Research
Exercise
September 19, 2023
Who benefits from aerobic + neck exercise? Predicting treatment success in neck pain

Introduction
In every patient you meet, you’ll try to determine the best approach for them to get better and hopefully soon. Some patients will have a strong treatment preference, and generally speaking, many of them would prefer or expect a passive approach. It is up to you to set out the lines of treatment and you’ll base your choices on what you’ve learned, what the patient would prefer, on the available evidence, and possibly, sometimes on your best available guess. Predicting how your treatment can be a success can be hard because many variables may be involved. Some people have longstanding issues, some may have high levels of pain or their pain may radiate towards other body regions. Which treatment approach would you choose? Predicting treatment success in neck pain is important as it gives us the information we need to tailor our interventions. That is what this study aimed to do by trying to predict who would benefit from performing aerobic exercise besides neck strengthening. Read on for more!
Methods
Predicting treatment success in neck pain can be important in determining which treatment approach to use in a particular patient, as there are many treatments available to relieve neck pain and its consequences. The data from this secondary analysis came from a RCT by Daher et al., (2020), which we reviewed recently.
Briefly, the participants were randomly assigned to perform neck strengthening exercises (control) or to the intervention group performing the addition of aerobic exercise to neck strengthening. It was a double-blind study including patients with nonspecific neck pain that had been lasting for at least 4 weeks, with and without referred pain. They had at least mild functional disabilities, representing a minimum score of 10/50 on the Neck Disability Index (NDI) questionnaire. Further, the population was sedentary.
The participants in both groups completed 6 weeks of training, with 2 supervised sessions per week. For the details about the exercise programs, we suggest you take a look at our previous research review. In this trial, the combination of aerobic and strength training resulted in 80% of the participants having a successful treatment outcome.
To develop the prediction model, candidate predictor variables were selected from clinical experience, published systematic reviews, prospective studies on prognostic factors for neck pain, and variables that significantly differed between the groups in the primary study. The primary outcome was the same as in the original study: the Global Rating of Change (GROC), where treatment success was defined as people reporting +5 or more after the study. The outcomes were dichotomized to whether or not treatment success was obtained.
The possible candidate predictor variables were then tested for their relationship with the presence or absence of treatment success via univariable regression analyses. When there was a relation, the significant predictor variables were tested through backward multivariate regression analysis. The variables that showed significance in this analysis were used to develop a clinical prediction rule to predict treatment success in neck pain patients who participate in aerobic training combined with strengthening. Sensitivities and specificities were calculated using the Receiver Operating Characteristic curve (ROC) to obtain the best cut-off values.
Results
So, when must we prescribe aerobic exercise combined with neck-specific exercises to obtain treatment success in neck pain patients?
A total of 139 participants were included in the study. They had suffered on average 222 days of nonspecific neck pain. Their mean NDI score was 16, their neck pain was of a mean VAS intensity of 6.7/10, and almost 40% had neck pain referring beyond the neck. They had moderate to high pain-related anxiety, especially for physical activity and work as reflected in the rather high FABQ scores:
- FABQ score of 33.5 (SD: 9.3); Maximum score = 96
- FABQ-Physical Activity score of 12.7 (SD: 4.1); Maximum score = 24 and
- FABQ-Work score of 20.8 (SD: 7.7). Maximum score = 42
After 6 weeks of aerobic exercise combined with strengthening, more than 60% of the participants reported a GROC of +5 or more, reflecting a successful outcome. This increased to 77% at 6 months. 6 variables were significantly different between the participants who had a successful outcome and those who did not:
- Duration of symptoms since onset,
- NFE test result,
- NDI,
- FABQ-Physical Activity score,
- VAS score,
- Active range of motion for neck extensionAbsence of referred pain
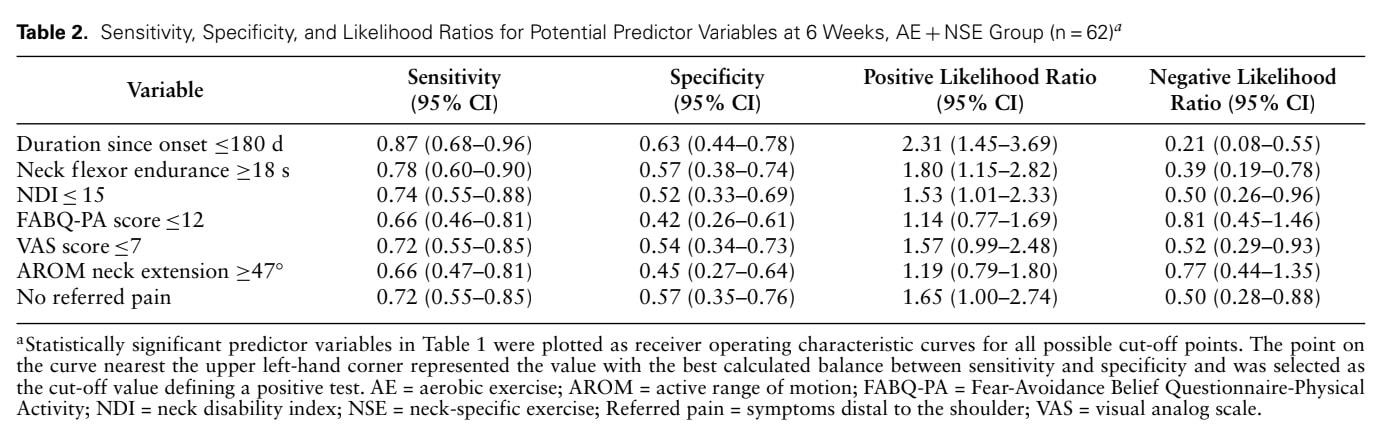
The ROC determined the following cut-off values:
- Duration of symptoms since onset ≤180 days,
- NFE test result ≥18 seconds,
- NDI ≤15,
- FABQ-Physical Activity score ≤12,
- VAS score ≤7,
- Active range of motion for neck extension ≥47 degrees.
