
Research
Chronic Pain
April 6, 2026
New Diagnostic Markers for Sensitization and Pain Inhibition Dysfunction in Fibromyalgia

Introduction
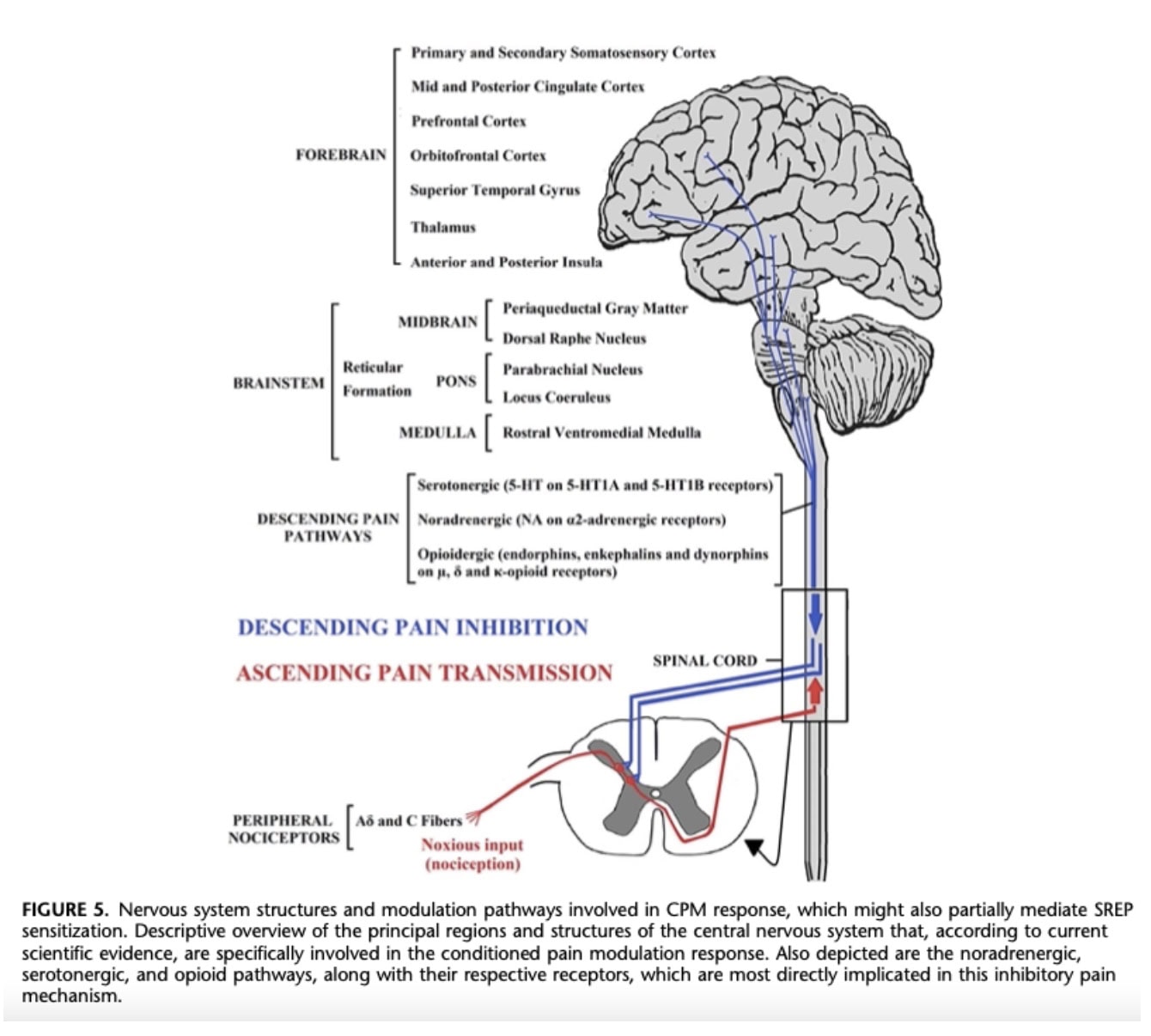
Fibromyalgia etiology remains poorly understood, and reliable diagnostic markers are still lacking. Central sensitization is thought to play a key role in pain amplification, involving both increased facilitation of ascending nociceptive pathways and impaired descending inhibitory mechanisms. Evaluating these pathways may provide valuable objective markers in both research and clinical settings, helping to better characterize underlying dysfunctions and guide targeted treatment strategies.
