Research
Head/Neck
May 15, 2026
Identifying Treatment Mechanisms in Neck Pain: Insights from Mediation Analysis of Physiotherapy Approaches

Introduction
Evaluating the clinical effectiveness of a treatment approach requires more than identifying symptom improvement alone; it also involves understanding the mechanisms underlying these changes. As previously outlined in this research review, the mechanisms of manual therapy have been well described. In the context of neck pain, treatment effects may arise through physiological, psychological, or behavioural processes. Treatment mechanisms in neck pain can be further distinguished into specific mechanisms, which are unique to a given intervention, and shared mechanisms, which are common across different treatment approaches. The following mediation analysis aimed to explore how therapeutic exercises and manual therapy may influence clinical outcomes through these proposed mechanisms.
Methods
Study design and settings
This study is a secondary analysis of a previous randomized clinical trial comparing manual therapy vs exercise in people with chronic neck pain. The original trial found no difference in outcomes (pain interference, pain intensity, or physical function) between the two treatments at 4 weeks and 6 months. Participants were adults with self-reported chronic neck pain (≥3/10 for at least 3 months). People with serious conditions or nerve-related neck pain were excluded.
Intervention
Participants received 4 weeks of treatment (5 sessions total), either manual therapy or exercise (strengthening/endurance). Both groups received similar time, support, and home exercises. Treatments were delivered by experienced physiotherapists and could be adapted to the patient.
Effects of interest
This study aimed to investigate 3 different variable relations:
- Direct effect where X or Y variable does not mediate the outcomes.
- The indirect effect is transmitted through the mediator, in other words, X on Y operating through M.
