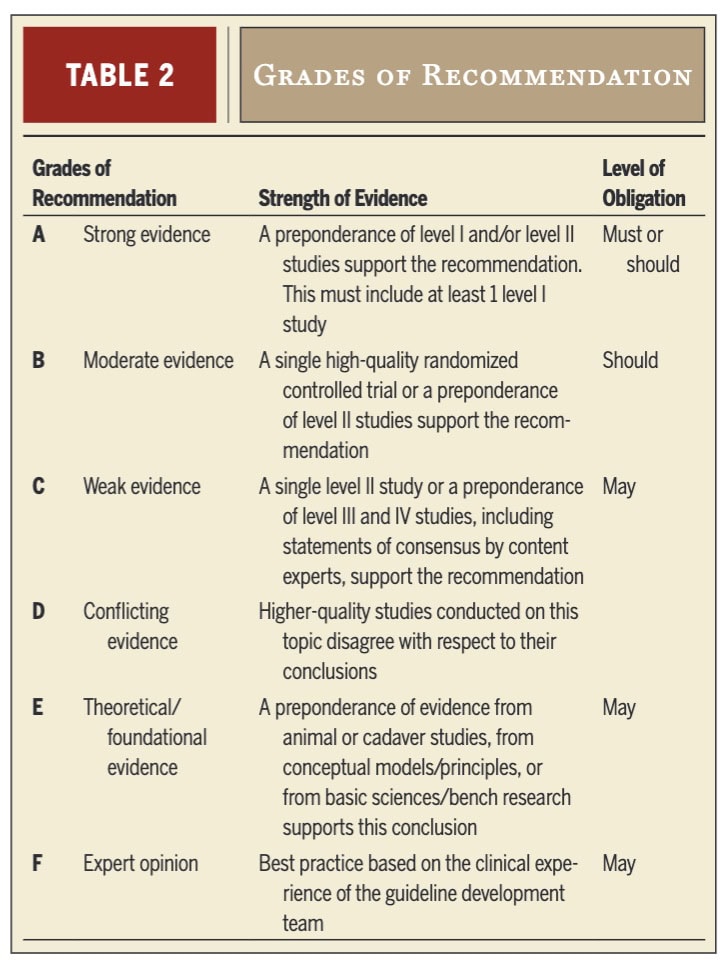
Grade B: Clinicians should use the Katz and Stirrat hand symptom diagram (HSD) to characterize symptom distribution, as it demonstrates moderate to high diagnostic accuracy.
Grade C: Clinicians may use either the Katz and Stirrat HSD or the Kamath and Stothard questionnaire as initial screening tools, particularly in work-related carpal tunnel syndrome, as both show good sensitivity and specificity, although further validation is needed.
Provocative tests
Provocative tests are used to reproduce symptoms and assess median nerve irritability in suspected carpal tunnel syndrome, but no single test is sufficient for carpal tunnel syndrome diagnosis, and results must be interpreted within a broader clinical assessment.
Grade B: Clinicians should use the Phalen test, Tinel sign, and carpal compression (Durkan) test to support diagnosis, as these demonstrate moderate diagnostic utility, with the Durkan test generally showing the highest accuracy.
Other tests, such as the hand elevation test and timed Phalen test, show promising specificity but require further validation. Neurodynamic tests have lower diagnostic value and are better suited for assessing nerve mechanosensitivity, while the scratch collapse test is not recommended due to poor sensitivity and reliability.
Diagnostic testing and sensory measures
Sensory and motor testing is useful for assessing the extent of nerve impairment and functional limitations but cannot confirm carpal tunnel syndrome diagnosis on its own.
Grade A: Clinicians should use the Semmes-Weinstein monofilament test (SWMT) as it demonstrates good reliability and correlation with carpal tunnel syndrome severity.
Grade B: Clinicians should use static two-point discrimination (2PD) to evaluate sensory innervation density in individuals with suspected carpal tunnel syndrome.
Grade C: Clinicians may assess grip and pinch strength (tripod or tip) and evaluate hand function using the PPB or DMPUT in individuals with suspected carpal tunnel syndrome, comparing results with established normative values.
Grade F: Clinicians may examine for thenar atrophy, which is highly specific for severe carpal tunnel syndrome but lacks standardized quantification and diagnostic utility.
Diagnostic testing and sensory measures: Combination testing
Combining multiple clinical tests into a test battery improves carpal tunnel syndrome diagnosis accuracy compared to using individual tests alone.
Grade B: Clinicians should use the Carpal Tunnel Syndrome-6 (carpal tunnel syndrome -6), as it integrates subjective and objective findings and demonstrates better diagnostic performance than individual tests, with scores ≥12 indicating a high probability of carpal tunnel syndrome. Its accuracy may be further enhanced when combined with ultrasound, although it remains effective as a standalone tool.
