Research
Pain & Psychosocial
April 20, 2026
Sleep Dysfunction in Musculoskeletal Pain - Part 2: Management of Sleep Dysfunction in Musculoskeletal Care

Introduction
Following our research review part 1, we’ll dive a little deeper into the management of sleep dysfunction in musculoskeletal care. The paper by Shepherd et al. (2026) is worth a second, separate review because its most clinically useful contribution is not merely that sleep matters, but that it shows what physiotherapists can realistically do about sleep dysfunction in musculoskeletal care. Poor sleep is often acknowledged but not systematically managed, even though sleep disruption is closely linked to greater pain sensitivity, emotional dysregulation, impaired recovery, and ongoing disability. The authors argue that sleep should not be viewed only as a symptom of pain but also as a parallel contributor to the persistence of pain and reduced function. That makes it worthwhile to dive deeper into sleep dysfunctions when deemed predisposing factors to the onset and persistence of pain problems.
Methods
The study we review here today is a clinical commentary, and with that being said, you must be aware that this does not reflect experimental studies like we use to review.
Therefore, there is no statistical analysis, no participants were included, and no intervention was delivered. Rather, the authors employed a pragmatic way of helping us screen for and address sleep dysfunctions in clinical practice. To do that, the existing literature was reconciled with clinical guidelines and prior frameworks. Their practical focus is on integrating selected principles from cognitive behavioral therapy for insomnia, or CBT-I, into physiotherapy management, while staying within the physiotherapist’s scope.
Results
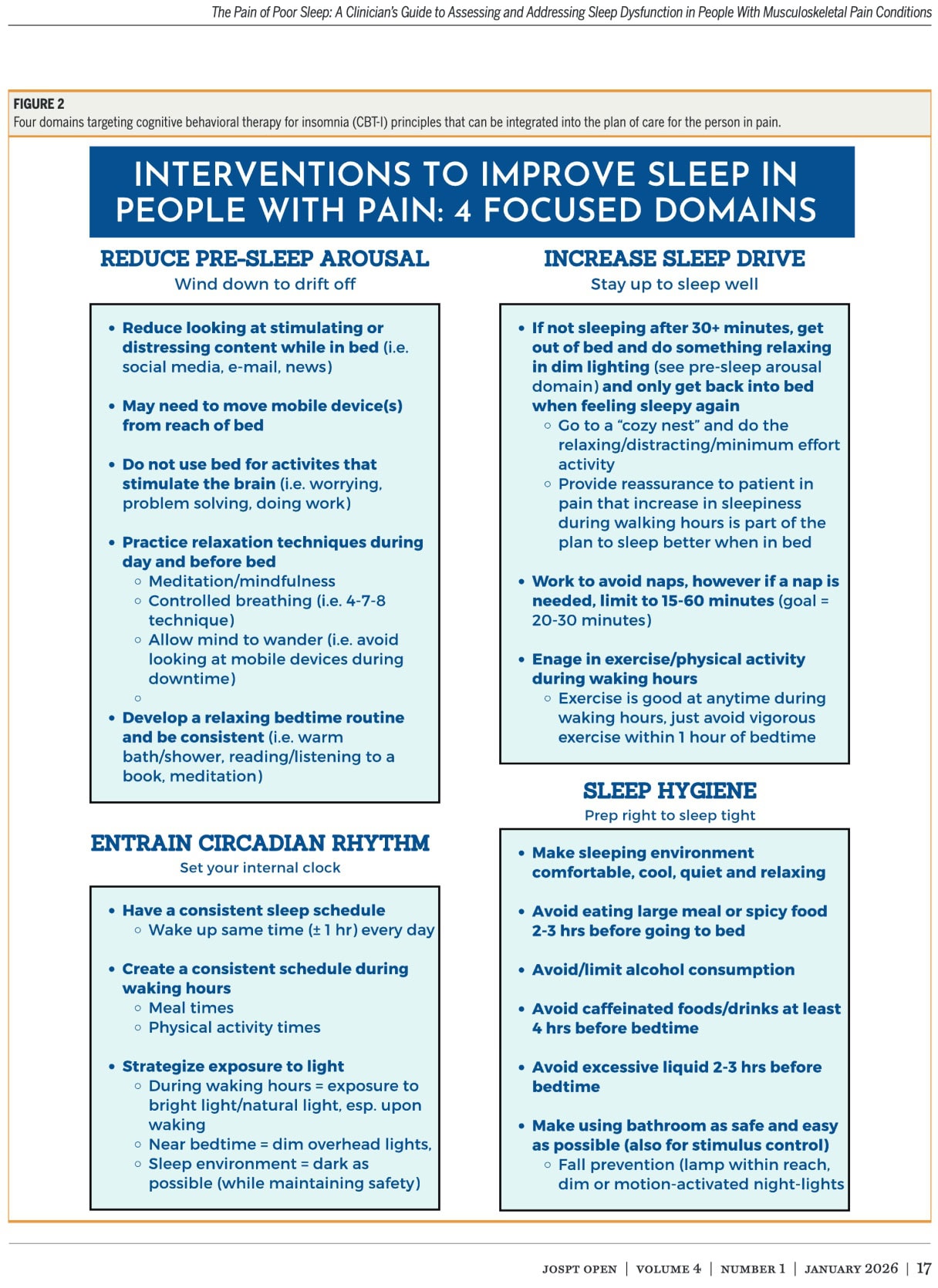
The authors describe four core pillars of management of sleep dysfunction in musculoskeletal care.
Pillar 1: Reducing Presleep Arousal: Wind down to drift off
A prerequisite for a good night’s sleep is getting that sleepy feeling before you tuck into bed. When your body or mind remains too activated, due to thoughts, pain-related rumination, stimulating content (for example: TV, social media,..), you make it harder to fall asleep.
To counter that, the authors suggest that physiotherapists can guide patients to reduce stimulating pre-bed activities, especially screen use, distressing media, or work-related engagement in bed.
