
Research
Ankle/Foot
August 14, 2025
Sinus Tarsi Syndrome: Diagnosis, Treatment & Rehabilitation Strategies

Introduction
Sinus tarsi syndrome (STS) refers to pain localized in the lateral tarsal sinus, often associated with hindfoot instability. However, its definition remains vague, and its exact cause is still unclear. First described as lateral foot pain following trauma, sinus tarsi syndrome has been observed in athletes (e.g., dancers, basketball and volleyball players) and individuals with flatfoot or obesity. Despite numerous reports, no clear consensus exists regarding its etiology, pathomechanics, or standardized diagnostic criteria.
Sinus tarsi syndrome treatment can vary widely—from conservative management like corticosteroid injections to surgical options such as denervation, debridement, or subtalar stabilization. Yet, due to its poorly defined nature, sinus tarsi syndrome remains a controversial condition without a unified treatment algorithm.
This review aims to clarify the anatomy of the tarsal sinus, the biomechanics of the subtalar joint, potential causes and differential diagnoses, current evaluation and sinus tarsi syndrome treatment algorithm strategies.
Methods
This narrative review, conducted in September 2022, involved an extensive search of medical databases. As the study was designed as a critical rather than a systematic review, PRISMA guidelines were not applied. The objective extended beyond identifying literature specific to sinus tarsi syndrome; it also included related topics. Full-text articles were obtained, and reference lists were screened for additional relevant studies and book chapters. The gathered literature was summarized and critically analyzed, focusing on sinus tarsi syndrome-related anatomy, biomechanics, etiology, clinical assessment, diagnosis, and treatment. The authors also included an anatomical overview and shared their clinical experience through illustrative cases.
Results
Anatomy
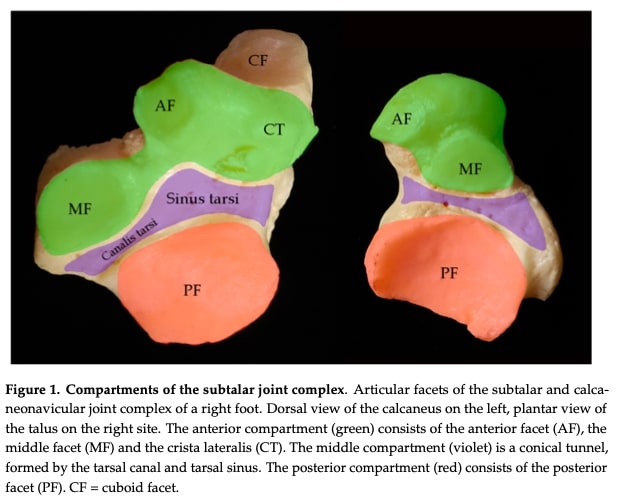
Anatomical Compartments.
The Anterior Compartment (Green) includes the anterior facet (AF), middle facet (MF), and crista lateralis (CT). It articulates with the talus to support midfoot mobility during gait.
The Middle Compartment (Violet) forms the tarsal canal/sinus (a conical tunnel containing ligaments, nerves, and vessels). This compartment is the common site of impingement/pain in sinus tarsi syndrome.
The Posterior Compartment (Red) contains the posterior facet (PF), where the convex calcaneal surface meets the concave talar surface.
The tarsal canal and sinus contain a network of ligaments, blood vessels, nerves, and soft tissues. This region receives its blood supply through anastomoses between branches of the lateral tarsal artery and the artery of the tarsal canal, which originates from the posterior tibial artery and provides the main blood supply to the talar body. The area is innervated by branches of the tibial, deep peroneal, and superficial peroneal nerves. The ligamentous structures in this region, particularly the interosseous talocalcaneal ligament, play a crucial role in maintaining subtalar joint stability.