- Total effect, corresponding to the combination of both.
X represents the independent variable and corresponds to baseline pain intensity. Pain intensity was selected because it is considered a primary driver of disability in chronic neck pain.
Y represents the outcomes, namely pain interference and physical function, measured using the PROMIS scales. Pain interference assesses the extent to which pain affects engagement in daily activities, as well as cognitive, emotional, and social participation. The physical function domain evaluates an individual’s ability to perform a range of physical activities.
M corresponds to the mediators that may explain clinical improvement. These mediators included specific physical treatment mechanisms in neck pain, such as tissue mobility, pain modulation, and muscle endurance, as well as shared psychological and relational mechanisms, including self-efficacy, fear, engagement, coping, and therapeutic alliance.
Shared mechanisms were assessed using the Working Alliance Inventory, selected items from the Optimal Screening for Prediction of Referral and Outcome-Yellow Flag (OSPRO-YF), the UW Pain-Related Self-Efficacy Scale, and the Clinician-Rated Patient Engagement scale.
Statistical analyses
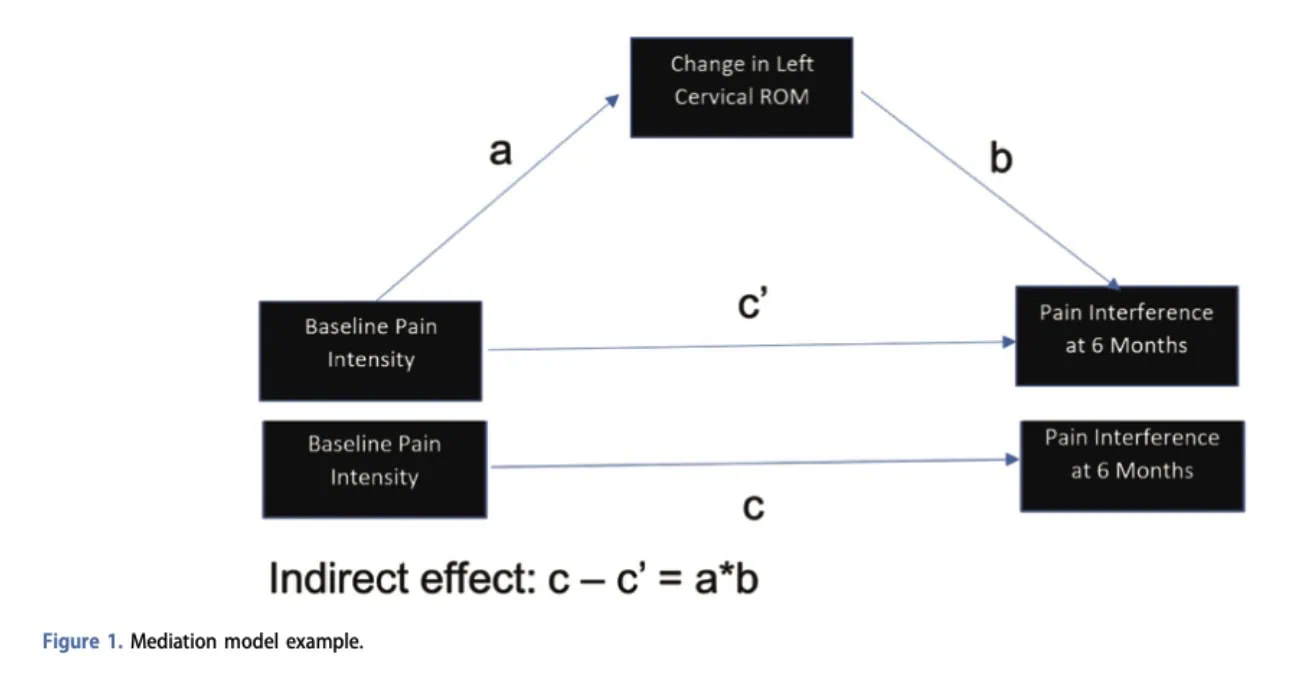
As illustrated in Figure 1, the analysis examined:
- the direct effect of pain intensity on outcomes (path c’),
- the effect of pain intensity on the mediator (path a),
- the effect of the mediator on outcomes (path b),
- and the indirect effect (a × b), representing the portion of the relationship explained through the mediator.
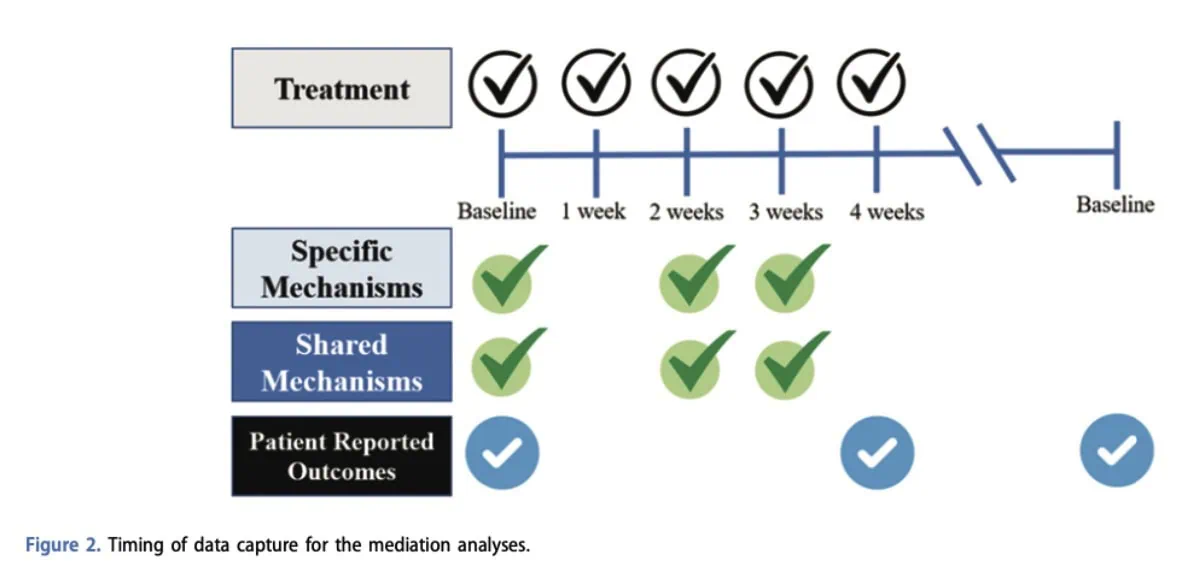
Four categories of mediators were tested separately: mobility, pain modulation, strengthening/endurance, and shared psychological mechanisms. These analyses were performed for both outcomes at short-term (4 weeks) and long-term (6 months) follow-up, resulting in 16 mediation models in total.
