Research
Diagnosis & Imaging
April 9, 2026
Screening for Tumors in Neck Pain: Most Commonly Reported Red Flags Derived from Individual Case Reports

Introduction
Neck pain is extremely common, and while most cases are classified as non-specific and benign, a small but clinically critical proportion may represent serious pathology. While the Canadian C-spine rules can be reliably used for examining the possibility of fractures to the neck, we know much less about red flags for tumors in the cervical spine. The challenge for physiotherapists, who often serve as first-contact practitioners, lies in distinguishing benign musculoskeletal pain from these rare but potentially life-threatening conditions.
Although clinical guidelines frequently promote the use of the identification of red flags to identify serious pathology, the evidence underpinning these red flags is weak, inconsistent, and often based on expert opinion rather than robust data. Therefore, this scoping review was necessary to map existing evidence and to identify commonly reported red flags to help us increase the evidence certainty.
Methods
This study was a scoping review conducted using the Joanna Briggs Institute (JBI) methodology and reported according to PRISMA Scoping Review guidelines. Any study design was eligible for inclusion when it reported on patients presenting to a primary care clinician with a primary complaint of neck pain, which was ultimately diagnosed as a tumor. The tumor diagnosis could encompass both malignant (primary or metastatic) and benign ones. The literature was searched until 2025.
Results
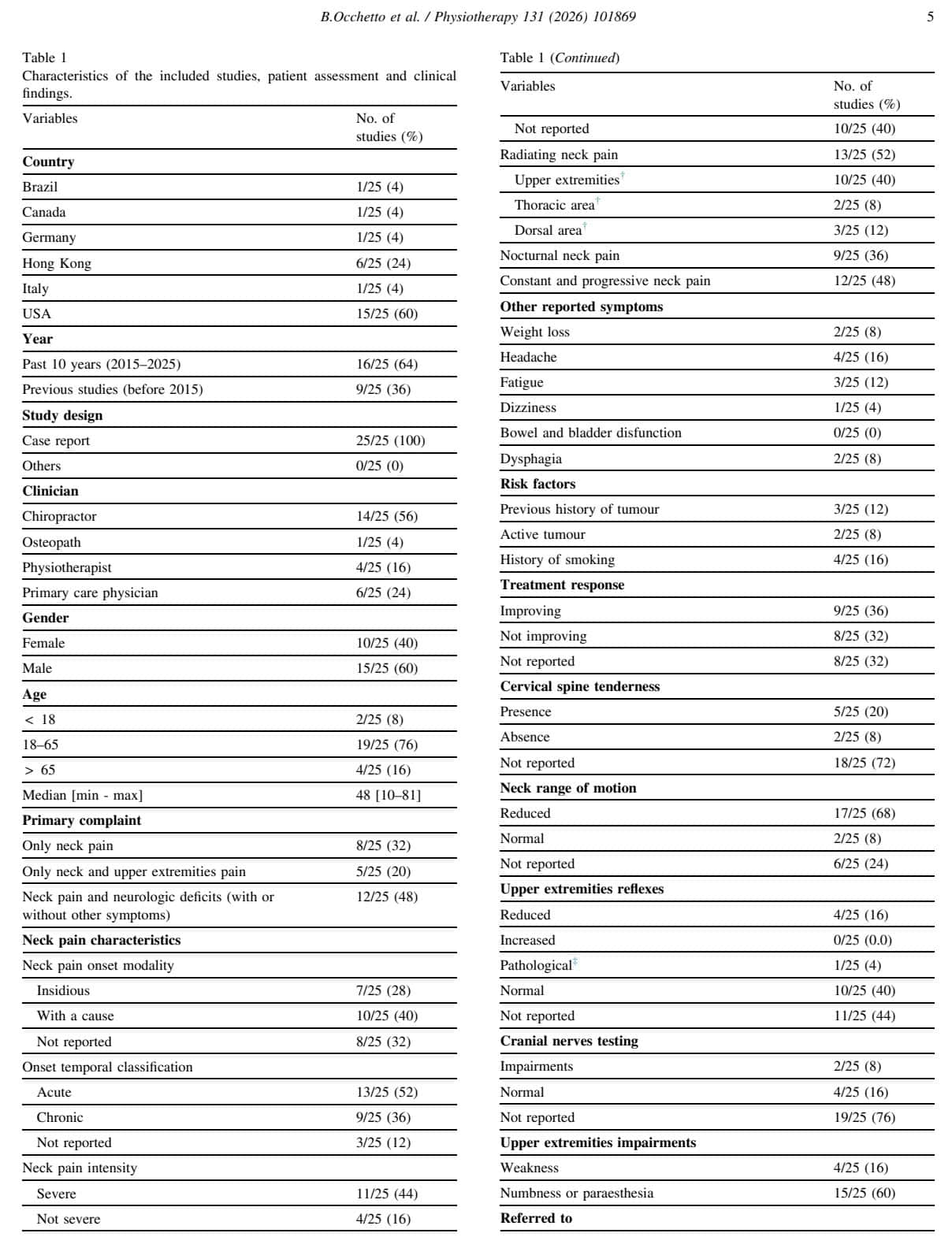
From 10,211 records, 25 studies were included, all of which were case reports. These 25 case reports were about 25 unique individuals who presented to a chiropractor, primary care physician, physiotherapist, or osteopath with a primary complaint of neck pain. The median age of these individuals was 48 years, but ranged from 10 years to 81 years of age. Ten cases were females (40%), and the rest were males (60%).
