Research
EBP & Statistics
July 17, 2025
Manual Therapy Mechanisms Explained: Bridging Science and Clinical Practice

Introduction
Manual therapy is defined as the “passive application of mechanical force to the outside of the body with therapeutic intent, often used in pain management (e.g., low back pain), rehabilitation, or general wellness and disease prevention” (NIH, 2021). Common techniques include joint mobilizations, manipulations, and soft tissue therapies. Despite its widespread clinical use, the relevance of manual therapy for orthopedic conditions remains debated.
Initially, its therapeutic effects were attributed to biomechanical mechanisms, such as realigning joints or correcting positional faults. However, contemporary research challenges this perspective suggesting that manual therapy’s benefits may stem from neurophysiological and contextual factors rather than structural changes. While evidence supports its efficacy, effect sizes are generally low to moderate, and outcomes vary significantly among patients.
Given this heterogeneity, identifying which patients are most likely to benefit from manual therapy is crucial. A deeper understanding of its mechanisms could improve patient stratification and treatment personalization. This article synthesizes current knowledge through a systematic, narrative, and scoping review, offering a comprehensive analysis of the scientific literature on manual therapy mechanisms.
Methods
This study integrates a systematic review (structured evidence synthesis), a narrative review (critical thematic analysis), and a scoping review (exploratory evidence mapping) to evaluate manual therapy mechanisms, with findings hosted digitally for ongoing updates.
Eligibility Criteria
Studies investigating manual therapy techniques relevant to physiotherapy practice (e.g., manipulations, mobilizations, soft tissue techniques) were included. Techniques using assistive devices were included only if direct therapist manipulation of the device was required. Invasive techniques (e.g., dry needling, acupuncture) were excluded. Mechanistic domains of interest included neurological, neuroimmune, biomechanical, neurovascular, neurotransmitter, neuroendocrine, and other manual therapy mechanisms. Only in vivo human and animal studies were eligible; cadaveric studies were excluded.
Data Selection
A comprehensive search was conducted across medical databases. Abstracts were screened first, followed by full-text review. Two authors independently performed screening, with discrepancies resolved by a third reviewer. Inter-rater agreement was assessed using Cohen’s kappa score (95% CI).
Data extraction
Two independent authors extracted the following variables from included studies: authorship, publication year, review methodology, searched databases, number of studies analyzed, mechanistic domain(s) investigated, manual therapy interventions, comparison groups, measured outcomes, and key conclusions. Discrepancies were resolved through consensus discussion.
Methodological quality appraisal
The methodological quality of included systematic and scoping reviews was assessed using AMSTAR-2 Risk of bias was evaluated using the ROBIS tool. Two reviewers independently conducted both assessments, with discrepancies resolved through discussion involving a third reviewer. Narrative reviews were exempt from formal quality or bias assessment due to their interpretive nature.
Data analysis and synthesis.
As this study aimed to comprehensively map existing evidence rather than quantify effects, no statistical analysis was performed. Findings were organized by predefined mechanistic domains (neurological, neuroimmune, biomechanical, etc.), with mechanisms not fitting these categories classified as “other.”
Results
The screening process identified 173 potentially eligible articles after initial title and abstract review. Following full-text review, 62 studies met all inclusion criteria and were retained for analysis. The included studies investigated manual therapy (mobilization, manipulation, soft tissue techniques, and massage) across diverse populations: symptomatic, asymptomatic, and unspecified human participants, as well as animal models. Comparators included sham interventions, control groups, or unspecified protocols.