The analyses used bootstrapping methods with 5,000 resamples to improve the robustness of the estimates. An indirect effect was considered statistically significant when the confidence interval did not include zero. The treatment group was included as a control variable in all analyses. Overall model fit and explained variance were also calculated using R² values.
Results
Participants had a mean age of 38.3 years and were predominantly female (72.4%). On average, they reported chronic neck pain lasting approximately 76 months, with moderate baseline pain intensity (4.5/10). Participants also presented higher-than-average pain interference and moderate impairment in physical function based on PROMIS scores.
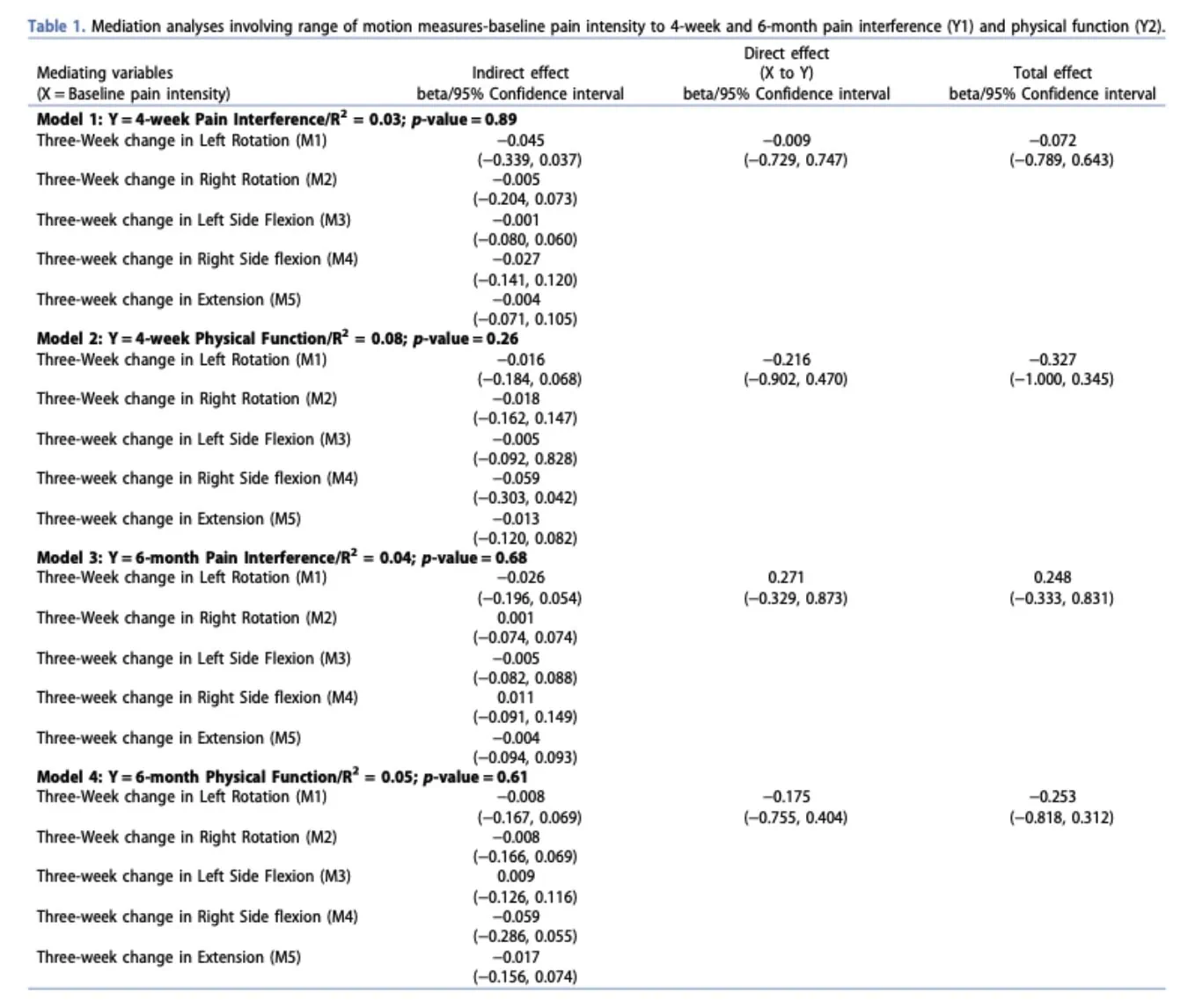
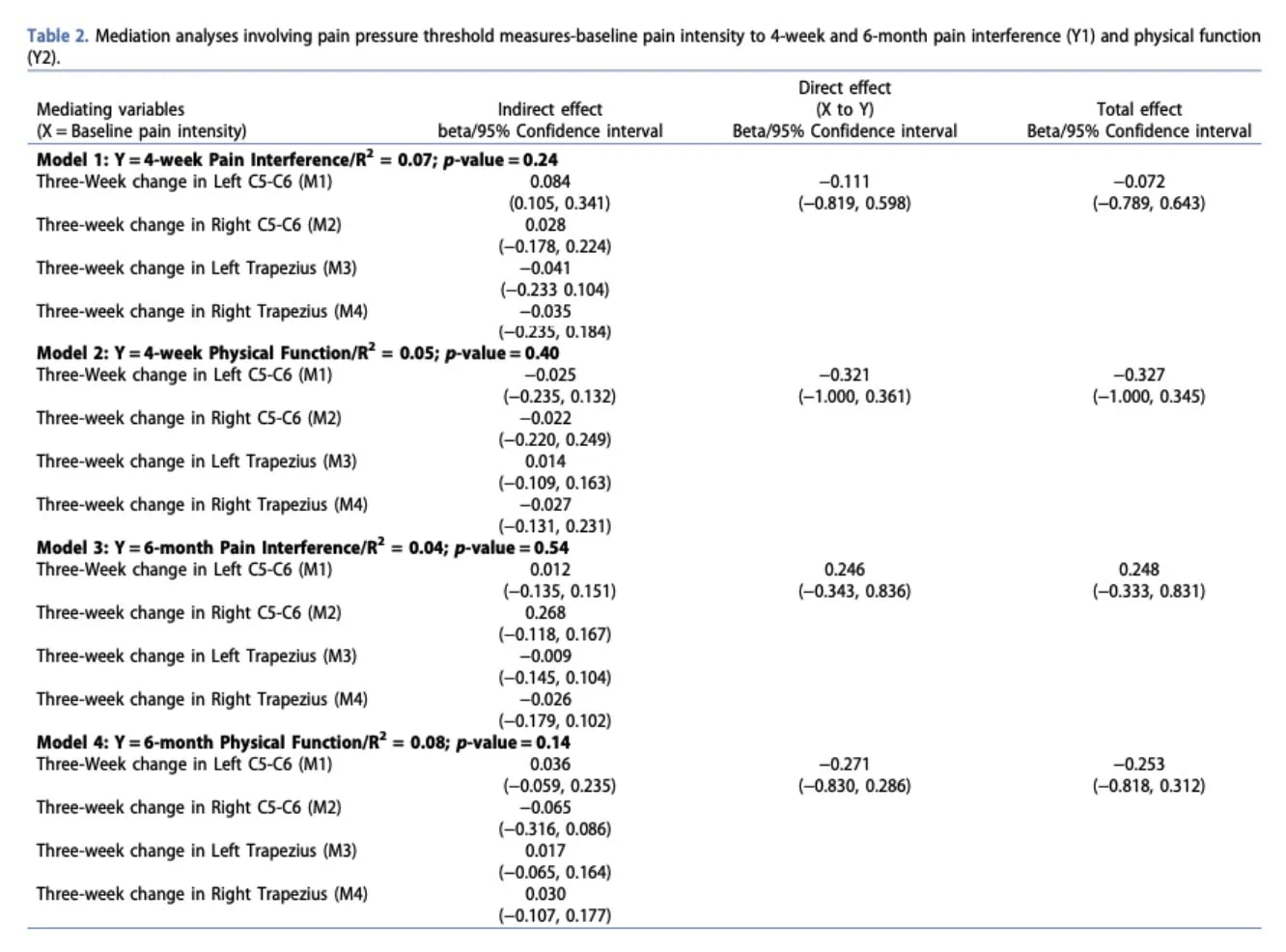
Tissue mobility
Changes in cervical mobility did not significantly mediate clinical outcomes. The R² values ranging from 0.02 to 0.08 indicate that the models accounted for only a small proportion (2%–8%) of the variability in patient outcomes. This suggests that improvements in range of motion alone did not explain the relationship between baseline pain and later function or pain interference.
