
Research
Lumbar/SIJ
May 10, 2026
Soft Bracing Effectiveness in Adolescent Idiopathic Scoliosis Compared Against Rigid Bracing and Wait-and-See

Introduction
Adolescents affected by idiopathic scoliosis are currently prescribed rigid braces. Although effective, these rigid braces come with several downsides, including difficulties with breathing and physical activity. Some adolescents suffer from skin breakdown issues and negative self-image. According to the International Society on Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT) 2016 guidelines, rigid braces have to be worn full-time, defined as at least 20-24 hours per day. But given the limitations of rigid bracing, other types of braces are being studied, such as those made from soft fabric. The idea is that by providing active soft support to the muscles, spinal movements are less restricted, allowing active correction of scoliosis by adjusting the tension in the elastic bands that make up the soft braces. As rigid braces have proven effectiveness in the prevention of scoliosis progression, soft braces should first be compared for their effectiveness. As this information is yet lacking, the current systematic review aims to map available evidence around the benefits and limitations of soft bracing, and compare the soft bracing effectiveness in adolescent idiopathic scoliosis against conventional methods of rigid braces.
Methods
A systematic search of the literature was conducted with the following PICOS.
The absolute goal of bracing, according to SOSORT, is to avoid surgery at all times by preventing scoliosis progression during maturation from adolescence to adulthood. Therefore, the Population of interest were adolescents with idiopathic scoliosis, with a curve magnitude under 40°, age under 18 years, and Risser stage ≤4, indicating the state of ossification of the iliac apophysis, as this is associated with the state of a patient’s spinal skeletal maturity.
The Intervention had to be soft bracing; the Comparator was the rigid brace. Outcomes were success rate, daily wear time, and comfort level.
Success of soft bracing was defined as curve progression of ≤5° at maturity and terminal follow-up Cobb angle <45°. Terminal follow-up meant the last follow-up, at least one year after discontinuing brace treatment. All Study designs were eligible.
The authors used odds ratios (ORs) in their single-arm analysis to statistically pool the soft-bracing outcomes across studies. The OR compares the number of treatment successes with the number of failures, rather than expressing success as a percentage. Because odds are not very intuitive clinically, the authors then converted the pooled OR into a more understandable percentage outcome, which they called the “converted success rate.”
Relative risks (RRs) were used in the double-arm analyses to statistically compare the effectiveness of soft bracing with other treatment approaches, such as rigid bracing or observation. The RR compares how likely treatment success was in one group relative to another group. An RR of 1 means both groups performed equally well, an RR greater than 1 means treatment success was more likely in the soft-brace group, and an RR below 1 means treatment success was less likely in the soft-brace group. Unlike the single-arm analysis, which only describes outcomes within soft-brace patients, the RR analysis allowed the authors to directly evaluate whether soft bracing performed better or worse than alternative treatment strategies.
Results
The meta-analysis included 12 studies and 510 patients. Five were single-arm studies, and seven were double-arm studies. Of the double-arm studies, four compared soft bracing with rigid bracing, and three compared soft bracing with observation.
The authors performed a single-arm meta-analysis and a double-arm meta-analysis. We’ll discuss both more in depth in the Talk nerdy to me section.