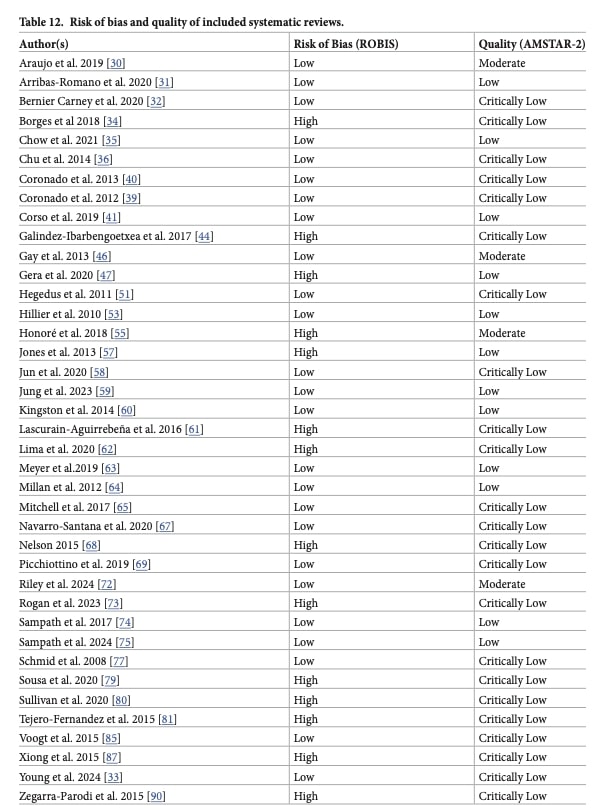
Quality assessment and risk of bias
Of the 62 included studies, 39 underwent formal methodological appraisal (the remaining studies were narrative reviews and were not assessed for quality and risk of bias).
- AMSTAR-2 quality ratings:
- Critically low: 23 studies (59%)
- Low: 12 studies (31%)
- Moderate: 4 studies (10%)
- ROBIS risk of bias:
- High risk: 14 studies (36%)
- Low risk: 25 studies (64%)
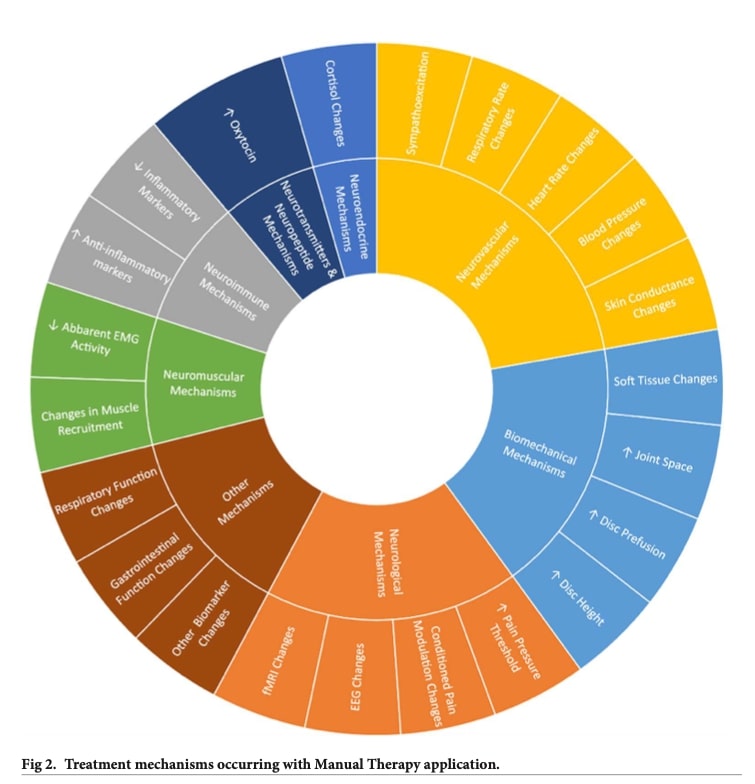
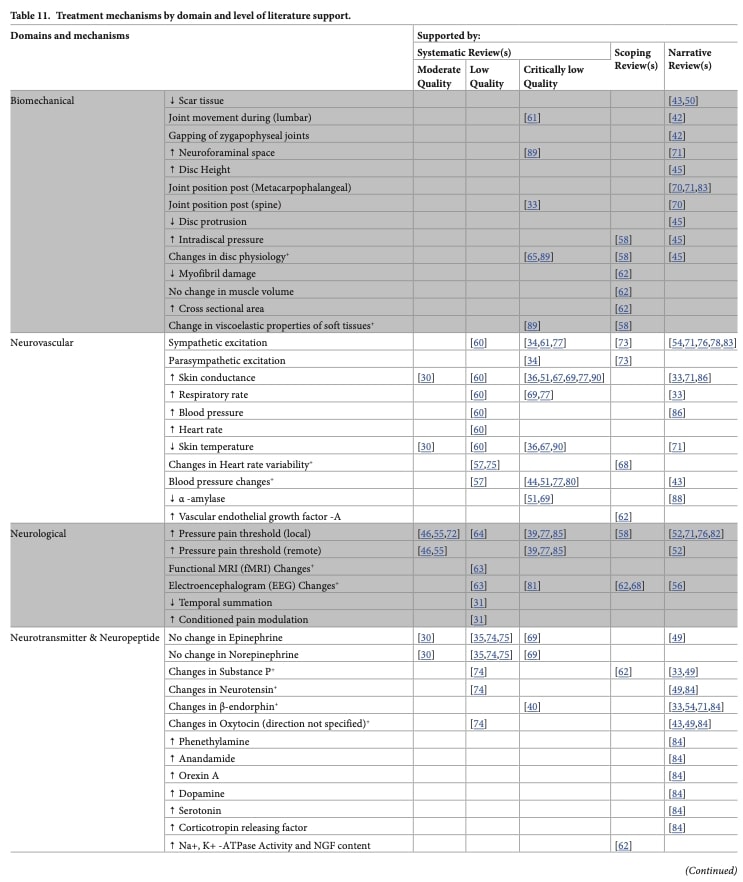
Biomechanical mechanisms
All 14 studies investigating biomechanical mechanisms of manual therapy were critically low quality according to AMSTAR-2 criteria. Among these, five studies reported changes in joint position following manual therapy techniques, though one study found no association between these positional changes and clinical outcomes such as pain or functional impairments. Two reviews 1,2 specifically questioned the validity of biomechanical joint movement principles in cervical spine manual therapy.
Additionally, five studies identified viscoelastic changes in soft tissues resulting from manual therapy, while four studies examined disc-related changes, including modifications in intradiscal pressure. All four-disc studies supported the association between improved disc diffusion and positive clinical outcomes.
Neurovascular mechanisms
Twenty-three studies (critically low to moderate quality) investigated neurovascular responses to manual therapy. The majority of evidence (12 studies) demonstrated sympathoexcitation following treatment. One key review highlighted that the direction of autonomic response depended on intervention intensity—noxious techniques elicited sympathoexcitation, while non-noxious techniques produced sympathoinhibition.
Physiological markers showed mixed results:
- Increased skin conductance (indicating sympathetic activation) was reported in 12 studies
- Decreased skin conductance was observed in one lumbar spine study
- No consistent patterns emerged for heart rate, heart rate variability, or blood pressure
Neurological mechanisms
Twenty-three studies (critically low to moderate quality) examined manual therapy’s neurological effects. Twelve of 20 studies demonstrated that manual therapy increased local pain thresholds (requiring greater force to elicit pain) compared to controls, with no significant difference between manipulation and mobilization techniques. Two reviews found manual therapy matched active physiotherapy for pressure pain thresholds.