When negative thoughts, anxiety, and stress is present, strategies such as deep breathing, progressive muscle relaxation, journaling, mindfulness, and scheduling time earlier in the day to process worries and thoughts, so that bedtime is less cognitively loaded, are suggested. A key behavioral principle should be kept in mind: the bed should be reserved for sleep and intimacy, not for problem-solving, catastrophizing, or prolonged wakeful rumination.
Pillar 2: Increasing Sleep Drive: Stay up to sleep well
Sleep drive refers to the buildup of sleep pressure across the waking day. To support this, the authors recommend limiting naps, reducing time spent awake in bed, and using some control principles. For example, if a patient cannot fall asleep within roughly 20 to 30 minutes, they should get out of bed and do a quiet, nonstimulating activity in dim light until they feel sleepy again.
In addition, the paper highlights appropriately timed exercise as a way to promote sleep pressure and reinforce the sleep-wake cycle, with the caveat that vigorous exercise should be avoided within one hour of bedtime. For the physiotherapist, this domain is especially relevant because daytime physical activity, exercise dosage, and behavioral activation are already familiar parts of rehabilitation. The authors also note that patients may need reassurance that some temporary daytime fatigue can occur when these behavioral strategies are first introduced.
Pillar 3: Entrain Circadian Rhythm: Set your internal clock
The key to good sleep? Regularity! Maintaining a consistent wake time within about one hour each day, including weekends, is recommended because this appears important in anchoring the body clock. The authors also advise looking at daily routine more broadly, including consistency of meals, activity, and social timing, since irregular lifestyle patterns may worsen circadian disruption.
Light exposure is treated as a major intervention tool. The authors recommend morning natural light exposure after waking and reducing bright artificial light in the one to two hours before bedtime. But what if your patient works in shifts? It can be helpful for shift workers to keep the sleep environment dark during daytime sleep and use sunglasses after a night shift to reduce morning light exposure. For musculoskeletal physiotherapists, this domain is relevant because chronic pain often disrupts daily routine, work status, and physical activity patterns, further disrupting sleep.