Single-arm analysis
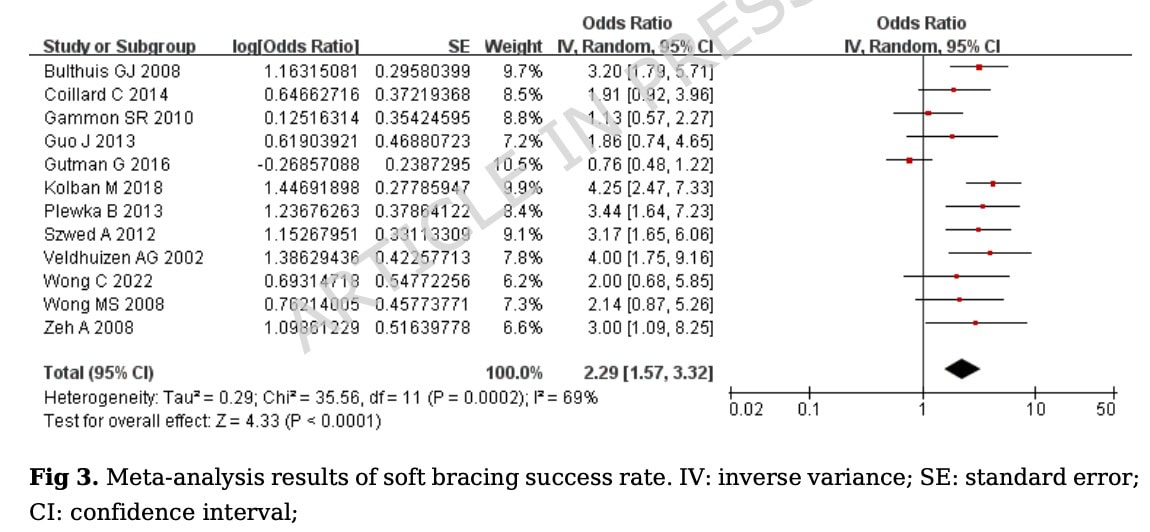
When all studies were pooled together, there was a statistically significant success rate OR= 2.29 (95% CI 1.57 to 3.32; p<0.0001), and a conversion success rate of soft bracing of 70% (OR= 0.70, 95% CI (0.61 to 0.77; p<0.0001).
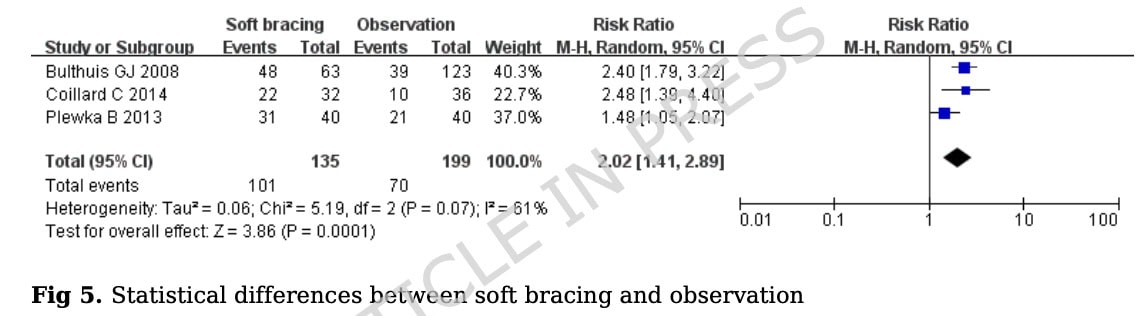
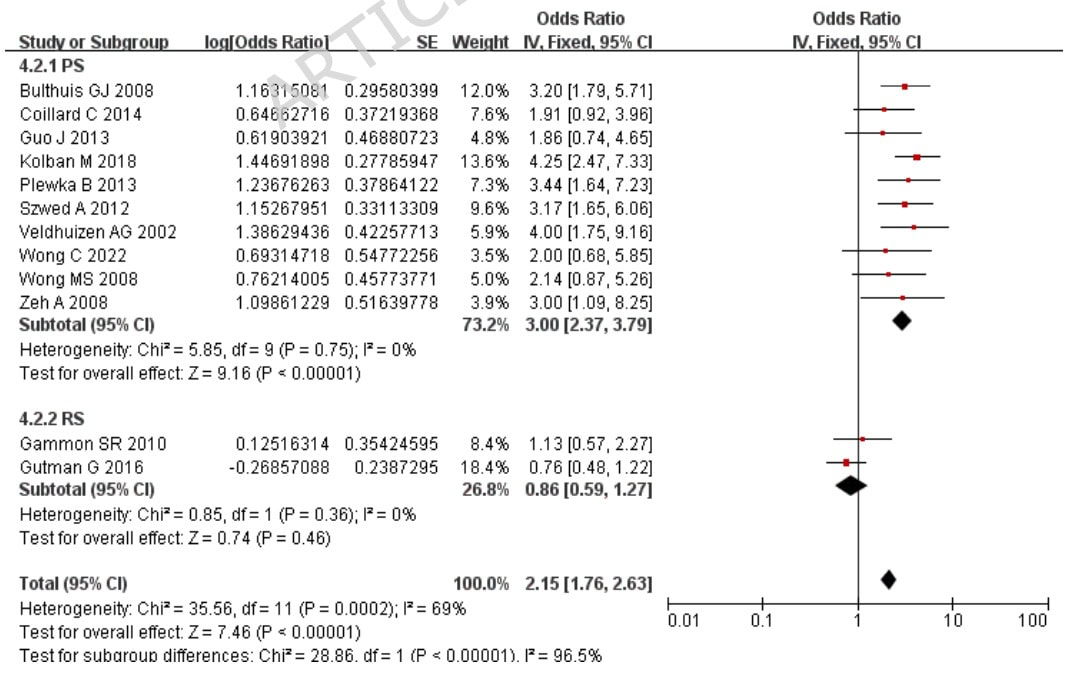
When soft bracing was compared against wait-and-see, the combined RR was 2.02 (95% CI 1.41 to 2.89; p=0.0001), meaning