
Research
Exercise
January 9, 2023
Progressive strengthening for persistent ACLR hamstring deficits

Introduction
The hamstring muscles are important to target in ACL rehab as the forces of the hamstring oppose forward translation of the tibia relative to the femur. Hence they help the ACL in preventing excessive forward translation of the tibia. ACL injuries account for a large number of knee injuries in active individuals and require a long rehabilitation period. In some, ACL reconstruction is performed with an autograft of the hamstring tendon. This requires additional attention to recover the strength of the hamstring muscle group. Studies point to an increased ACL retear risk in those who have had a prior ACL injury. Those with persistent strength deficits and limb symmetry imbalances, as can be seen in many patients even after “completing” months of rehabilitation, are at even greater risk. This study wanted to find out whether people having persistent hamstring strength deficits may benefit from a progressive strengthening approach in the late stages of rehab. Therefore, progressive strengthening for persistent ACLR hamstring deficits at 12-24 months was compared to low-intensity home exercises.
Methods
A superiority randomized controlled trial was conducted in Denmark. Participants were recruited 12-24 months after ACL reconstruction. They had to have persistent maximal hamstring strength asymmetry, objectified with a >10% leg-to-leg difference in isometric knee flexion measured with the knee at 90°.
They were randomly assigned to a supervised progressive strength training group that also included neuromuscular exercises or to a control home-based low-intensity weight-bearing exercise program.
In the progressive strengthening group, participants completed 60-70 minutes of supervised sessions two times per week for 12 weeks. This program consisted of 8 exercises which were performed in 3 sets of 10 repetitions at an intensity of 12 repetitions max. The exercises that were performed included leg presses, lying leg curls, squats with a barbell behind the head, Nordic hamstring exercise.

The neuromuscular progressions were made from lunges to lunges with weights in the hands, to lunges with thoracic rotations. A lateral jump progressed from jumping over a barbell on both legs to jumping over the barbell on 1 leg. Trunk stability progressed from a Superman exercise supported on the knees and forearms and lifting one leg and the opposite arm to the same exercise performed from a planking position. Bridges were performed bilaterally first and progressed from single-leg bridges to bridges on a gym ball with a hamstring curl.
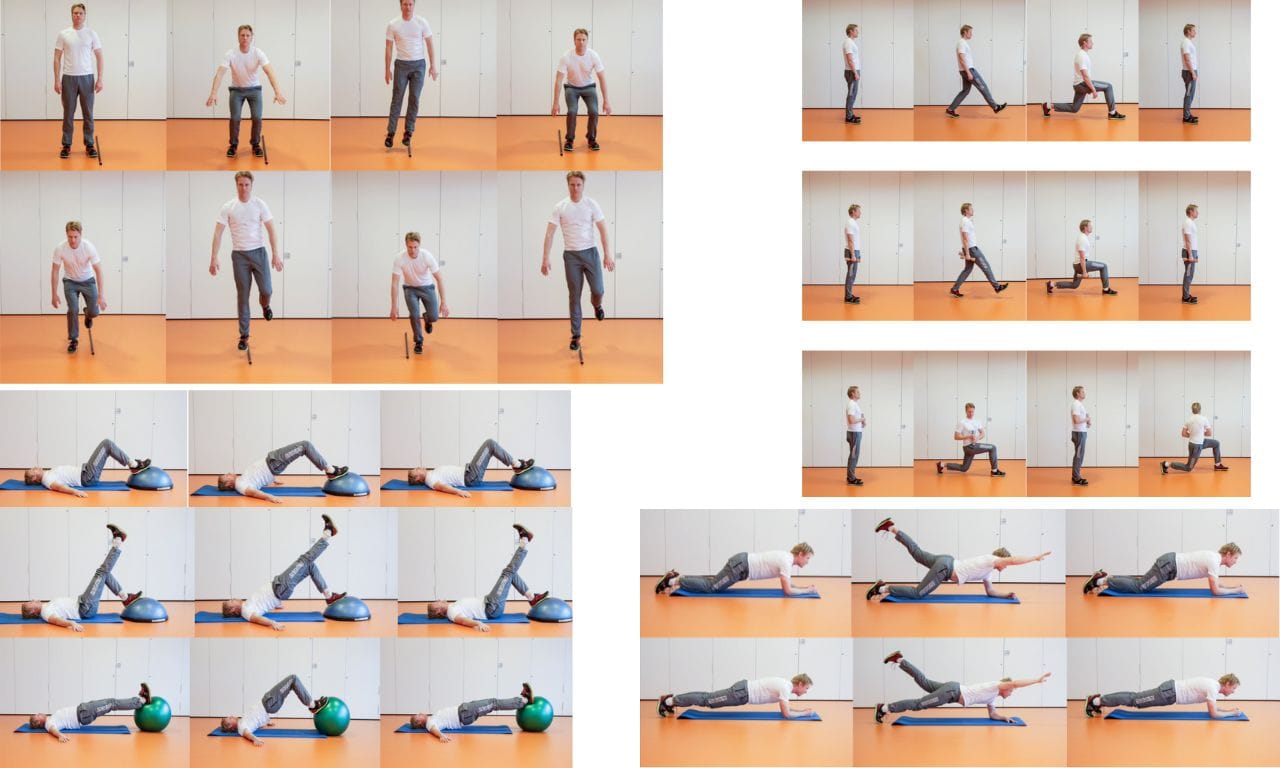
The control group received verbal and written instructions on how to perform 4 home weight-bearing low-intensity exercises, twice a week. These exercises included gluteal presses, squats, standing leg curls and stationary lunges, all performed with the resistance of an elastic band.