The slowly repeated evoked pain (SREP) protocol is a recently developed method that assesses pain amplification by measuring increases in pain ratings in response to repeated low-frequency stimuli. While temporal summation of pain (TSP) is the most commonly used clinical test, its higher stimulation frequency may primarily reflect central sensitization processes. In contrast, the lower frequency used in SREP is thought to better capture the combined contribution of both ascending facilitation and descending inhibition.
Conditioned pain modulation (CPM) is a well-established measure of endogenous pain inhibition and is consistently found to be impaired in individuals with fibromyalgia, who typically demonstrate lower CPM responses compared to asymptomatic individuals. This study aimed to investigate endogenous pain inhibition dysfunction in fibromyalgia, assessed via CPM, between individuals with fibromyalgia and pain-free controls, and to investigate the relationship between SREP sensitization and CPM responses in the fibromyalgia group. SREP may provide an indirect reflection of deficits in descending inhibitory pathways.
Methods
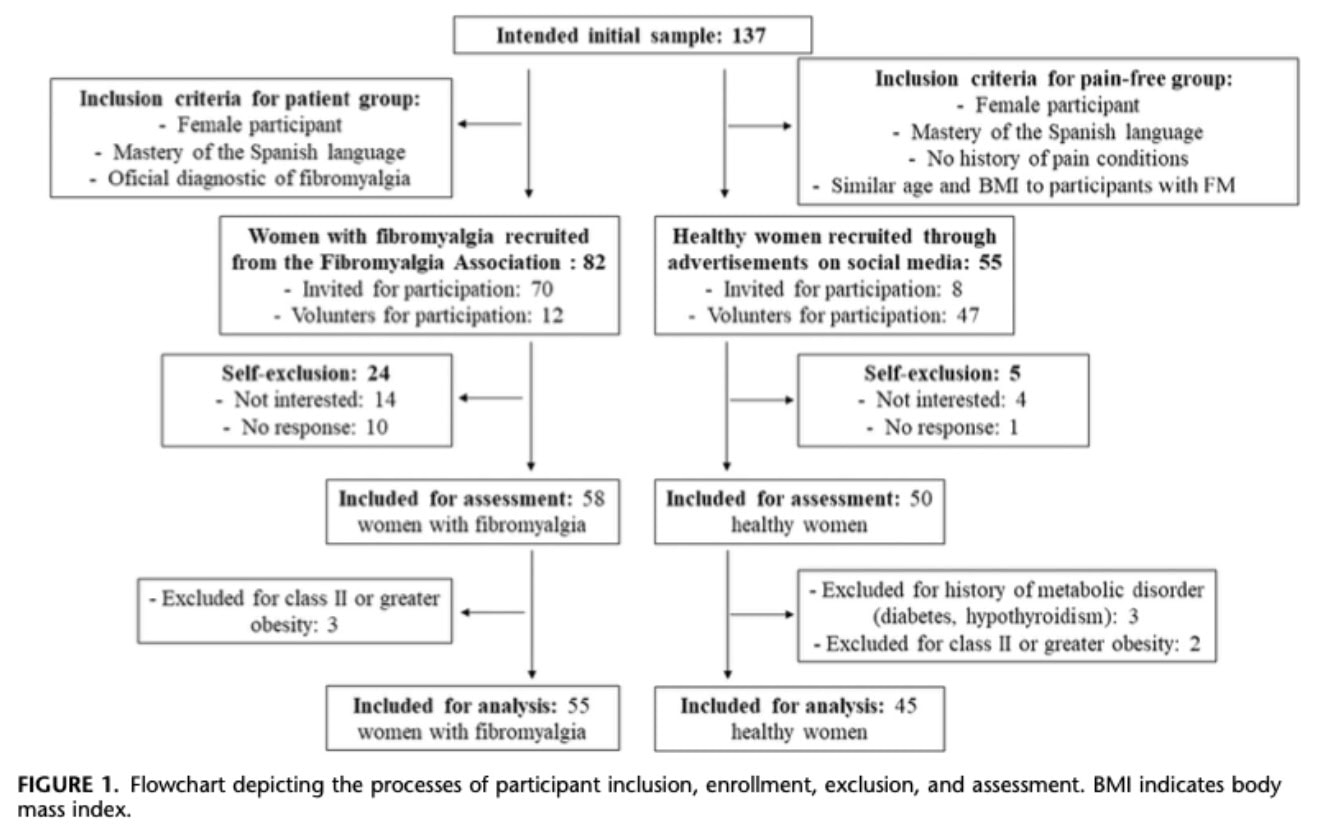
The study included 55 women with fibromyalgia (FM) and 45 age-matched pain-free women. FM participants were diagnosed by rheumatologists using the 2010 ACR criteria. Only women were included due to the higher prevalence of FM in females.