Pain modulation
Mediation analyses examining pain modulation and strengthening/endurance showed similar results. In both models, the direct effect accounted for most of the total effect, while the proposed mediators were not statistically significant. For pain modulation, R² values ranged from 0.04 to 0.08, indicating that the models explained only a very small proportion of the variability in outcomes.
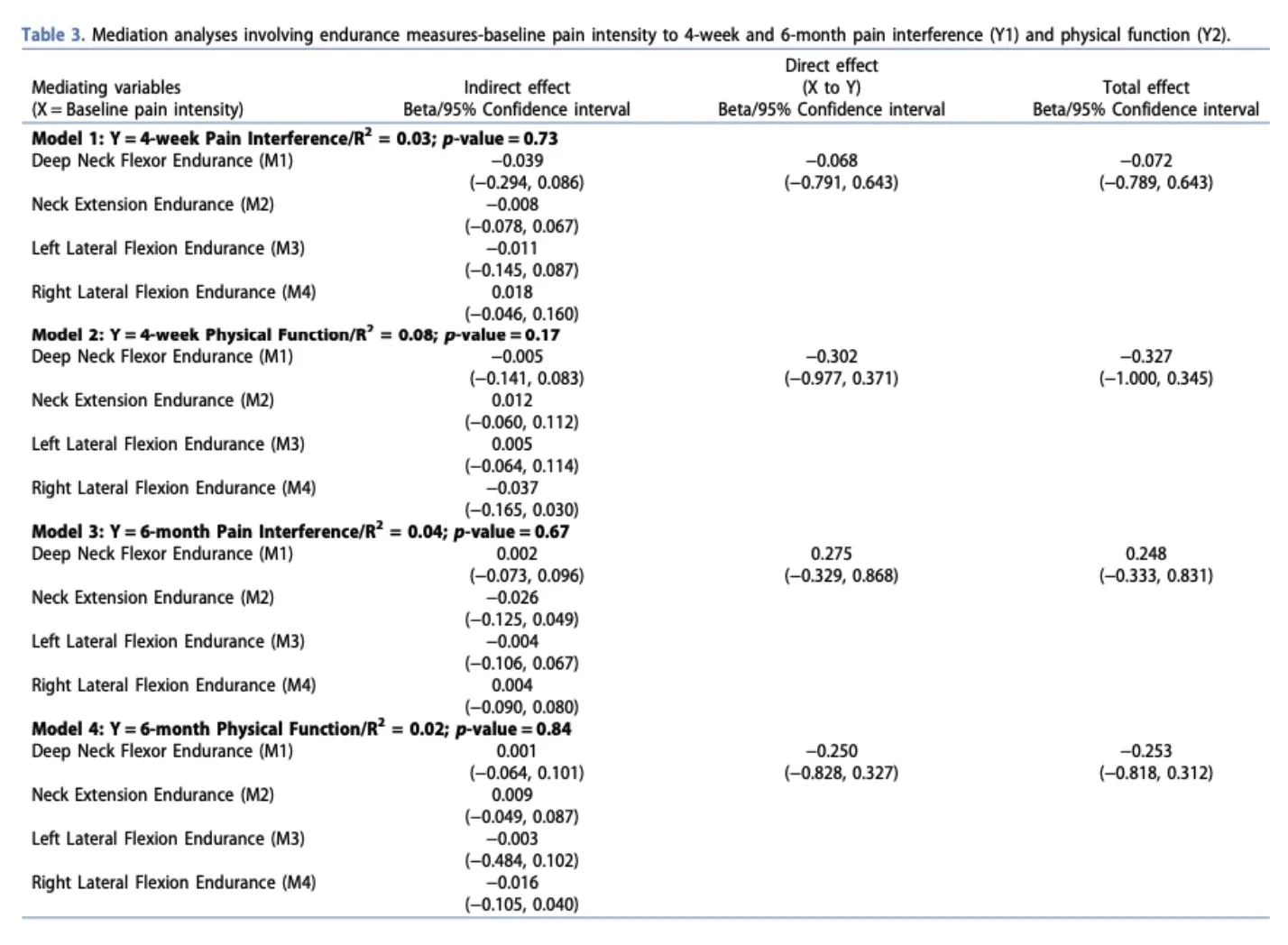
Endurance
For strengthening and endurance, R² values similarly ranged from 0.02 to 0.08, with non-significant p-values, suggesting that these models explained only a small proportion of the variability in outcomes.