Pillar 4: Sleep Hygiene: Prep right to sleep tight
The authors suggest common behavioral and environmental recommendations that support sleep, such as maintaining a quiet, cool, dark sleep environment and avoiding caffeine, alcohol, nicotine, and heavy late meals. However, they are clear that sleep hygiene alone has limited effectiveness, especially in persistent insomnia or pain-related sleep dysfunction. In this commentary, sleep hygiene is presented as an adjunct rather than a stand-alone intervention. The authors also sensibly note that certain sleep hygiene recommendations may be unrealistic for some patients because of financial or environmental limitations, so clinicians should use judgment rather than provide generic advice without context.
Questions and thoughts
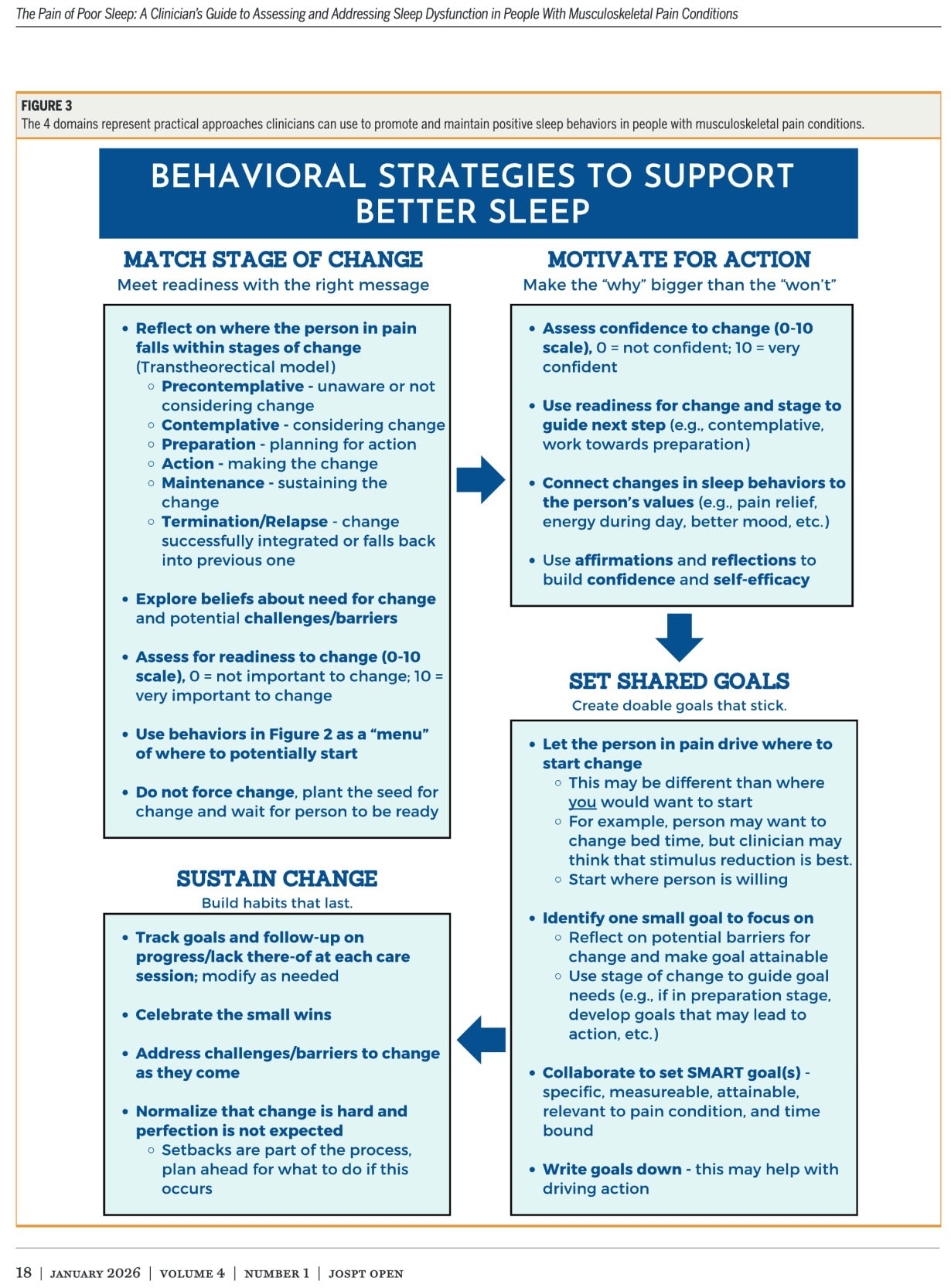
This clinical commentary provides a practical intervention framework for physiotherapists managing people with musculoskeletal pain and concurrent sleep dysfunction. The approach remains focused on clinician-deliverable behavioral strategies rather than diagnosis of sleep disorders, and it positions physiotherapists as providers of sleep health support within a stepped-care model.