Exclusion criteria (both groups)
- Metabolic, degenerative, or cerebrovascular diseases
- Severe physical or mental disorders (e.g., cancer, psychosis, substance abuse)
- Obesity ≥ class II
- Pregnancy
Eight participants were excluded. In the FM group, mean symptom duration was 22.15 ± 10.76 years, and 40% reported comorbid pain conditions (mainly osteoarthritis, hernias, and arthritis).
Self-report Questionnaires
Clinical pain was assessed using the Brief Pain Inventory (BPI). Fatigue was measured with the Fatigue Severity Scale (FSS). Anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale (HADS), while state anxiety was assessed with the State-Trait Anxiety Inventory (STAI). Fibromyalgia severity was measured using the Revised Fibromyalgia Impact Questionnaire (FIQ-R), with a mean score of 64.82 ± 17.43.
Experimental Pain Measures
Pressure Pain Threshold & Tolerance
Measured using a computer-controlled algometer applied to the third fingernail of the nondominant hand (rate: 1 kg/s). Pain threshold (“first pain”) and tolerance (“maximum tolerable pain”) were each assessed twice, and mean values were used.
Slowly Repeated Evoked Pain (SREP)
Nine identical pressure stimuli (5 s, every 30 s) were applied at an individually calibrated intensity based on threshold and tolerance. Pain was rated (0–10) after each stimulus. Sensitization was calculated as the difference between the last and first ratings (T9–T1), with higher values indicating increased pain sensitization.
Conditioned Pain Modulation (CPM)
CPM was used to assess endogenous pain inhibitory capacity through a “pain inhibits pain” paradigm. A conditioning stimulus was applied via interdigital web pinching (between the third and fourth fingers of the dominant hand) using an algometer. Pressure was gradually increased until participants reported a pain intensity of 6/10 on a numerical scale, then maintained for 30 seconds.
During this conditioning stimulus, a test stimulus (pressure pain threshold) was applied to the third fingernail of the nondominant hand using the same procedure as baseline. Pain thresholds were measured before (Tnc) and during (Tc) the conditioning stimulus. The CPM response was calculated as the difference between thresholds (Tc − Tnc), where positive values indicate effective endogenous pain inhibition.
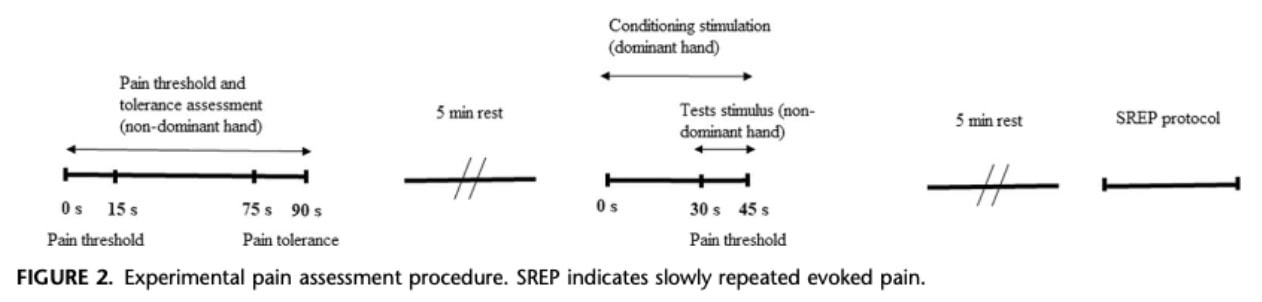
Procedure
Participants first completed clinical questionnaires, followed by a familiarization phase to ensure understanding of pain threshold, tolerance, and the pain rating scale (VNS). Pain threshold assessments (with and without conditioning pain) were performed in a counterbalanced order, separated by a 5-minute rest period. The SREP protocol was conducted 5 minutes after the CPM assessment.