Notably, one study demonstrated improved conditioned pain modulation and reduced temporal summation. Other findings included EEG changes, nerve conduction modifications, and cerebral blood flow alterations (7 studies).
Neurotransmitter/neuropeptide mechanisms
Sixteen studies (critically low to moderate quality) investigated neurochemical responses to manual therapy. Key findings included:
- Oxytocin (a hormone linked to stress reduction): Four reviews reported increased levels post-treatment, though one found opposing effects depending on technique (increase after soft tissue mobilization vs decrease after manipulation)
- Substance P (a pain-associated neuropeptide):
- Three of five reviews showed elevation following manipulation
- One study demonstrated reduction after mobilization
- One review found no significant changes
- β-endorphin: While manual therapy generally increased levels, these effects were inconsistent when compared to sham interventions
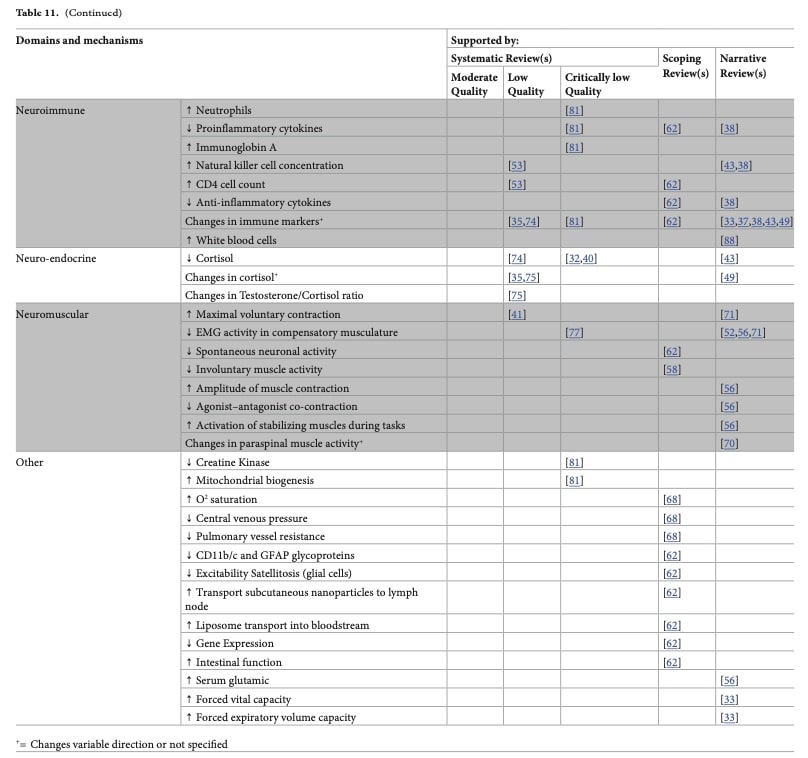
Neuroimmune mechanisms
Twelve reviews (critically low to moderate quality) showed manual therapy may modulate immune function, particularly in symptomatic patients. The most consistent finding was reduced pro-inflammatory cytokines (e.g., TNF-α) with increased anti-inflammatory markers (e.g., IL-10), though results varied. Effects surpassed sham/no-treatment controls in symptomatic populations. Other modulated markers included leukocytes, natural killer cells, and immunoglobulins (IgA/G/M).
Neuroendocrine mechanisms
Twelve critically low to low-quality studies examined neuroendocrine responses to manual therapy, primarily measuring cortisol levels. Most studies found minimal differences between manual therapy, control, and sham groups. However, two reviews reported larger effect sizes for manual therapy, and one study observed longer-lasting effects compared to controls.
Neuromuscular mechanisms
Ten studies (critically low to low quality) examined neuromuscular responses to manual therapy. Key findings included:
- Muscle Spindle Activity: One study reported altered afferent discharge (sensory signals from muscle stretch receptors) following manipulation/mobilization, with effects varying by spinal segment and thrust velocity
- Functional Changes: Post-treatment observations included:
- Increased maximal voluntary contraction
- Reduced resting EMG activity
- Decreased muscle co-contraction
Other mechanisms