After 12 weeks, the between-group change in maximal unilateral isometric hamstring strength of the knee was the primary outcome. This was measured using a dynamometer in a 90° flexion of the knee and expressed in torque.
Results
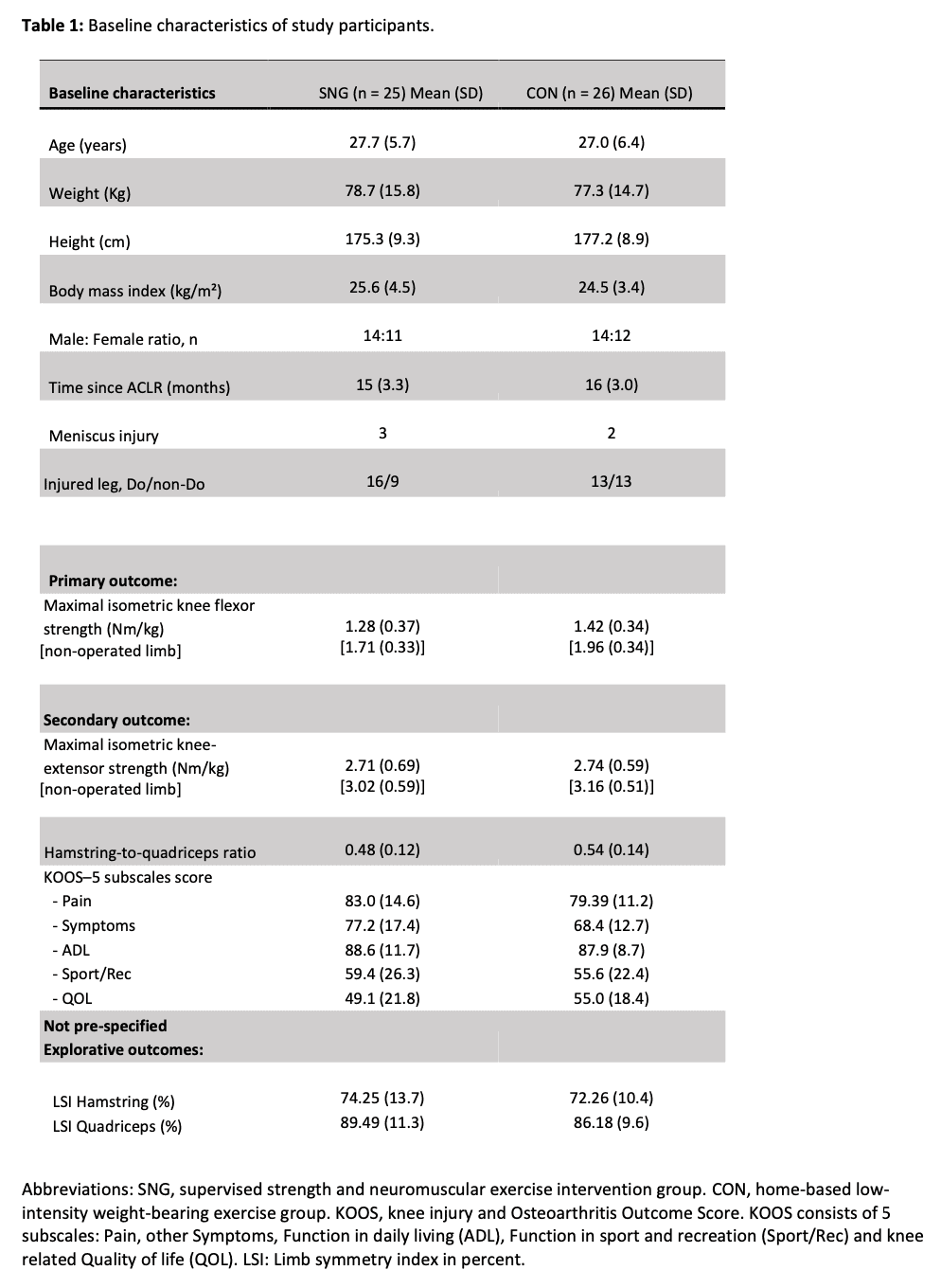
A sample of 51 participants was randomized in this study to the progressive hamstring strengthening intervention or control group. The baseline characteristics show both groups were comparable.