Participants were instructed to avoid analgesics for 24 hours and caffeine for 6 hours prior to testing. All provided informed consent.
Statistical Analyses
The sample size was based on previous studies to ensure sufficient statistical power. Data were normally distributed, allowing the use of parametric tests.
- CPM analysis: A two-way ANOVA compared pain thresholds before vs. during conditioning (Tnc vs. Tc) between groups (FM vs. controls). Additional t-tests compared FM patients who showed a CPM response (Tc − Tnc > 0) to those who did not.
- SREP analysis: A two-way ANOVA examined pain ratings across the 9 stimuli (T1–T9) between groups to assess pain sensitization.
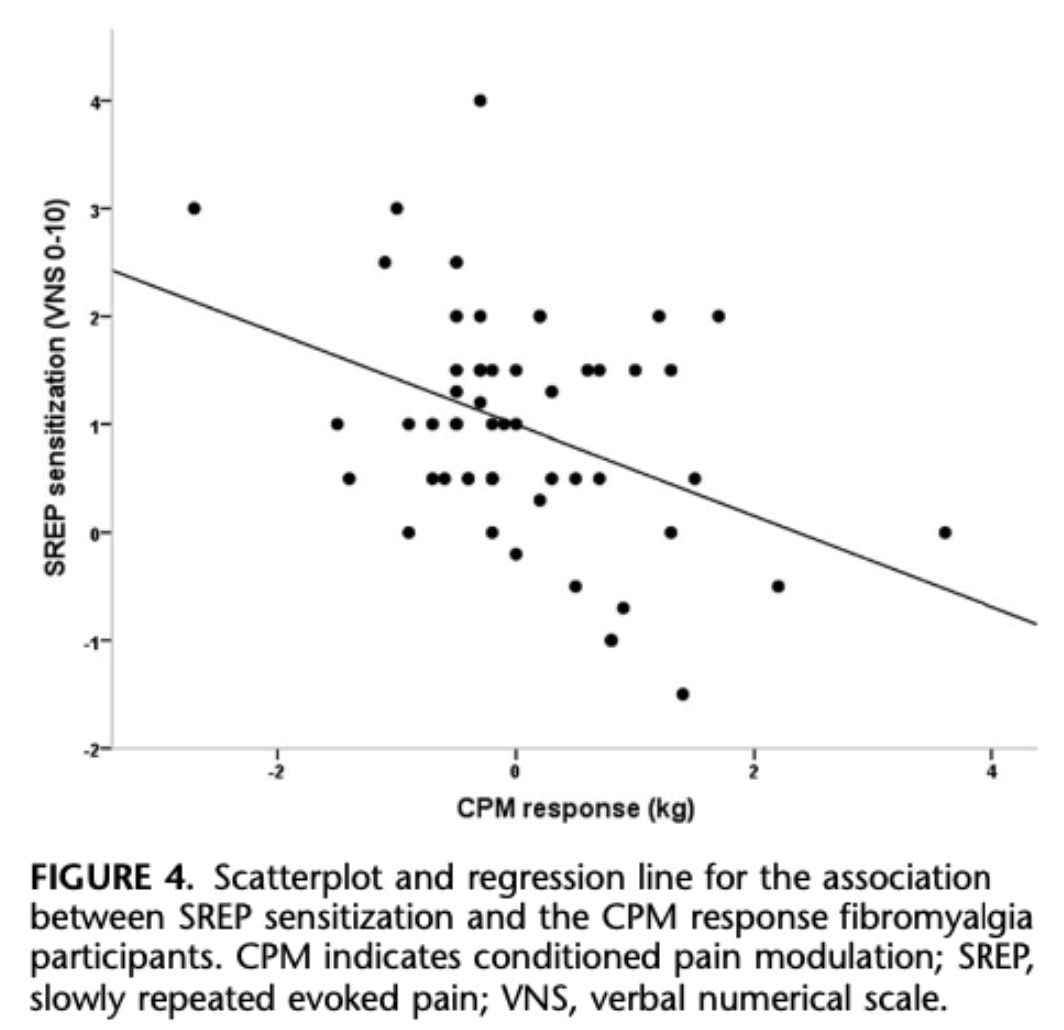
- Associations: Correlations were used to examine relationships between SREP sensitization, CPM response, and clinical variables (pain, fatigue, etc.), with confidence intervals estimated via bootstrapping.