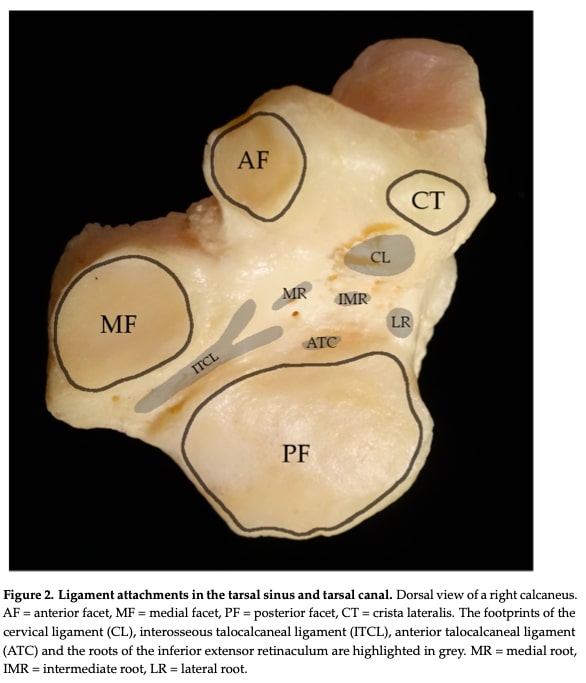
The tarsal sinus and canal contain three primary stabilizing structures: the cervical ligament (CL), the interosseous talocalcaneal ligament (ITCL), and the three roots of the inferior extensor retinaculum (IER). These work in conjunction with additional lateral stabilizers including the calcaneofibular ligament (CFL), anterior talocalcaneal ligament (ATC), and bifurcate ligament (composed of calcaneonavicular and calcaneocuboid components). Medially, stability is provided by the medial collateral ligament complex (incorporating tibionavicular, tibiospring and tibiocalcaneal portions of the deltoid ligament), anterior and posterior tibiotalar ligaments, and the spring ligament complex (comprising superomedial ligament, medial plantar oblique ligament and inferior plantar ligament). The posterior articular facets of the talus and calcaneus are substantially larger than the middle and anterior facets, with these facet systems being separated by the interosseous talocalcaneal ligament. This comprehensive ligamentous network collectively ensures proper talotarsal joint stability and function during weight-bearing activities, where the larger posterior facet bears the majority of axial loads while the smaller anterior and middle facets facilitate necessary joint mobility.
Biomechanics
Joint Structure & Motion
- The subtalar (talocalcaneal) joint is a saddle-shapedjoint with a convex upward orientation, functioning like a “mitered hinge.”
- It allows triplanar motion: inversion/supination (25–30°) and eversion/pronation (5–10°), combining with ankle dorsiflexion/plantarflexion for gait.
Implications for Gait
- Hindfoot valgus: “Unlocks” the midfoot during heel strike, enabling shock absorption.
- Hindfoot varus: “Locks” the midfoot in late stance, creating a rigid lever for push-off.
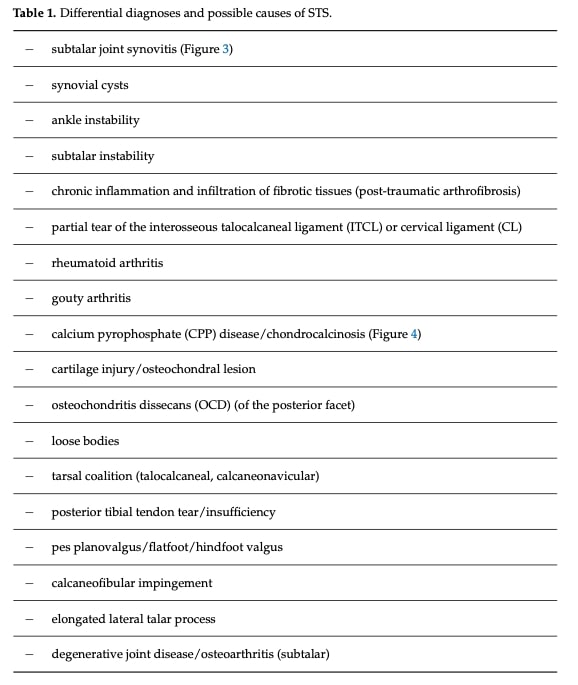
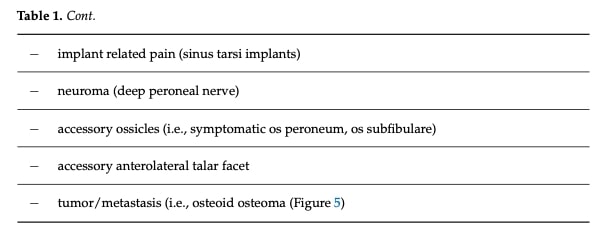
Etiology
Several causes of sinus tarsi syndrome have been proposed. Initially described by Brown in 1960 as herniated synovial membrane impingement, soft tissue compression remains a widely accepted theory. Other possible etiologies include ligament injury, sinus bleeding, talotarsal arthritis or synovitis, and chronic fibro-adipose inflammation. Lateral impingement may also result from posterior tibial tendon dysfunction, hindfoot valgus, or anatomical variations such as an accessory anterolateral facet.