that soft bracing was more effective than wait-and-see. However, there was significant heterogeneity with the I-squared statistic being 69%.
Double-arm meta-analysis
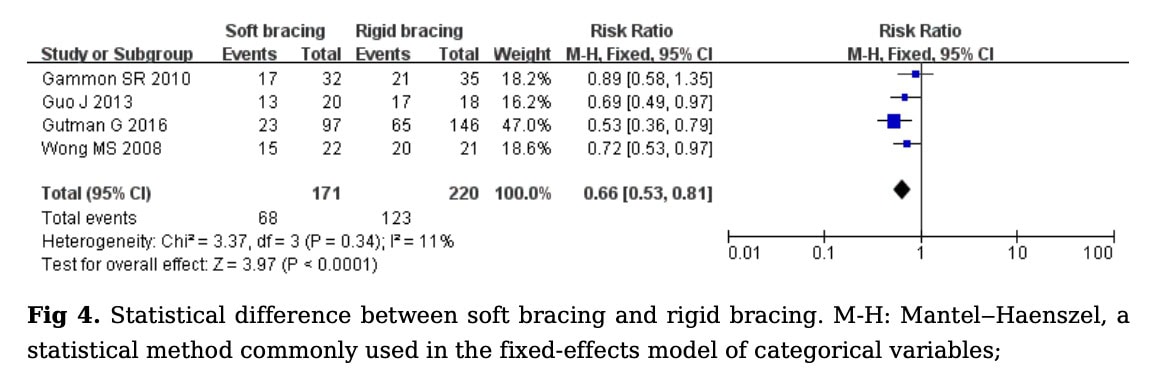
In the seven studies including a control group, 4 studies compared soft braces to rigid braces. When soft bracing studies were compared against rigid braces, the combined RR was 0.66 (95% CI 0.53 to 0.81; p<0.0001), indicating a higher success rate of rigid bracing.