Six critically low-quality studies explored additional manual therapy effects. Three demonstrated cardiopulmonary improvements (increased vital capacity, forced expiratory volume, and O2 saturation), while others reported changes in gene expression, intestinal function, and mitochondrial activity, along with alterations in enzyme/protein/amino acid profiles.
Questions and Thoughts
This comprehensive review challenges the traditional biomechanical paradigm of manual therapy, proposing instead that its therapeutic effects may be better explained by neurophysiological mechanisms—including neurological, neurovascular, and neuroimmune pathways. While certain studies did demonstrate mechanical effects (such as altered joint positioning or disc properties), these findings emerged primarily from critically low-quality research. More consistent, though still preliminary, evidence points to mechanisms like pain threshold modulation, autonomic nervous system changes, and inflammatory marker regulation.
The interpretation of these findings must be tempered by significant methodological constraints. Most included studies, particularly those investigating biomechanical effects, were rated as critically low or low quality. Furthermore, the inherent complexity of manual therapy—where neurophysiological effects intertwine with contextual factors like placebo responses and therapeutic alliance—makes isolating specific mechanisms extraordinarily difficult. Even studies employing sham controls struggled to disentangle these interrelated components. Perhaps most critically, while this review maps potential manual therapy mechanisms, it cannot clarify their clinical significance or determine which techniques prove most effective for specific patient subgroups.
One promising thread involves patients with central sensitization. Several studies noted manual therapy’s capacity to reduce temporal summation and enhance conditioned pain modulation—effects potentially mediated through descending pain inhibitory pathways, as detailed in this trial. This suggests manual therapy might hold particular value for this patient population, though rigorous phenotyping systems remain to be developed.
These findings underscore the need for: (1) higher-quality mechanistic studies that account for multimodal influences, and (2) clinical trials pairing mechanistic measures with patient stratification. The “Talk Nerdy to Me” section that follows will delve deeper into the methodological challenges confounding this field of research.