Instability of the talocrural and talotarsal joints is often associated with sinus tarsi syndrome and can be classified as mechanical (due to ligament damage or avulsion) or functional (related to proprioceptive deficits, possibly from partial nerve injury). Key ligaments involved in subtalar instability include the calcaneofibular ligament (CFL) and the interosseous talocalcaneal ligament (ITCL). Sinus tarsi syndrome may result from either or both instability types, described collectively as “subtalar instability syndrome,” which involves either impaired neuromuscular control or ligamentous insufficiency.
Vascular mechanisms have also been suggested: trauma may induce fibrotic changes in the venous structures of the sinus tarsi, impairing venous drainage and increasing intrasinusal pressure.
Additionally, nociceptive and proprioceptive dysfunctions are implicated in sinus tarsi syndrome. The sinus tarsi is richly innervated, primarily by branches of the deep peroneal and sural nerves, and contains a high density of mechanoreceptors (free nerve endings, Ruffini endings, Pacinian corpuscles, and Golgi-like endings). This indicates that the sinus tarsi serves as both a mechanical and sensory organ, contributing to foot and ankle proprioception and possibly playing a central role in sinus tarsi syndrome pathophysiology.
History and physical examination
Subjective Findings (Patient History & Symptoms).
A comprehensive history is essential due to the diverse etiologies of sinus tarsi pain. Key points include:
- Pain characteristics: location (typically over the sinus tarsi), duration, aggravating factors (e.g., sports activity), and timing.
- Functional limitations: difficulty participating in sports, walking on uneven surfaces, or performing dynamic movements.
- History of instability: common complaints include sensations of “giving way” or “rolling over,” recurrent swelling, and instability.
- Trauma and prior interventions: any previous foot/ankle injuries, surgeries, or treatments.
- Associated conditions: clinicians should rule out differential diagnoses such as infection, arthritis, or gout.
Notably, all patients with STS typically report localized tenderness in the sinus tarsi region.
Objective Findings (Clinical Examination & Testing)
A detailed physical exam should include:
- Inspection: Assess for swelling, redness, or warmth in the hindfoot.
- Hindfoot alignment and gait: Observe for deformities or abnormal gait patterns; evaluate peroneal muscle activity.
- Neurovascular status: Perform a thorough neurovascular assessment of the foot.
- Palpation: Tenderness in the sinus tarsi, especially during dynamic hindfoot eversion, may indicate impingement.
Stability Testing:
- ATFL (Anterior Talofibular Ligament): Anterior drawer test in 20° plantarflexion.
- CFL (Calcaneofibular Ligament): Anterior drawer in neutral dorsiflexion with varus stress.
- Subtalar joint: Anterior drawer in 90° dorsiflexion and varus stress with the ankle stabilized to assess for hyperlaxity.
- Midfoot: Assess for excessive inversion/eversion to rule out midfoot instability.
- Strength testing: Evaluate peroneal muscle function, which contributes to dynamic joint stabilization.