In eight patients, the complaint was isolated to the neck region, five experienced neck and upper extremity pain, and 12 patients had neck pain and associated neurological symptoms, with or without pain in the upper extremities.
Patient history findings
The subjective history taking revealed that in 10 people, the neck pain started with a specific event, being a traumatic event, or a Valsalva manoeuvre, or physical exertion, and seven people experienced an insidious onset of their symptoms.
52% experienced symptoms for less than three months, 36% reported having chronic neck pain with symptoms being persistent for more than three months, and in the other cases, pain was not described in detail. 73% reported the pain as being severe on the NRS, VAS, with >7/10 scores. The other studies reported moderate-to-mild cervical pain.
Thirteen patients reported radiating pain. 77% of these people experienced radiating pain to the upper limbs, 23% to the upper back, and 15% to the thorax. Fifteen case studies reported sensory alterations with symptoms of numbness or paresthesia in the upper limbs. Four studies mentioned upper limb muscle weakness.
Objective examination
In the objective examination, local tenderness to the cervical spine was reported by 5 subjects. In almost 70%, this was accompanied by reduced neck range of motion.
The most common red flags identified were:
- Severe, progressive, constant neck pain
- Neurological signs and symptoms
- Weakness
- Sensory deficits
- Altered reflexes
- Cranial nerve involvement
- Nocturnal neck pain
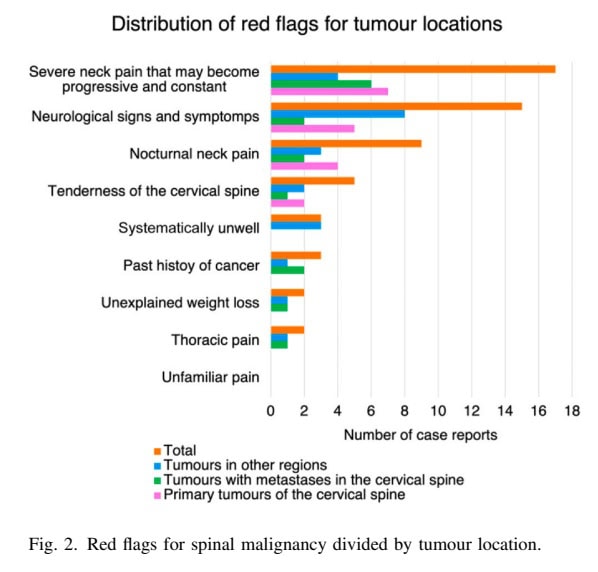
These patients were referred to an outpatient specialist or to the emergency department, and all were diagnosed with a tumor. Nine patients had a primary tumor of the cervical spine, eight had a metastasis in the cervical spine, and eight people had a primary tumor in other parts of the body.