These four pillars are based on cognitive behavioral therapy principles for insomnia (CBT-I). The authors conclude that CBT-I is the first-line nonpharmacological treatment for insomnia and that its principles can be partially integrated into physiotherapy practice when treating people with musculoskeletal pain, as it has demonstrated long-term benefits for sleep quality and pain outcomes.
Just like with CBT for pain problems, this approach aims to facilitate self-management by addressing the individual psychological contributors. Importantly, the authors do not expect physiotherapists to deliver full CBT for insomnia (CBT-I), but rather to integrate the core behavioral principles into musculoskeletal care.
We must acknowledge that this is not a definite piece of evidence, but merely a framework. While helpful, the recommendations have not been tested in randomized clinical trials, and that should be remembered when interpreting these findings.
Talk nerdy to me
The primary limitation of this clinical commentary is its pragmatic approach, which bypasses a systematic review process, inherently raising the risk of bias. The absence of a systematic search strategy, predefined inclusion criteria, and risk-of-bias assessment means the selection of evidence is not transparent. Consequently, the authors may have introduced selection bias by preferentially including studies that support their proposed framework. The conclusions, therefore, must be interpreted cautiously, given the lack of direct empirical validation, reliance on secondary evidence, and non-systematic methodology. Furthermore, the inherent lower level of evidence in a clinical commentary, compared to randomized controlled trials or systematic reviews, must be acknowledged.
Despite its methodological limitations, the commentary offers significant strengths in clinical application. It provides a highly generalizable and pragmatic, stepwise framework for use in clinical practice. The authors successfully synthesized complex, multidisciplinary evidence from sleep medicine, psychology, and pain science into a readily implementable tool for physiotherapists. This approach is designed to assist clinicians in screening for sleep disorders related to musculoskeletal pain and guiding referral decisions when necessary. Importantly, it maintains the current scope of practice, aiming to support the clinician rather than demanding expertise in sleep disorders. The paper ultimately delivers a clinically valuable, theory-informed framework.
Take-home messages
Disturbed sleep is not just a symptom; it actively drives pain and recovery. When patients report sleep disturbances, rather than just documenting that, we should go further and screen for potential underlying drivers of musculoskeletal pain conditions. If sleep dysfunction is identified and considered as a factor underlying the development of or persistence of the musculoskeletal pain condition, as highlighted in our previous research review, we can refer the patient for further assessment by sleep experts. Nonetheless, the current review emphasizes that the physiotherapist can support better sleep by targeting four areas: reducing presleep arousal, increasing sleep drive, regularizing circadian rhythm, and using sleep hygiene as an adjunct rather than a stand-alone treatment.
Reference
100% FREE POSTER PACKAGE
Receive 6 High-Resolution Posters summarising important topics in sports recovery to display in your clinic/gym.