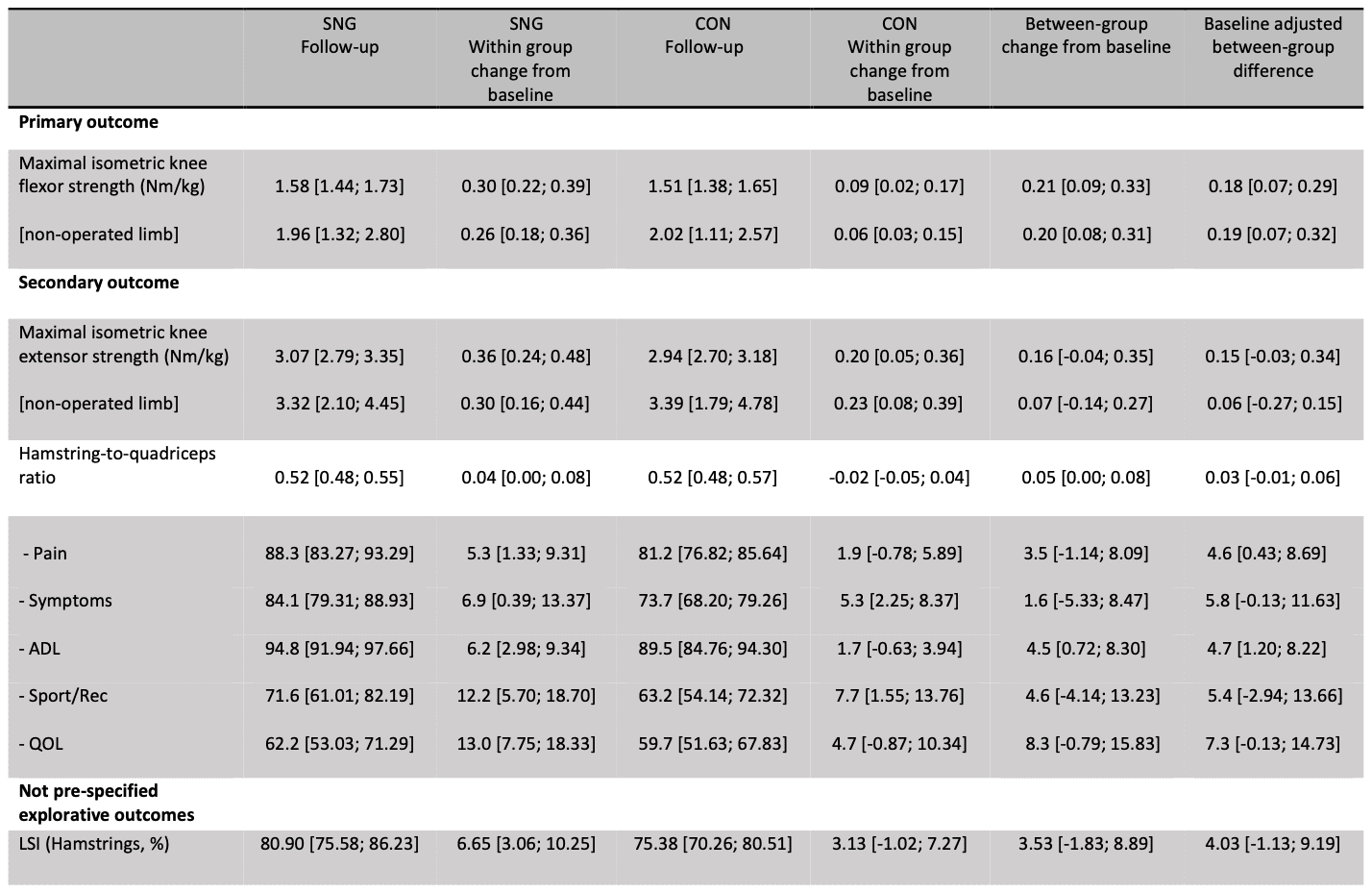
Progressive strengthening for persistent ACLR hamstring deficits resulted in greater improvement in isometric hamstring strength in the intervention group compared with the control group. The difference was 0.18 Nm/kg and had a large effect size of 0.30. Both groups showed within-group improvements: 0.30 Nm/kg in the intervention group and 0.09 Nm/kg in the control group.