- Prediction model: A multiple regression analysis tested whether CPM response, pain intensity (BPI), and fatigue (FSS) predicted SREP sensitization.
Results
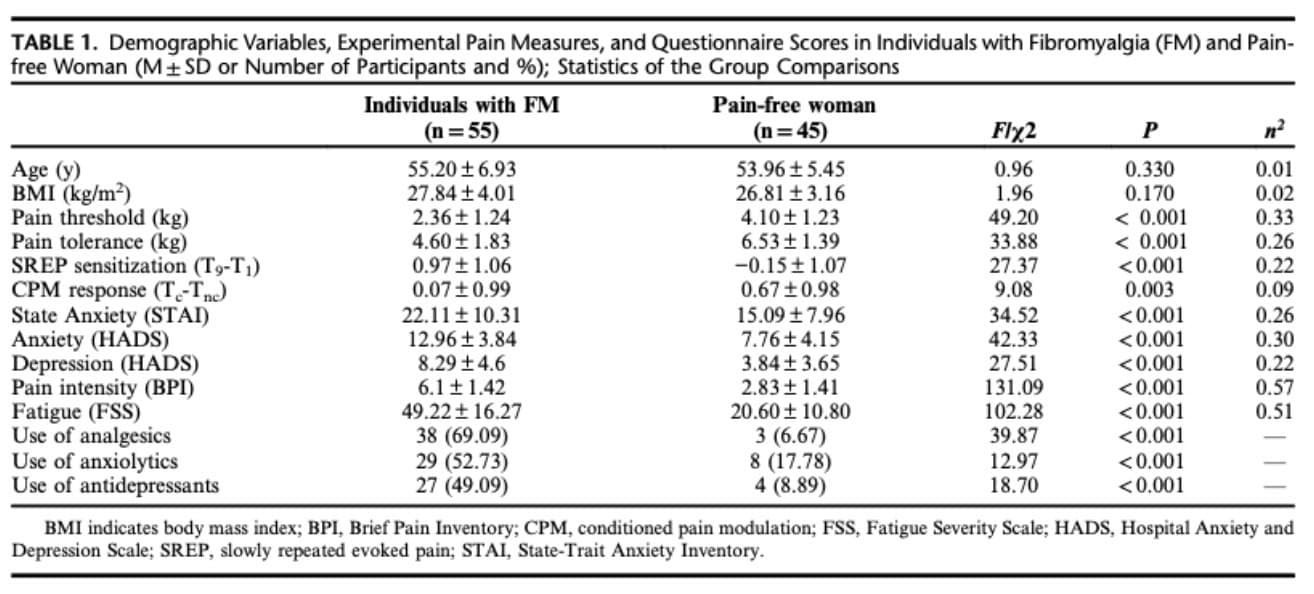
Women with fibromyalgia (FM) showed a more severe clinical profile compared to pain-free controls. They reported higher levels of pain, fatigue, and anxiety, along with lower pain threshold and tolerance, greater SREP sensitization, and a reduced CPM response (weaker pain inhibition).
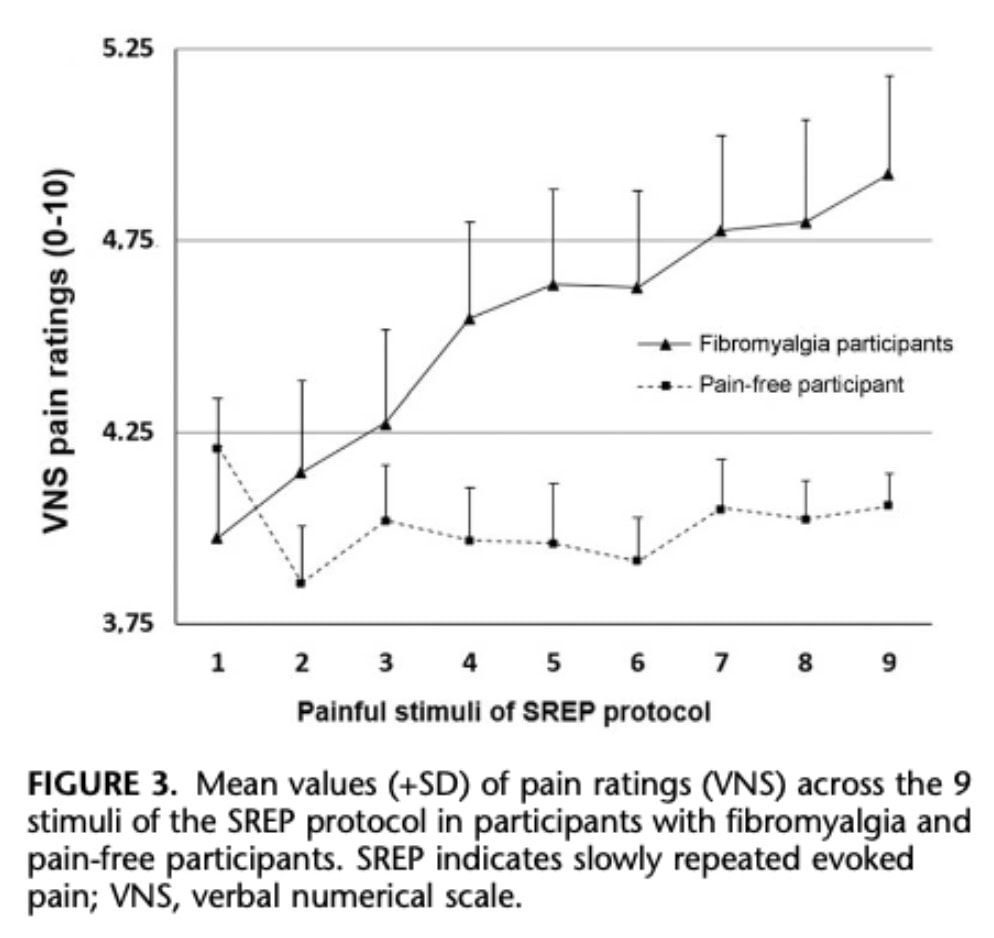
Regarding pain sensitization, pain ratings increased across repeated stimuli in the whole sample. However, this effect differed between groups:
- FM group: significant increase in pain over time, indicating clear sensitization
- Control group: no significant increase
This indicates that enhanced temporal pain sensitization is specific to FM.