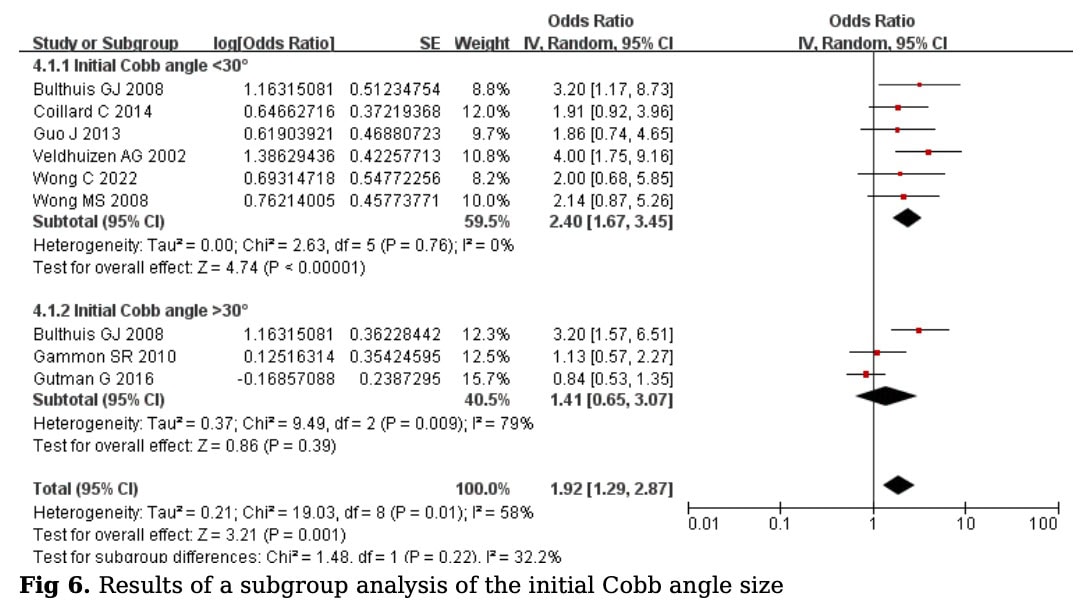
Subgroup analyses were performed to determine whether the initial Cobb angle could be a factor influencing the observed outcomes. When the participants were dichotomized according to their initial Cobb angle below or above 30°, the results revealed that the conversion success rates for Cobb angles < 30° were 71% with OR= 0.71 (95% CI 0.63 to 0.78; P< 0.00001) and for Cobb angles > 30° were 59% with the OR= 0.59 (95% CI 0.39 to 0.75; P=0.39).
Prospective versus retrospective study types as a grouping factor in the subanalyses obtained a conversion success rate of 75% (with OR= 0.75; 95% CI 0.70 to 0.79; P< 0.00001) and 46% (with OR= 0.46; 95% CI 0.37 to 0.56; P=0.46), respectively.
Questions and thoughts
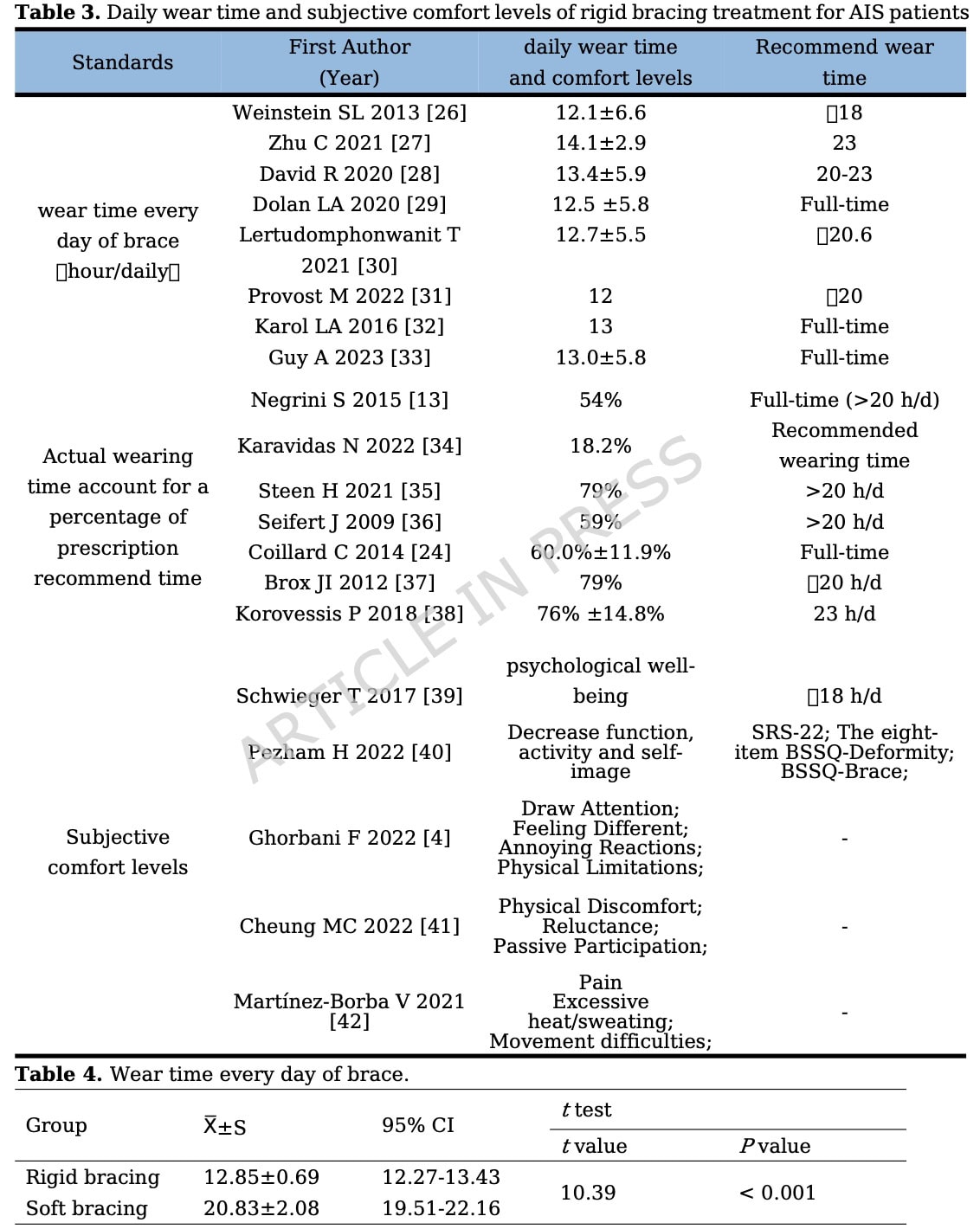
So, is soft bracing effective for adolescent idiopathic scoliosis? It depends on your definition of effectiveness. When you are looking at a hard endpoint outcome, such as curve progression, then rigid braces appear better than soft bracing, but soft bracing is better than wait-and-see (although this comes with high heterogeneity). Looking at comfort while wearing the brace, and daily wear time, soft braces were worn for a mean of 20.83 hours per day versus 12.85 hours for the rigid ones. This difference was statistically significant.
Of course, no one wants the adolescent to progress the scoliosis. The absolute goal of bracing, according to SOSORT, is to avoid surgery at all times. Surgery is typically used when a Cobb angle of 45-50° is observed, and others consider bracing inappropriate for those with curves of >40°, so this population of adolescents seems well chosen to answer a relevant clinical question. Can we avoid progression to greater Cobb angles – and thus surgery – in adolescents with a curve < 40°? Success rates indicated no more progression than 5° and no more than 45° of Cobb angle at the last follow-up. With these criteria in mind, it appeared that rigid braces were more effective than soft braces, and soft braces were more effective compared to doing nothing. But more importantly, those with Cobb angles below 30° had higher success rates with soft braces than those with more severe curve deformities at baseline. So it can be possible that adolescents with scoliosis below 30° can be successfully managed with soft bracing.
On the other hand, we also see that soft braces were worn significantly longer per day than rigid braces. A relevant question to be further investigated raises my mind: could rigid bracing be supported by the wear of soft braces? When we prescribe rigid braces for 20-24 hours per day, but these are only worn for 12h, while the soft braces are worn for nearly 21h, the effectiveness of rigid braces could be potentially maximized even further. That is something that would need to be evaluated in other studies.