Talk nerdy to me
This living systematic and scoping review offers an exhaustive examination of manual therapy mechanisms, yet the high heterogeneity among included studies—combined with their generally low methodological quality (ranging from critically low to moderate)—makes drawing definitive conclusions challenging. This reality forces us to confront fundamental questions about how manual therapy research should be conducted.
As highlighted in a recent editorial, emerging observational evidence indicates that anterior and posterior mobilizations may produce enhanced long-term benefits when applied to patients demonstrating favorable initial responses to treatment. However, while clinical trials demonstrate promising results – including approximately 30% pain reduction following manual therapy interventions – these studies face significant methodological limitations. Crucially, they cannot adequately isolate the specific therapeutic effects of manual therapy from potentially confounding variables such as contextual treatment factors and placebo responses that inherently accompany hands-on interventions.
The editorial authors propose these clinical improvements may reflect individual variations in endogenous pain-modulation capacity identifiable during initial examination. To test this hypothesis, a concurrent validity study design would be essential—one that combines clinical assessments with laboratory-based evaluation of pain adaptive behavior. The cold pressor test offers a validated experimental approach for this purpose, quantifying whether subjects develop decreased sensitivity (adaptive response) or increased sensitivity (non-adaptive response) to sustained noxious stimuli. A strong correlation between adaptive responses and the 30% improvement threshold following posterior-anterior mobilization would provide the first evidence for a clinically practical marker of pain adaptability.
Should this correlation between pain adaptability and clinical improvement be confirmed, establishing a causal link would require responder analyses through controlled trials. While randomized controlled trials (RCTs) represent the gold standard, the editorial authors note their inherent limitation in matching participant characteristics across study arms. They propose crossover designs (figure 1) as an alternative solution, where participants serve as their own controls through sequential treatment phases separated by washout periods. In this model, subjects would be randomized to receive either manual therapy or active comparator (e.g., exercise) first, followed by a washout period before crossing over to the alternate intervention.
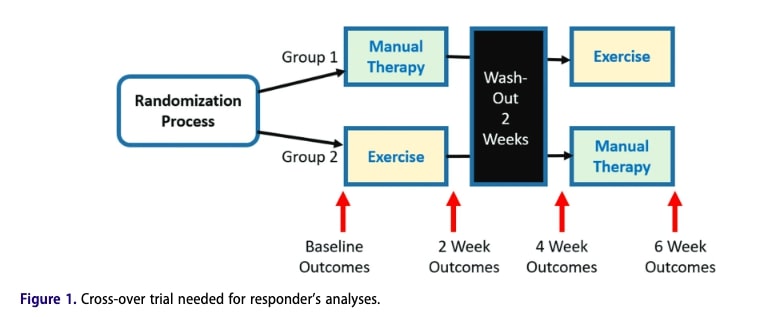
However, this approach presents practical challenges for musculoskeletal conditions like low back pain, where symptom fluctuation and natural history complicate the determination of adequate washout procedure. This fundamental constraint underscores the need for innovative study designs that can isolate treatment-specific effects while accounting for the dynamic nature of orthopedic conditions.
Take-home messages
Mechanistic Complexity: This review provides the most comprehensive synthesis of manual therapy mechanisms to date, revealing intertwined neurophysiological, biomechanical, and immune responses. However, the predominance of low-quality studies and inherent complexity of these interventions limit definitive conclusions.
Clinical Translation Gap: While identified manual therapy mechanisms (e.g., pain modulation, autonomic changes) show promise, their clinical relevance remains unclear due to individual variability and contextual factors
Optimizing Practice: Clinicians should use test-retest strategies—assessing immediate changes in pain/function—to identify likely responders during initial treatment
Methodological Challenges: Conventional study designs (e.g., RCTs) struggle to isolate manual therapy’s specific effects from placebo and contextual components. Innovative approaches—such as mechanism-targeted subgroup analyses—are needed.
Clinical Resources:
- Master 150+ manual therapy techniques: Physiotutors Manual Therapy App
- Deepen theoretical knowledge: Manual Therapy Podcast
Reference
5 ESSENTIAL MOBILIZATION / MANIPULATION TECHNIQUES EVERY PHYSIO SHOULD MASTER
Learn 5 essential mobilization / manipulation techniques in 5 days that will skyrocket your manual therapy skills immediately – 100% For Free!