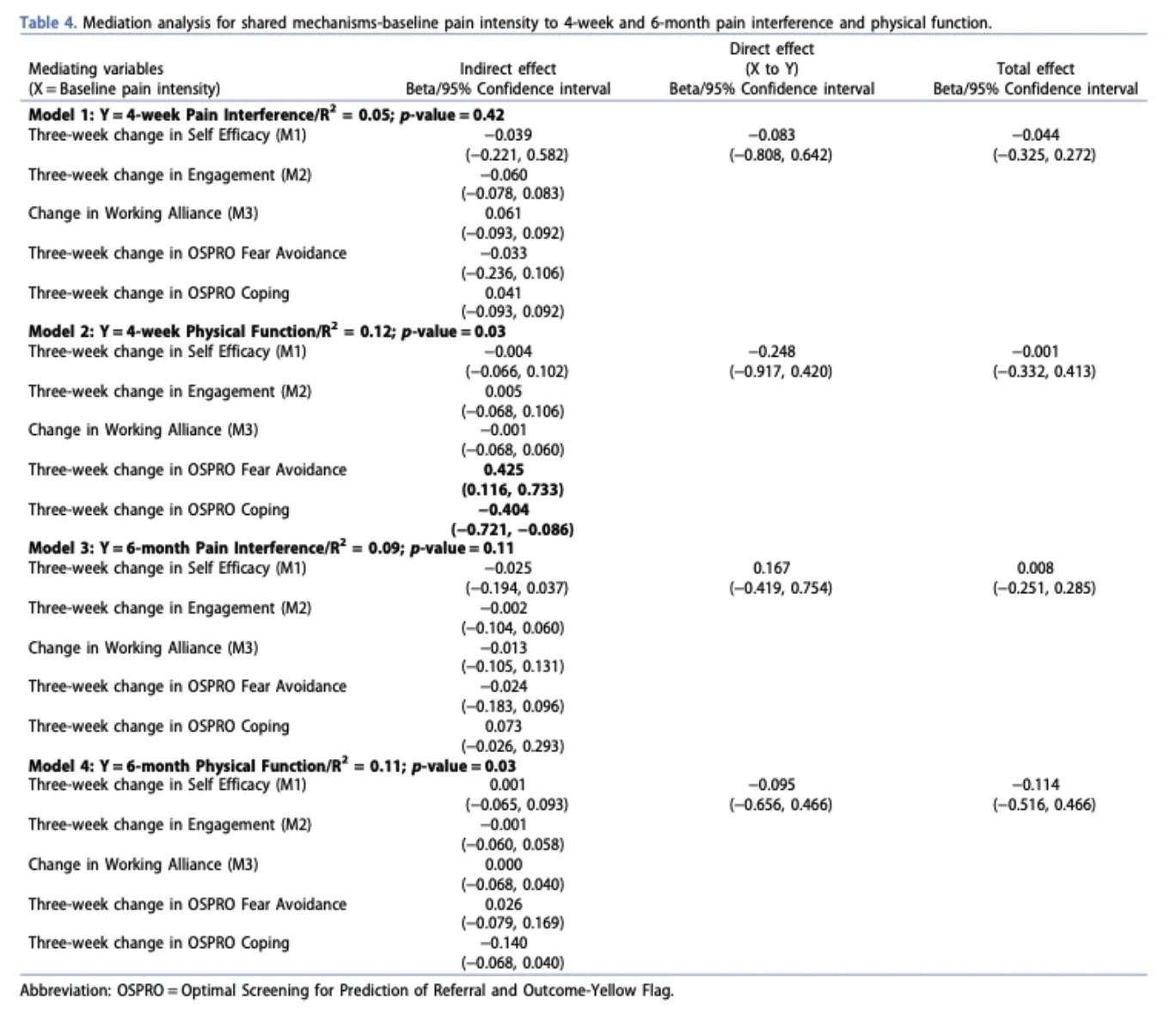
Shared mechanisms
Mediation analyses examining shared psychological mechanisms (self-efficacy, working alliance, engagement, fear avoidance, and coping) showed slightly stronger results than the physical mechanisms models, with R² values ranging from 0.05 to 0.12. Two models reached statistical significance for physical function outcomes at 4 weeks and 6 months. Specifically, reduced fear avoidance and improved coping strategies were associated with better physical function at 4 weeks. However, for pain interference outcomes, improvements were mainly explained by direct effects rather than by the proposed psychological mediators.