Why was the initial Cobb angle of 30° chosen to dichotomize groups in the subgroup analyses? The authors likely selected 30° as the cutoff because it represents a clinically meaningful threshold in adolescent idiopathic scoliosis management and because previous literature has suggested that soft bracing may be most effective for curves below this range. Curves above 30° generally carry a greater risk of progression and may require stronger corrective forces, which rigid braces are better able to provide. Their subgroup analysis supported this rationale, as patients with Cobb angles below 30° showed a higher success rate and lower heterogeneity than patients with larger curves. However, the paper did not strongly justify the choice of 30° statistically, so the cutoff appears to have been based mainly on clinical reasoning and previous literature rather than a predefined data-driven threshold. Subgroup analyses based on post hoc or loosely justified thresholds should always be interpreted cautiously because different cutoffs (for example, 25° or 35°) might have produced different subgroup findings.
Talk nerdy to me
It’s a meta-analysis, so in theory, the gold standard. While that is true, we’ll have to be honest that not every conclusion of a meta-analysis is considered the top tier of the evidence base. In this particular case, the fact that the authors performed a single-arm meta-analysis is doubtful.
With a single-arm meta-analysis, they are putting all studies together, regardless of whether or not a control group (from a randomized controlled trial or a longitudinal case-control study) was included. Some single-arm studies, for example, an observational cohort study, do not include control groups or control participants. While these studies can give an indication of whether or not soft bracing can have positive effects in the course of the follow-up measurements, these effects are not compared against a control group. We can derive some information from these designs, but no hard evidence.
The authors’ decision to perform a single-arm meta-analysis is questionable, primarily due to the methodological execution. The authors included 12 studies in total – 7 double-arm and 5 single-arm designs – yet they proceeded to pool the data from the 7 double-arm trials into a single-arm meta-analysis. This feels a bit unnatural. By pooling every study that examined soft bracing – not just those strictly designed as single-arm observational cohorts, but also those incorporating a control group (such as observation or rigid bracing), they effectively extracted data from the intervention arms while discarding the corresponding control groups. Discarding the control groups from higher-quality double-arm studies to bolster the single-arm data makes the process feel less like objective synthesis and more like statistical framing.
Although this can estimate an overall soft-brace success proportion, it also strips the controlled studies of their comparator context. Therefore, the reported 70% success rate derived from the single-arm meta-analysis should be interpreted as a way to generate explorative information, while the comparative findings from the double-arm meta-analyses, where soft bracing outperformed the wait-and-see but underperformed rigid bracing, should carry more clinical weight.
Sensitivity analysis revealed that the study results were robust. Possible publication bias was examined and showed it absent.
Take-home messages
The reason this review was needed is clinically straightforward: rigid bracing works, but it is not easy to live with. The article highlights that rigid braces may reduce muscle endurance and pulmonary function, limit physical activity, and contribute to skin breakdown. Full-time brace wear is often prescribed at 20–23 hours per day, but comfort and adherence become major barriers. Soft braces were developed to address this problem: they are made of softer fabric, allow some spinal movement, and use elastic tension rather than a rigid shell to apply corrective forces.
The evidence mainly applies to skeletally immature adolescents with adolescent idiopathic scoliosis, with curves below 40°, and the strongest subgroup signal favoured patients with Cobb angles below 30°. Regardless of the observed effects, rigid bracing was still superior to soft bracing, while wear time and comfort were significantly better with soft bracing compared to rigid bracing. Although rigid bracing comes with downsides, it is still the best option for preventing curve progression. Future research should look into the differences in outcomes when wear time is included as a variable. But other strategies can also be studied, for example, other research has looked into the effectiveness of night-time bracing, finding similar effects compared to full-time rigid bracing. Putting all these together in future research would be beneficial to support clinical decision making for these adolescents.
Reference
MASSIVELY IMPROVE YOUR KNOWLEDGE ABOUT LOW BACK PAIN FOR FREE
5 absolutely crucial lessons you won’t learn at university that will improve your care for patients with low back pain immediately without paying a single cent