Questions and thoughts
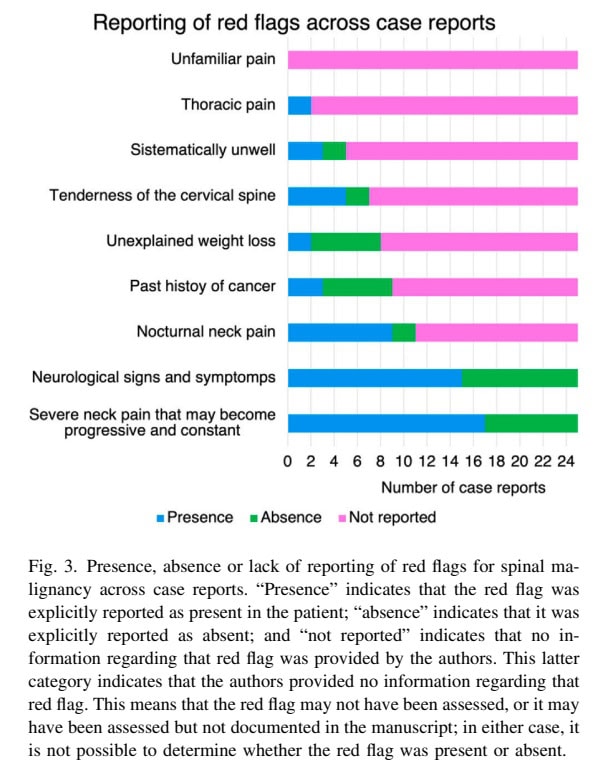
Many classic red flags (e.g., unexplained weight loss, prior cancer) were rarely reported, and some expected red flags were not reported at all. The scoping review identified a high variability in the documentation, as many studies did not report whether red flags were present or absent. We must remain aware that although other red flags were not reported, this doesn’t mean they are useless or invalid.
Rather, it pointed out that much more research is needed to clarify which specific red flags exist in the region of the cervical spine, especially since many red flags are based on expert opinion and derived from other regions of the body, not the neck. However, being aware of the top 3 red flags described here, it is important to note that these findings are rarely present in isolation. So, having one red flag does not immediately raise suspicion of a serious underlying pathology being present. You must be aware that the specific inclusion criterion for studies to be included in this scoping review was that the original complaint of neck pain was ultimately diagnosed as a malignancy. But, you’ll see many more patients with, let’s say, nocturnal neck pain who don’t have an underlying serious pathology. As a consequence, you’ll have to continue screening for red flags, and when signs and symptoms do not fit a certain expected trajectory, then you can raise your suspicion.
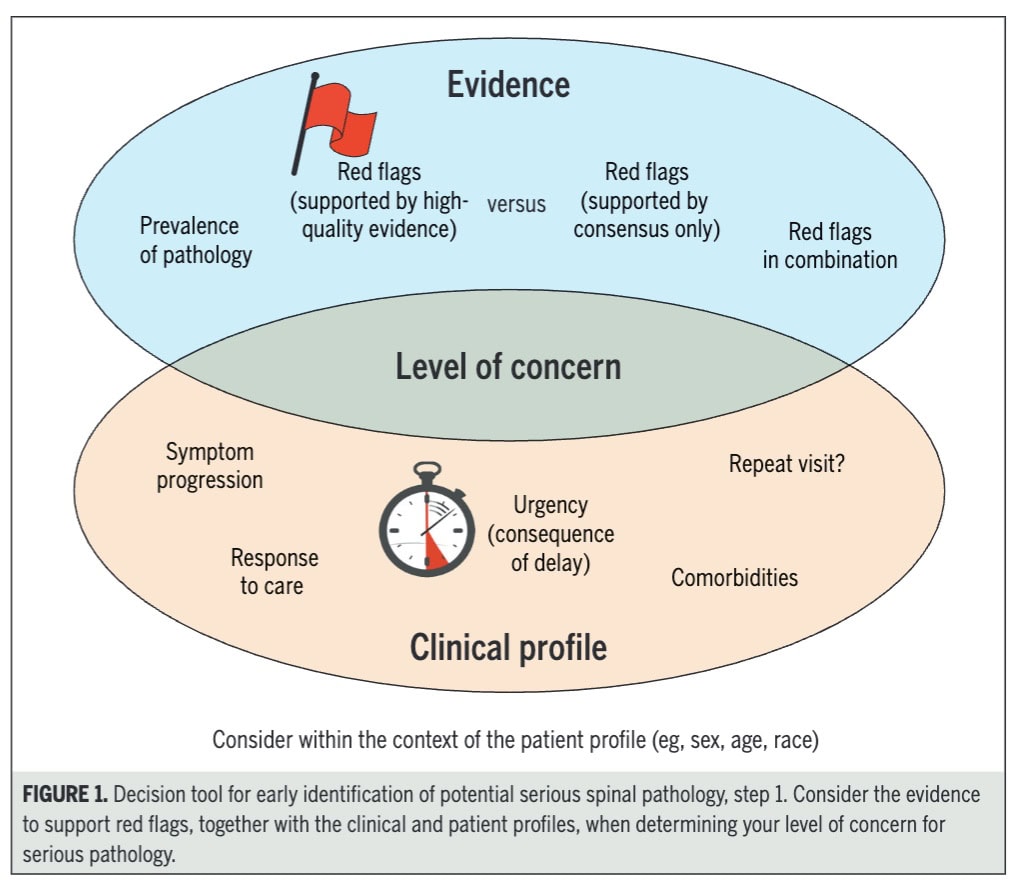
In the International Framework for Red Flags for Potential Serious Spinal Pathologies from the International Federation of Orthopedic and Manipulative Physical Therapists (IFOMPT), which was intentionally developed to help us identify serious underlying pathologies in the spine, developing such an “index of suspicion” was proposed. Although most of the evidence in this Framework was derived from the lumbar spine, we can adopt a similar strategy when assessing patients with complaints in the cervical spine.