For pain inhibition dysfunction in fibromyalgia, results from the CPM paradigm showed a clear group difference. Healthy participants demonstrated effective endogenous pain inhibition, whereas this mechanism was impaired in FM:
- 40% of FM patients showed a CPM response
- 80% of controls showed a CPM response
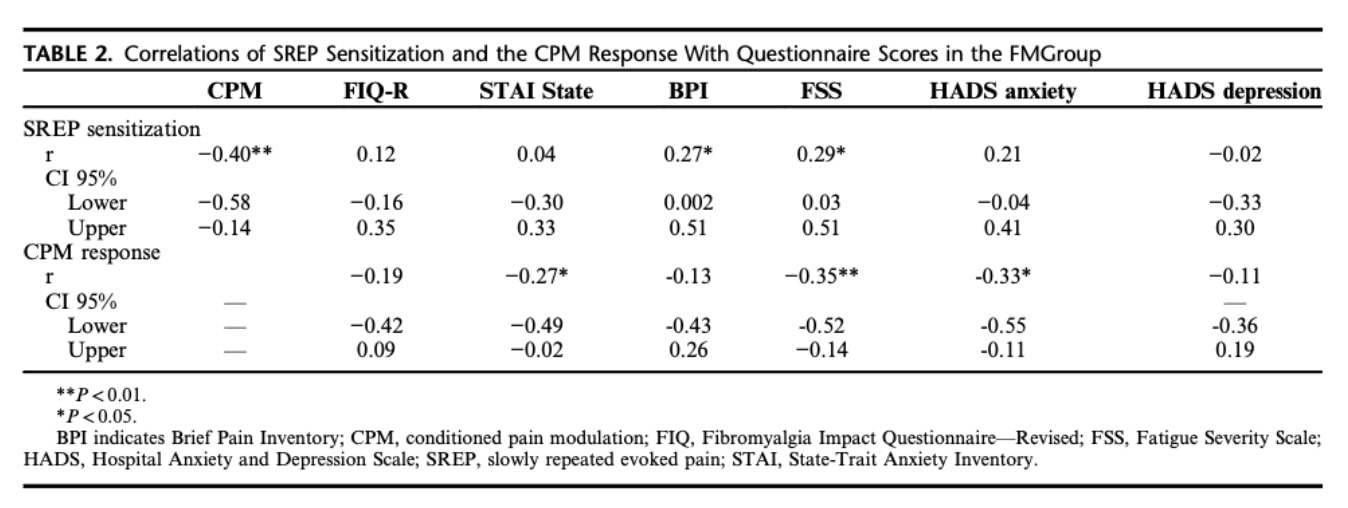
In the FM group, associations between variables revealed that:
- Higher fatigue was linked to:
- Greater SREP sensitization
- Reduced CPM response
- Higher pain intensity was associated with increased SREP sensitization
- Higher anxiety was associated with poorer CPM response
A regression analysis further showed that CPM response was the only significant predictor of SREP sensitization, suggesting that pain inhibition dysfunction in fibromyalgia contributes directly to increased pain sensitization.