Questions and thoughts
Secondary outcomes included the change in quadriceps strength and hamstring-to-quadriceps (H:Q) ratio. A patient-reported outcome was included as well and was the Knee Injury and Osteoarthritis Outcome Score (KOOS). As an exploratory variable, the limb symmetry index (LSI) was calculated.
The primary outcome was statistically significant, meaning that the maximal isometric strength of the hamstrings improved more in the progressive strengthening group than it did in the control group. The secondary outcomes show a similar trend to the primary outcome in quadriceps strength, but not in the H:Q ratio. The strength of the quadriceps improved almost equal to the improvements seen in the hamstrings. Hence, it is logical that the hamstring: quadriceps ratio did not improve. The LSI showed improvements over the 12-week duration of the study in both groups. However, at the trial completion, an asymmetry in the injured and non-injured leg was still evident and still not fully recovered. Of course, it is good that the non-injured leg gained strength as well. But this means that the differences in symmetry had not improved to a large extent. Maybe the exercises were performed too much with bilateral loading? However, this remains unknown as the paper did not report details about the progressions that had been made by the individuals on average. Therefore, unfortunately, we cannot know to what extent the exercises were performed bilaterally or unilaterally. The exercises, however, were likely to be feasible in both groups as little drop-out (2 and 3 in the intervention and control) and high adherence rates were documented at 92 and 100% in the intervention and control groups, respectively.
Progressions were individually made in the intervention group and this was at the physiotherapist’s discretion. The quality of the exercises performed, the number of sets and repetitions, and the use of additional weights were also adjusted individually. But no criteria for progressions or information is provided. It was however mentioned that the exercises were performed for 10 repetitions at an intensity of 12RM. This is thus approximately 83% of the maximum repetitions possible. While 80% is a good target intensity to exercise, this intensity of 12RM may have been too low to achieve maximal muscle strength increases as often intensities of close to 1RM are advocated to increase maximal strength. This was also shown in a trial by Kubo et al where they found a lower increase in muscle strength with the 12RM protocol than the other protocols (4 or 8RM).

Talk nerdy to me
The study used torque to express the measured strength. This was obtained by multiplying the force in Newton by the lower limb length and dividing by body weight. Hence, the use of torque made comparisons between subjects possible, irrespective of limb length and body weight. Force was measured isometrically in 90° of knee flexion. It would have been interesting to see the results of an isotonic strength test, as this more closely resembles knee functioning. The choice of isometric testing is understandable as it is easy to perform and can easily be replicated. However, these individuals were at least 1-year post-ACL reconstruction, so in this case, isotonic strength measurements would be more informative to document their knee impairments. Although isotonic strength testing is not widely accessible, it would have been interesting to include this besides the isometric dynamometry testing.
A quick side note to mention is that the abstract mentioned that people with a hamstring autograft reconstructed ACL were included, but further, the paper mentioned that a gracilis autograft was also possible. Further, no details about the ACL reconstruction were provided.
The trial was analyzed with an intention-to-treat model and the outcomes were adjusted to possible covariates sex, age, BMI, and baseline scores. The trial was registered a priori, but very brief information was provided and no protocol was published, unfortunately. There is not much to say about the randomization and blinding. These were performed according to the rules.
Take home messages
After progressive strengthening for persistent ACLR hamstring deficits, a large effect size indicated a significantly higher improvement in knee flexor strength compared to usual care. Despite being statistically significant, the difference of 0.18 Nm/kg between both exercise groups did not exceed the minimal important difference of 0.31 Nm/kg that was set before the trial started. Both groups improved over the course of the 12-week duration of the trial, with the largest improvements seen in the progressive strengthening group. These results may be promising to examine over a longer period of time but equally, heavier progressions can be considered in future research.
Learn more
https://physiotutors.com/research/rehabilitation-trajectory-after-acl-reconstruction
https://physiotutors.com/research/accelerated-aclr-rehabilitation-protocol
https://physiotutors.com/research/quadriceps-strength-and-function-after-aclr
Reference
Additional reference
LEARN TO OPTIMIZE REHAB & RTS DECISION MAKING AFTER ACL RECONSTRUCTION
Sign up for this FREE webinar and top leading expert in ACL rehab Bart Dingenen will show you exactly how you can do better in ACL rehab and return to sport decision making