Determining whether a patient’s musculoskeletal complaint has a specific (serious) underlying cause is less about identifying a single decisive sign and more about building and continuously updating an index of suspicion. The framework emphasizes that red flags are not diagnostic on their own, but instead, they function as clinical cues that must be interpreted in context and, importantly, in combination.
They outline the following steps:
The first step in this filtering process is to consider the patient’s baseline profile, including age, sex, comorbidities, and social or environmental risk factors. These elements shape the pre-test probability of serious pathology. For example, older age increases the likelihood of fracture or malignancy, while factors such as immunosuppression or intravenous drug use raise suspicion for infection. This contextual layer is essential, as the same symptom may carry very different implications depending on the individual.
Next, clinicians evaluate red flags, but always as clusters rather than isolated findings. Certain patterns are more concerning than others. Progressive neurological deficits raise suspicion for conditions like cauda equina syndrome. Non-mechanical pain behavior, such as constant, worsening, or unfamiliar pain that does not respond as expected to treatment, is another important signal. Systemic features like unexplained weight loss, fever, or fatigue may indicate malignancy or infection, while minor trauma in a patient with known osteoporosis can point toward fracture. A history of cancer, particularly when combined with new or changing pain and night symptoms, further elevates concern.
A crucial element in this framework is the evolution of symptoms over time. Improvement or stability generally supports a benign musculoskeletal presentation, whereas worsening symptoms, unexpected progression, or failure to respond to appropriate care should prompt reconsideration of the diagnosis. In practice, this temporal behavior is often one of the strongest indicators that something more serious may be occurring.