When comparing FM patients based on CPM response:
- Those without a CPM response had:
- Higher symptom severity (fatigue, anxiety, overall impact)
- Lower pain tolerance
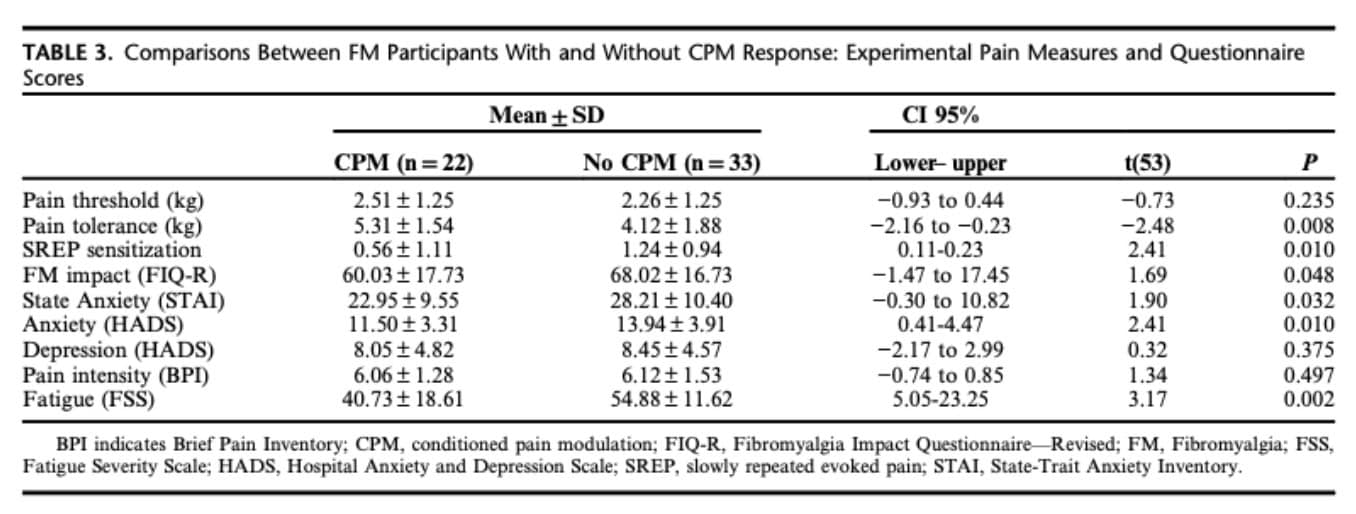
Finally, the presence of additional pain-related comorbidities did not significantly influence pain measures or clinical symptoms.
Overall, the findings suggest that fibromyalgia is characterized by a combination of enhanced pain sensitization and pain inhibition dysfunction in fibromyalgia, with these mechanisms appearing closely interrelated.
Questions and thoughts
The pathophysiological mechanisms underlying fibromyalgia remain poorly understood. As a result, many women may receive a fibromyalgia diagnosis in the absence of a clear medical explanation for their symptoms. In this context, fibromyalgia can become a “convenience diagnosis”, providing both a label for patients and a clinical starting point for practitioners. However, several other conditions—such as myofascial pain syndrome or small fiber neuropathy —can present with similar symptoms and are frequently underdiagnosed, particularly in women.
This raises broader concerns about sex disparities in healthcare, where women’s symptoms are often under-recognized or misinterpreted, leading to delayed or less precise diagnoses. The relative lack of research in female-predominant conditions further contributes to this issue.
The broad and non-specific definition of fibromyalgia also calls into question the inclusion criteria used in this study. Participants were diagnosed based on the 2010 American College of Rheumatology (ACR) criteria, which rely on symptom-based measures (WPI and SS scores) and the absence of another explanatory condition. While practical, these criteria encompass a heterogeneous patient population and may blur distinctions between fibromyalgia and other chronic pain conditions.