Questions and thoughts
Diagnostic features of carpal tunnel syndrome (carpal tunnel syndrome) still require further clarification. Clinicians should systematically assess the entire course of the median nerve to identify potential sites of compression, as part of a possible double-crush mechanism. Indeed, the median nerve may be compressed at multiple anatomical interfaces, contributing to symptoms along its distribution. In this context, the CPG emphasizes the importance of screening the cervical spine and other potential proximal compression sites during the clinical examination.
Regarding diagnostic tools, ultrasound (US) appears promising and may offer good validity and reliability in carpal tunnel syndrome assessment. However, electrodiagnostic (EDX) testing—still widely used in clinical and research settings—has notable limitations, particularly its inability to assess small unmyelinated nerve fibers (C and A-δ), which are key contributors to pain. This raises concerns about the overall validity of traditional diagnostic approaches.
Some evidence illustrates these limitations. For instance, one study reported that electrodiagnostic testing (EDX) demonstrated higher sensitivity (87%) but low specificity (27%), whereas ultrasound (US) showed lower sensitivity (76%) but improved specificity (51%). Notably, this study evaluated both modalities against the Carpal Tunnel Syndrome-6 (carpal tunnel syndrome -6), which is recommended in the current guideline as a grade B diagnostic tool. Overall, both modalities demonstrate limitations, and their diagnostic accuracy remains subject to debate.
Talk nerdy to me
The lack of a clear and reliable diagnostic standard for carpal tunnel syndrome raises important concerns regarding the interpretation of current literature. While clinical practice guidelines (CPGs) synthesize the best available evidence, uncertainty in diagnosis and classification remains a key limitation. The recommendation to assess multiple potential compression sites along the median nerve suggests that carpal tunnel syndrome may overlap with other conditions, such as double crush syndrome or thoracic outlet syndrome. This overlap complicates both diagnosis and research interpretation.
Most studies investigating carpal tunnel syndrome interventions rely on diagnoses established through electrodiagnostic testing or ultrasound. However, these tools may not adequately distinguish between different pathologies affecting the median nerve, potentially leading to heterogeneous study populations and blurred treatment effects in carpal tunnel syndrome. Although large sample sizes in CPGs provide strong statistical power, they may also mask individual variability and limit the applicability of generalized recommendations to specific patients, highlighting the importance of clinical reasoning and individualized and precision care.
Finally, severity classification remains problematic. Current tools used to categorize carpal tunnel syndrome severity lack sufficient validity, which may further contribute to heterogeneity in study populations and affect the interpretation of intervention outcomes.
Take-home messages
- Carpal tunnel syndrome diagnosis remains clinical and multifactorial, as there is still no true gold standard. Physiotherapists must combine subjective history, objective testing, and clinical reasoning rather than rely on a single test.
- No single test is sufficient for carpal tunnel syndrome diagnosis. Provocative tests (Phalen, Tinel, Durkan) should be used as part of a broader assessment, with the carpal compression (Durkan) test showing the highest diagnostic utility.
- Validated questionnaires improve diagnostic accuracy, especially the Katz and Stirrat hand symptom diagram and the Carpal Tunnel Syndrome-6 (CTS-6), which integrates subjective and objective findings and increases diagnostic probability.
- Sensory testing is essential for grading impairment, not confirming diagnosis. The Semmes-Weinstein monofilament test and two-point discrimination are the most reliable measures for assessing severity and sensory loss.
- Electrodiagnostic testing (EDX) and ultrasound are helpful but imperfect.
-
- EDX assesses large-fiber function but misses small-fiber involvement and may yield normal results in symptomatic patients.
- Ultrasound detects structural changes but lacks standardized severity classification.
- Carpal tunnel syndrome is not purely local. Clinicians should screen for proximal involvement (cervical spine, double crush mechanism) and consider overlapping neuropathic conditions.
- Pain is often a major component, and psychosocial factors (catastrophizing, anxiety, depression) can significantly influence symptom severity and outcomes.
- Risk factors are consistent and clinically relevant: female sex, age, obesity, and repetitive forceful manual work increase likelihood of carpal tunnel syndrome.
- Combining tests improves diagnostic accuracy. A test battery approach (history + clinical tests + CTS-6 ± imaging) is more reliable than isolated findings.
- Clinical classification of severity remains inconsistent, meaning physiotherapists should prioritize functional impact and patient presentation over rigid staging systems.
Reference
Watch two 100% Free Webinars on Shoulder Pain and Ulna-Side Wrist Pain
Improve your Clinical Reasoning for Exercise Prescription in the Active Person with Shoulder pain with Andrew Cuff and Navigate Clinical Diagnosis & Management featuring a Case Study of Golfer with Thomas Mitchell