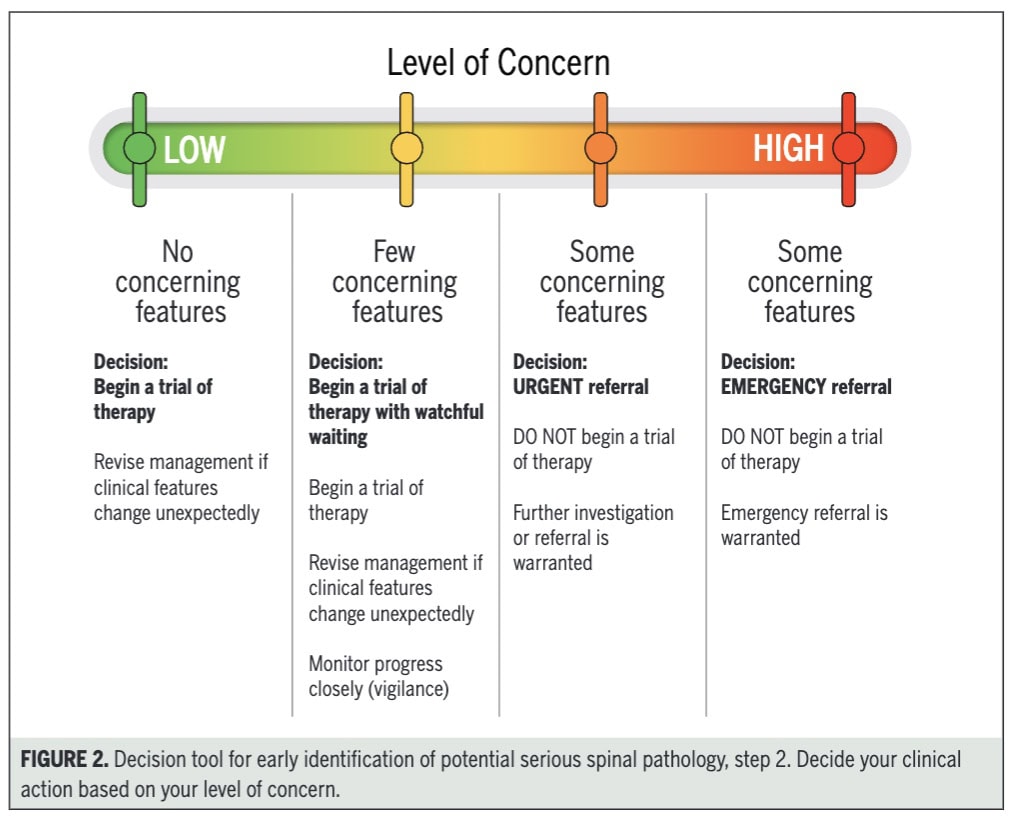
Based on the integration of patient profile, red flag clusters, and symptom progression, clinicians then categorize their level of concern. When concern is low, a trial of conservative therapy is appropriate. With moderate concern, clinicians may proceed with treatment but should apply close monitoring and clear safety netting. When multiple or progressive red flags are present, urgent referral for further investigation is warranted, and in cases of high suspicion (e.g., significant neurological compromise), immediate emergency referral is required. This stepwise decision-making process ensures that care is both safe and proportionate to risk.
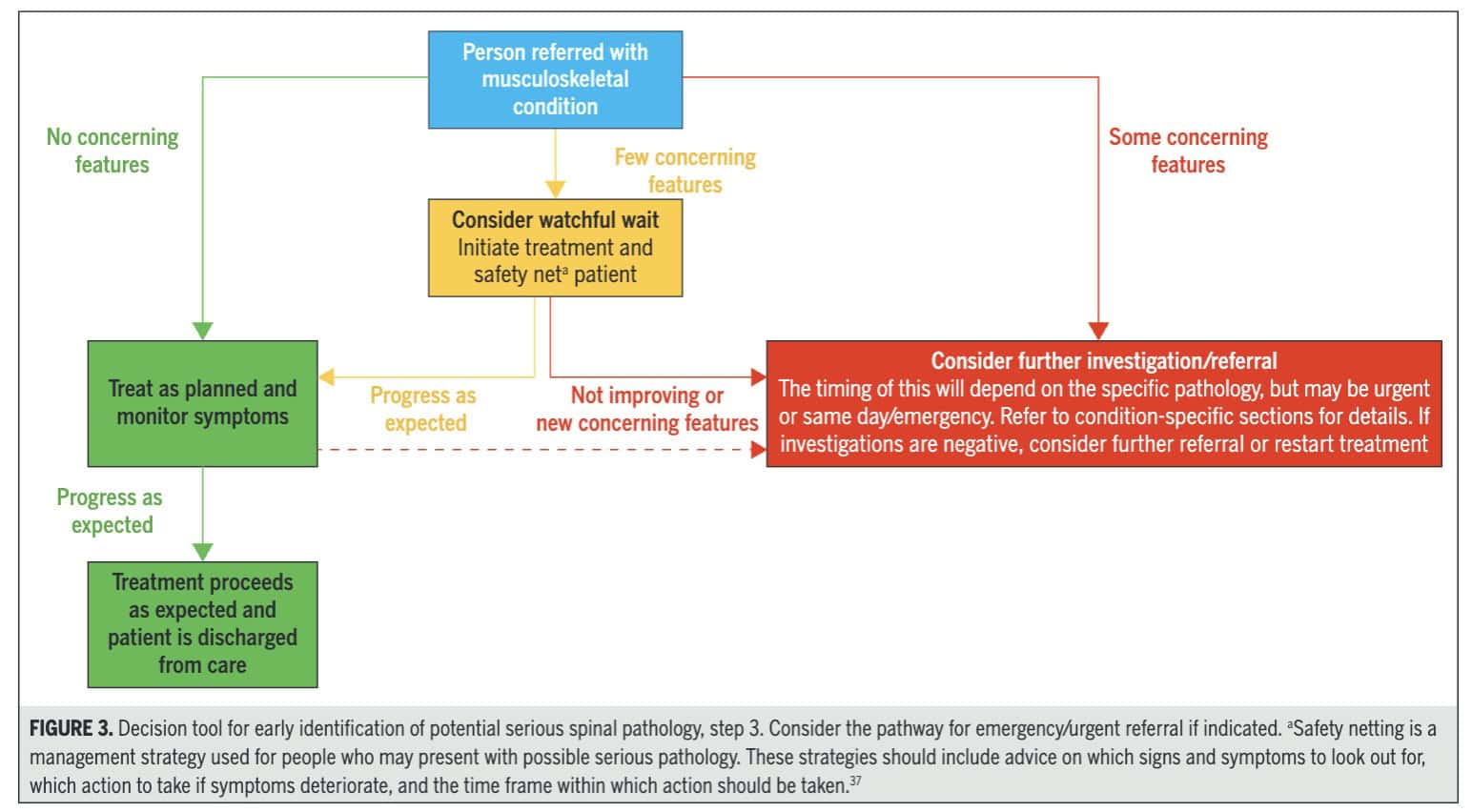
Finally, the framework highlights the importance of safety netting. Even when serious pathology is not initially suspected, patients should be informed about warning signs, what actions to take if symptoms worsen, and the expected timeframe for improvement. This acknowledges that serious conditions may evolve and ensures timely reassessment if the clinical picture changes.
Talk nerdy to me
The evidence derived from this scoping review has to be seen as of low quality since the included studies were all case reports. However, in the absence of better quality research, we can still use these red flags as proposed here, if remembering that there may be more than the ones outlined here. A gap in the literature was identified by the absence of specific information regarding the red flags in the neck region, and the authors concluded that many of the red flags proposed for neck malignancies were derived from the low back region. That’s why it is important to consider this evidence as preliminary and as a door-opener for further research.