Moreover, the absence of a gold standard for diagnosis limits the evaluation of the psychometric validity of these criteria. They have been widely criticized for their lack of specificity, potentially reinforcing a diagnosis of exclusion and complicating differential diagnosis.
Although the experimental pain measures used in this study (e.g., SREP, CPM) are not diagnostic tools, they provide valuable insights into pain inhibition dysfunction in fibromyalgia, particularly regarding sensitization and pain modulation. These assessments may help clinicians, especially physiotherapists, to better tailor interventions. However, their lack of specificity to fibromyalgia should be acknowledged, as similar alterations may be present in other chronic pain conditions.
Talk nerdy to me
As the underlying pathophysiological mechanisms of fibromyalgia remain incompletely understood, recent research has increasingly focused on advances at the molecular and neurophysiological levels to better characterize the condition.
As discussed previously, the broad nature of the American College of Rheumatology (ACR) criteria raises concerns regarding their reliability, specificity, and sensitivity. This highlights the need for a more precise understanding of the mechanisms underlying fibromyalgia. In this context, central sensitization may be more objectively assessed using tools such as functional MRI (fMRI) and evoked EEG potentials, particularly to explore alterations in descending pain inhibitory pathways.
Transcutaneous electrical nerve stimulation (TENS) has also been investigated as a potential therapeutic approach. Some studies suggest that TENS may reduce central nervous system excitability by enhancing descending inhibitory mechanisms. For instance, a placebo-controlled trial reported that a single session of TENS increased conditioned pain modulation (CPM) and reduced both pain and fatigue in patients with fibromyalgia. However, recent systematic reviews report mixed findings regarding its overall effectiveness on pain reduction. The mitigated results on TENS effect on pain could be further explained by the lack of reliable diagnostic criteria and other contributing factors.
The mechanisms underlying TENS are traditionally explained by the Gate Control Theory, whereby stimulation of non-nociceptive Aβ afferent fibers inhibits ascending nociceptive input at the spinal level. In addition, TENS is thought to activate descending inhibitory pathways, which may explain its potential effects on CPM and pain modulation.
More recently, the role of the immune system in fibromyalgia has gained attention, particularly the involvement of neutrophils. These first-line immune cells appear to be more active in individuals with fibromyalgia, contributing to a state of low-grade systemic inflammation. Neutrophils release pro-inflammatory cytokines such as IL-6, IL-8, and TNF-α, which are known to sensitize nociceptive pathways. Altogether, these findings contribute to a more integrated understanding of fibromyalgia pathophysiology and may help guide the development of targeted pharmacological and non-pharmacological interventions.
Take-home messages
Fibromyalgia should not be viewed solely as a peripheral pain condition, but rather as a disorder of pain processing, characterized by a combination of increased pain sensitization and pain inhibition dysfunction in fibromyalgia.
- Assess beyond pain intensity. Patients with fibromyalgia present altered pain modulation:
- ↑ Sensitization (SREP)
- ↓ Inhibitory capacity (CPM)
Consider integrating simple clinical proxies of pain modulation (e.g., response to repeated stimuli, flare-ups, recovery time).
- Tailor treatment to the nervous system, not just tissues. Interventions should aim to:
- Reduce central excitability
- Enhance descending inhibition
Think graded exposure, gradual exercising, pain education, pacing, rather than purely structural approaches.
- Identify subgroups of patients. Patients with impaired pain inhibition (low CPM):
- Tend to have worse symptoms (fatigue, anxiety, severity)
- May respond differently to treatment → Personalization of care is key.
- Leverage treatments targeting pain modulation. Modalities such as:
- Exercise
- TENS
- Cognitive and behavioral approaches may work partly by enhancing descending inhibitory pathways.
- Consider psychosocial contributors. Fatigue and anxiety are strongly linked to:
- ↑ Sensitization
- ↓ Inhibition → Reinforces the need for a biopsychosocial approach
- Be cautious with the diagnosis. Fibromyalgia is a heterogeneous and non-specific label:
- Always screen for differential diagnoses
- Avoid reducing the patient to the label alone
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Watch this FREE video lecture on Nutrition & Central Sensitisation by Europe’s #1 chronic pain researcher Jo Nijs. Which food patients should avoid will probably surprise you!