Special Clinical Indicators:
- Dynamic impingement test (proposed by the senior author): Pain elicited during hindfoot eversion with simultaneous palpation of the sinus tarsi suggests impingement.
- Diagnostic/therapeutic injection: Pain relief after local anesthetic or corticosteroid injection into the sinus tarsi strongly supports the diagnosis of sinus tarsi syndrome.
Complementary Clinical Exams and Imaging – Implications for Physical Therapists
Standard Radiographs
Weight-bearing AP and lateral X-rays are useful to detect structural deformities such as planovalgus alignment, which may contribute to altered biomechanics and sinus tarsi syndrome symptoms.
While specialized views (Broden, Harris–Beath, Saltzman) and stress radiographs can offer additional detail, they are rarely used in standard practice due to limited diagnostic accuracy.
Advanced Imaging
Since subtalar joint structures are complex and not well visualized on plain films, cross-sectional imaging is often needed when symptoms persist or underlying pathology is suspected:
CT scans (especially weight-bearing when available) are used to assess bony abnormalities, such as:
-
- Hindfoot malalignment
- Bony impingement
- Tarsal coalitions or arthritic changes
This can inform orthotic decisions or indicate need for surgical referral.
MRI is the imaging modality of choice to explore soft tissue causes of sinus tarsi syndrome:
- Detects ligament injuries (e.g., CFL, ITCL), synovitis, scar tissue, or tendon pathologies.
- Also identifies bone marrow changes (bruising, contusion) from altered loading.
MRI is sensitive but not always specific, which underscores the importance of clinical correlation.
SPECT-CT may identify increased bone activity (e.g., in impingement syndromes), though it remains rarely used in routine settings.
Diagnostic Injections
- A therapeutic trial of anesthetic or corticosteroid injection into the sinus tarsi can help confirm the diagnosis if it relieves symptoms.
- Injections are typically performed under imaging guidance and may guide interdisciplinary treatment planning.
Arthroscopy
- Subtalar arthroscopy allows for direct assessment of the joint and is the most accurate method to confirm intra-articular causes (e.g., ligament tears, arthrofibrosis).
- MRI may miss certain ligamentous injuries, highlighting arthroscopy’s diagnostic value when conservative care fails.
Treatment
Most authors agree that the initial sinus tarsi syndrome treatment should be non-operative. Common conservative approaches include corticosteroid or local anesthetic injections into the sinus tarsi, activity modification, and physiotherapy. Taillard et al. reported that approximately two-thirds of patients responded well to these non-surgical interventions.
When conservative treatment fails to alleviate symptoms, surgical options may be considered. Historically, open decompression of the sinus tarsi—often involving removal of structures within the lateral portion of the sinus—has shown success in reducing symptoms in up to 90% of cases although details about the exact structures removed are often lacking in older studies.
Other surgical approaches include open denervation of the terminal branches of the deep peroneal nerve, which has been associated with good outcomes, including pain relief and return to normal activity in the majority of patients. More recently, arthroscopic decompression has gained popularity as a minimally invasive alternative for sinus tarsi syndrome treatment. This technique is described as technically straightforward and offers the advantage of allowing both diagnosis and treatment during the same procedure. It is also associated with quicker recovery times and a safe profile, making it an increasingly preferred option for patients with persistent sinus tarsi pain.