Questions and thoughts
The interventions and participant classification used in this study remained relatively generic. Participants were broadly categorized as individuals with self-reported chronic neck pain, without further subgrouping based on clinical presentation, symptom behavior, or potential underlying mechanisms. This broad inclusion strategy may have reduced the ability to identify meaningful treatment mechanisms in neck pain relationships between interventions and outcomes.
This issue may also have been reinforced by the selected outcome measures. Although the PROMIS tools provide robust generic health assessments and facilitate comparisons across conditions, they may lack sensitivity for condition-specific changes in chronic neck pain. Consequently, subtle clinical improvements or mechanistic effects may not have been adequately captured, potentially contributing to the absence of significant mediation findings.
Another possibility is that the mediation model itself failed to capture the true mechanisms underlying clinical improvement. In other words, the statistical framework may not have been sufficiently sensitive to detect the complex and multidimensional interactions involved in chronic pain rehabilitation. The authors therefore advocate for more refined research tools capable of better characterizing pain mechanisms, improving measurement validity, and optimizing the timing of assessments.
Finally, the proposed mediators and their associated proxy measures may not accurately reflect the biological or psychological treatment mechanisms in neck pain recovery. For example, using cervical mobility as a proxy for tissue function may oversimplify the physiological processes involved. Improvements may instead relate to factors such as tissue tolerance, resilience, sensorimotor adaptation, or broader neurophysiological changes. Furthermore, the inability to identify significant specific or shared mediators may suggest that some relevant mechanisms remain insufficiently understood. Emerging evidence regarding novel nociceptive pathways and immune system involvement in chronic pain further highlights the complexity of these processes.
Talk nerdy to me
One major methodological limitation relates to the statistical assumptions underlying mediation analyses. Mediation models require sufficient variability within mediator variables to identify indirect effects. In this study, several mediators demonstrated restricted distributions, with participants exhibiting relatively homogeneous scores for mobility, pain sensitivity, endurance, therapeutic alliance, and engagement. Such restricted variance substantially reduces statistical power and limits the model’s ability to detect mediation pathways.
This issue was further compounded by ceiling effects, particularly for therapeutic alliance and patient engagement measures, where many participants presented with high baseline scores. When scores cluster near the upper limit of a scale, the capacity to observe meaningful improvement or variability becomes limited, attenuating potential indirect effects.
The heterogeneity of the study population likely further diluted mechanistic specificity. Chronic neck pain was operationally defined primarily through symptom duration (>3 months), without finer phenotypic characterization. Such a definition encompasses highly heterogeneous clinical presentations with potentially distinct nociceptive, neuropathic, inflammatory, psychosocial, and sensorimotor mechanisms. Stratified analyses or subgrouping based on symptom profiles, psychosocial characteristics, or mechanistic pain classifications may have improved the sensitivity of the mediation models and strengthened causal interpretation.
Take-home messages
- Improvements in chronic neck pain are unlikely to rely solely on mobility, strength, or pain modulation. Recovery probably involves interacting physical, psychological, and behavioural mechanisms and potentially other unknown mechanisms.
- Manual therapy and exercise produced similar outcomes, suggesting different interventions may act through shared treatment mechanisms in neck pain rather than distinct biomechanical effects.
- Fear avoidance and coping strategies only showed significant associations with physical function at 4 weeks.
- Improvements in tissue mobility, pain modulation, and muscle endurance did not appear to significantly mediate pain-related outcomes in individuals with chronic neck pain.
- Chronic neck pain is highly heterogeneous. Broad classifications based only on symptom duration may overlook important mechanistic subgroups.
- Mechanistic studies should be interpreted cautiously, as current research tools may still inadequately capture the complexity of pain and recovery processes.
Reference
100% Free Headache Home Exercise Program
Download this FREE home exercise program for your patients suffering from headaches. Just print it out and hand it to them for them to perform these exercises at home