They came along with the most optimal values for sensitivity and specificity as depicted hereunder.
From the final regression analysis, the following 3 candidate predictor variables remained significant:
- Duration of symptoms ≤6 months (180 days),
- NFE test result ≥18 seconds
- Absence of referred pain
The above 3 variables were analyzed to identify the outcome of interest. The positive likelihood ratio was 2.30 (95% CI, 1.40 to 3.77) if 2 of the 3 variables were present. This means that a patient with 2 of the 3 variables positive was 2.3 times more likely to achieve treatment success with aerobic exercise added to strengthening than a patient without those variables present. The post-test probability of success was 84.0%.
If all 3 variables were present, the positive likelihood ratio was slightly lower: 1.87 (95% CI = 1.37 to 2.57). A patient with all 3 variables was 1.8 times more likely to achieve success by adding aerobic exercise on top of the strengthening program for neck pain than a patient without. The post-test probability of success was 94.0%.
Questions and thoughts
- These outcomes were quite stable as almost 90% of those initially reporting treatment success, were still satisfied after 6 months. To note, in the period between those 2 measurements, participants were only advised to keep exercising 3 times per week for at least 30 minutes (aerobic exercise) and strength training.
- Further, the results indicated that of those who did not obtain a successful outcome after 6 weeks, almost 60% did at 6 months. This resulted in almost 4/5 of the participants attaining a positive outcome following the strengthening with an aerobic exercise program. Having 2 out of 3 predictor variables positive at baseline gave a probability of treatment success of 87% at 6 months following the strengthening with an aerobic exercise program.
- The pre-test probability of combined aerobic and strengthening treatment success in neck pain was 61.0% in the short term and 77.0% in the long term. The post-test probability for patients with at least 2 of the 3 predictor variables was 84.0% in the short term and 87.0% in the long term, suggesting such patients are likely to benefit from this program.
It is unclear whether every type of aerobic exercise added to strengthening would give these outcomes. In this particular study, the only aerobic exercise included cycling (supervised). In the home exercise program, participants could choose between cycling or walking. Ninety percent of them were prescribed to walk in the home exercise program. Adherence was not mentioned, and this implies that, due to the lack of a true control group and in the absence of information on adherence, we cannot state what caused the positive evolution in this population. It could have been natural history, the attention someone received, the fact that the combination of aerobic and strengthening led to longer physiotherapy sessions and thus better outcomes, etc. The addition of the aerobic program itself could have improved someone’s general fitness, which may be responsible for better pain relief,… You see, many questions remain, but that is why we love science!
The results of this study form an essential first step in the direction of more targeted care. Precision medicine rather than a one-approach-fits-all. To be continued…
Talk nerdy to me
- The results indicated a good fit of the model was revealed by the Hosmer-Lemeshow test and gave a moderate relationship, reflected by Nagelkerke’s R2 of 0.40.
- The reason that from the 7 candidate predictor variables, only 3 were retained in the model could be because of multicollinearity between the variables. For example, the NDI includes questions about pain, but these are also present when considering the FABQ, and equally, pain scores are reflected on the VAS. As such, these variables are related to one another. The analysis removes variables that are too strongly correlated to avoid reduced power.
- Essential to note is that this study formed the first step in the derivation of a clinical prediction rule. The following steps should be the validation in a different sample to see whether the results are reproducible. Followed by an impact analysis to determine if this prediction model improves patient outcomes and finally implementation in real-life practice.
Take home messages
The current study aimed to identify subgroups of patients who were most likely to benefit from combined aerobic exercise and strengthening for neck pain. As such, it tried to determine who you should prescribe aerobic exercise to obtain treatment success in neck pain, combined with strengthening exercise.
By determining the 1) duration of symptoms, 2) the performance on the neck flexor endurance test, and 3) the absence of referred pain, this study provides you with an easy tool to determine which patients with nonspecific neck pain could benefit from aerobic exercise added to strength training.
Reference
Additional reference
100% FREE HEADACHE HOME EXERCISE PROGRAM
Download this FREE home exercise program for your patients suffering from headaches. Just print it out and hand it to them for them to perform these exercises at home