Questions and Thoughts
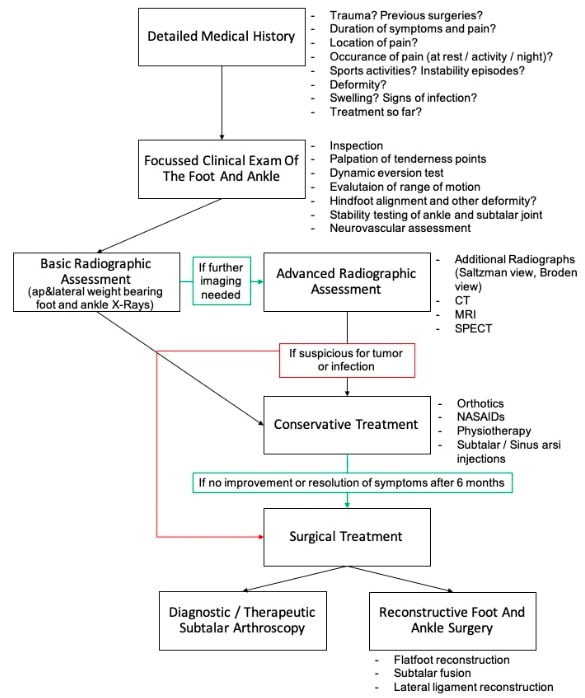
The authors propose a structured treatment algorithm for managing sinus tarsi syndrome, offering a comprehensive overview of the clinical care pathway. Basic radiographic imaging is systematically recommended, underscoring the importance of interdisciplinary collaboration, especially as physiotherapists may lack the authority to order advanced imaging. However, one might argue that an initial six-month trial of conservative management, tailored to clinical examination findings, is appropriate before considering further investigations, as early radiographic results may not directly influence initial sinus tarsi syndrome treatment decisions. Close collaboration with radiologists and physicians remains crucial, particularly if the patient’s clinical progression does not follow the expected course.
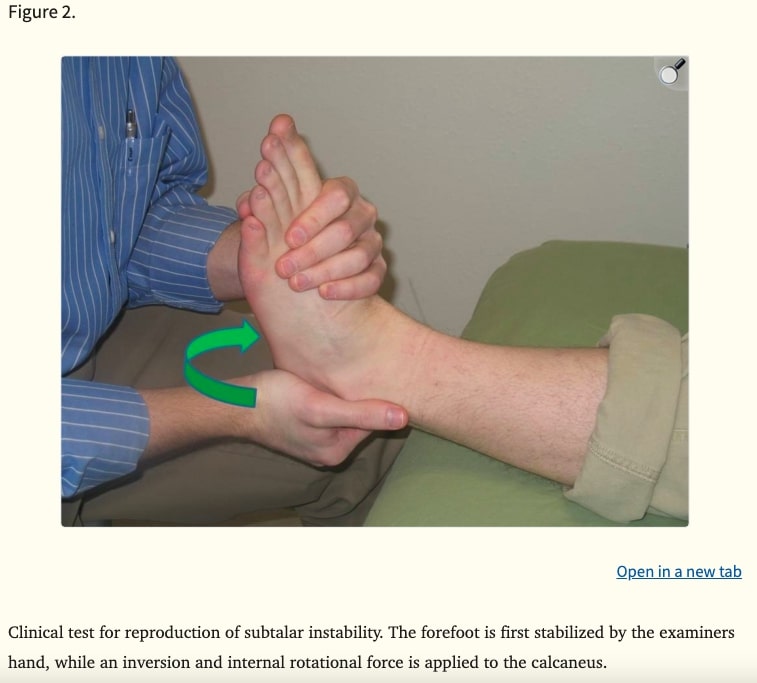
Assessment of Subtalar Joint StabilitySubtalar joint stability is commonly assessed by applying medial and lateral glides of the calcaneus over a fixed talus, as well as through joint distraction. A specific test described by Therman et al. positions the athlete supine, with the ankle in slight dorsiflexion to stabilize the talocrural joint. The examiner applies inversion and internal rotation to the calcaneus while stabilizing the forefoot, followed by an inversion force on the forefoot. A positive test is indicated by excessive medial calcaneal shift and reproduction of the athlete’s symptoms of instability.
Conservative Management of Sinus Tarsi Syndrome
The term sinus tarsi syndrome encompasses a wide variety of underlying pathologies. Therefore, the clinician must accurately identify the specific pathology to inform the treatment strategy. When physiotherapists suspect sinus tarsi syndrome during patient evaluation, the clinical focus should first determine whether the patient presents with signs of proprioceptive deficits or stability issues.