Due to the inclusion of only case studies, it was impossible to conduct a meta-analysis, and important information may be lacking. As can be seen in Figure 3, a lot of papers didn’t mention the absence of a certain red flag being reported, not meaning that the red flag was absent. It could have been forgotten to report or document these findings, for example. These are all factors in which case study designs limit the certainty of evidence.
Take-home messages
Evidence for neck pain red flags relies heavily on case reports rather than robust diagnostic trials. Performing a thorough history-taking remains the cornerstone of the clinical encounter. When screening someone, and in light of more robust evidence surrounding the specific red flags for the neck, focusing on pain progression and neurological deficits, rather than waiting for more severe signs like weight loss are of utmost importance.
Because the evidence is based solely on case reports, we cannot determine the true prevalence of these red flags or their ability to actually “rule in” a tumour, risking both over-referral and missed diagnoses. Therefore, I recommend using the International Framework for Red Flags for Potential Serious Spinal Pathologies from the International Federation of Orthopedic and Manipulative Physical Therapists (IFOMPT). As it was developed to help us identify serious underlying pathologies in the whole spine, determining an “index of suspicion” based on known risk factors, red flags, and evolution of symptoms over time seems the best strategy so far to construct a level of concern and direct your care pathway accordingly.
Reference
21 OF THE MOST USEFUL ORTHOPAEDIC TESTS IN CLINICAL PRACTICE
We have comprised a 100% Free E-Book containing 21 of the hands-down most useful orthopedic tests per body region guaranteed to help you reach a proper diagnosis today!