Sinus tarsi syndrome is frequently associated with Chronic Ankle Instability (CAI), and the clinical examination should help clarify whether sinus tarsi syndrome contributes to the patient’s symptoms. If inflammation or synovitis is suspected, further imaging may be warranted to confirm the diagnosis. Non-steroidal anti-inflammatory drugs (NSAIDs) have been considered in a narrative review with clinical commentary a relevant solution to manage inflammation.
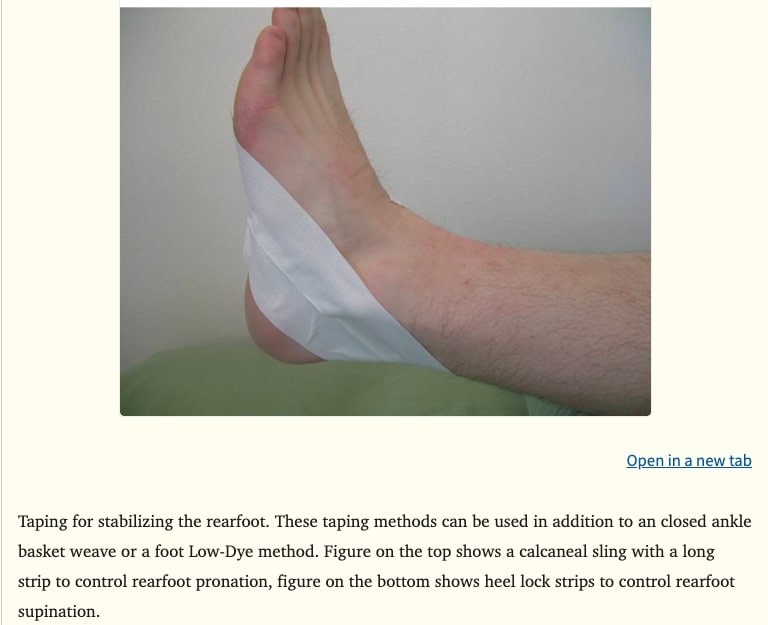
Furthermore, this same review on conservative sinus tarsi syndrome treatment suggests the following interventions: proprioceptive and balance training, muscle strengthening, bracing, taping, and foot orthoses. Orthotics may limit excessive subtalar joint motion. Recommendations include using rigid midsole footwear with a straight last and firm heel counter, although these are general sports shoe recommendations rather than sinus tarsi syndrome treatment specific guidelines. Taping techniques aimed at limiting subtalar and midfoot motion, particularly excessive pronation, have been described but evidence regarding their specific effectiveness for sinus tarsi syndrome remains limited. The taping application used in this study is presented below.

Stability Training as a Core InterventionStability training remains central to sinus tarsi syndrome treatment, considering the wide range of possible etiologies including herniated synovial membrane impingement, soft tissue compression, ligament injury, sinus bleeding, talotarsal arthritis or synovitis, and chronic fibro-adipose inflammation. Rehabilitation should target the impaired structures. Dynamic stability must be emphasized to compensate for passive stability deficits— Interestingly, a recent literature review revised the conceptual model of CAI, offering a comprehensive overview of the interconnected consequences of CAI on patient outcomes. Proprioceptive training and improving the reactive contraction times of muscles involved in subtalar motion are key objectives.
Phased Rehabilitation Approach
The narrative review with clinical commentary exploring conservative management for sinus tarsi syndrome suggests a three-phase rehabilitation model for conservative sinus tarsi syndrome treatment:
Attain phase: Starts with single-leg standing exercises to promote ankle balance and subtalar joint stability, initially with eyes open then progressing to eyes closed. The focus is on preventing excessive pronation and maintaining a stable foot and rearfoot position.
Maintain phase: Adds perturbations to challenge the stabilizer muscles of the ankle, starting with contralateral hip movements in different planes. The goal is to enhance dynamic balance and avoid compensations at the hip or rearfoot.
Additional balance and strength exercises: Uses star excursion balance tests, heel raises, theraband oscillations, and ball catching/throwing to further develop concentric and eccentric control of the ankle and subtalar joint under external perturbations.
Sustain phase: Introduces closed chain activities like lunges and step-downs to build feedforward motor control and ensure proper knee-foot alignment while minimizing excessive subtalar motion.
Sustain phase progressions: Advances to hopping, jumping, and running drills, including pivoting and cutting maneuvers at low speed, ensuring controlled foot and leg alignment without rearfoot instability.
Return to play criteria: Based on the athlete’s ability to perform multidirectional and high-speed movements without symptoms. A gradual return to sport-specific activities is recommended to prevent recurrence of sinus tarsi inflammation.
Talk nerdy to me
The critical review discussed offers an in-depth synthesis of sinus tarsi syndrome-related anatomy, biomechanics, etiology, clinical assessment, diagnosis, and treatment. While comprehensive, its design presents limitations. The absence of statistical analyses, likely due to the limited amount of available data, prevents reporting of effect sizes and tools such as forest plots (common in systematic reviews) that enhance data reproducibility could not be applied.
Additionally, the critical review design is prone to selection bias (study choices reflecting reviewer preferences), confirmation bias (favoring findings supporting personal experience), and publication bias (preference for positive or well-known results).
The narrative review with clinical commentary, heavily referenced for the conservative management discussion in the question and thoughts part, shares these limitations. Notably, this second review involves a single author, increasing susceptibility to bias.
Despite these constraints, both resources provide valuable foundational knowledge on sinus tarsi sydrome, helping clinicians understand, examine, and manage this condition. Clinicians are encouraged to trial proposed interventions, document patient outcomes rigorously, and contribute to developing evidence-informed patterns of care for patients with sinus tarsi syndrome.
Take home messages
Sinus tarsi syndrome is a complex, multifactorial condition
- Sinus tarsi syndrome serves as an umbrella term encompassing diverse etiologies, including ligamentous injury, synovial impingement, subtalar instability, and chronic inflammation. A thorough clinical evaluation is essential to identify the underlying pathology.
Diagnosis relies on clinical assessment but benefits from interdisciplinary collaboration
- Key diagnostic tools include localized tenderness on palpation, dynamic impingement tests, and response to diagnostic injections.
- While imaging (MRI, CT) is valuable for ruling out structural causes, early radiographic findings may not alter initial conservative management. Close collaboration with radiologists is critical for refractory cases.
Furthermore, clinical testing such as ankle anterior drawer test, and forced dorsiflexion sign. are relevant tests for ankle pain differential diagnosis.
Sinus Tarsi Syndrome can be mistaken for other conditions, with anterior ankle impingement being a key differential diagnosis to consider. The Physiotutors assessment protocol for foot and ankle disorders further supports accurate differentiation and sharpens clinical examination skills.
Conservative management is first-line but requires structured rehabilitation
- A 6-month trial of targeted sinus tarsi syndrome treatment (e.g., proprioceptive training, bracing, NSAIDs) is recommended before pursuing advanced diagnostics or surgery.
- Rehabilitation should follow a phased approach (Attain → Maintain → Sustain), emphasizing dynamic stability and sport-specific progressions.
This physiotutors youtube video will provide you with various treatment ideas ranging from mobilization technique to stability and jumps exercises for ankle sprain.
Surgical options are reserved for refractory cases
- Arthroscopic decompression has emerged as a minimally invasive and effective option, offering both diagnostic and therapeutic benefits.
Gaps in evidence persist
- Limited high-quality studies exist on specific sinus tarsi syndrome treatment (e.g., taping, orthotics). Clinicians should document outcomes to contribute to the evidence base.
- Future research should focus on standardized diagnostic criteria and tailored treatment algorithms.
Reference
THE ROLE OF THE VMO & QUADS IN PFP
Watch this FREE 2-PART VIDEO LECTURE by knee pain expert Claire Robertson who dissects the literature on the topic and how it impacts clinical practice.
