
Research
EBP & Statistics
June 1, 2026
Lumbar Motor Control Tests: When a Statistical Difference Isn't a Clinical Win

Introduction
Lumbar motor control (LMC) is frequently proposed as an important factor in chronic non-specific low back pain (NSCLBP), and several test batteries have been developed to identify motor control deficits. One such battery is the test battery proposed by Adelt et al. (2021), which contains direction-specific tests for flexion, extension, and rotation/lateral flexion. Earlier research, however, demonstrated that the flexion-related tests in this battery were extremely easy, meaning most people passed them regardless of whether they had low back pain or not. As a result, the question arises whether these tests had the ability to discriminate between individuals with better or worse movement control, or whether these tests were valid to measure the construct of lumbar motor control. Four new flexion-based tests were integrated into the existing test battery, and the current study investigated whether these newer tests were more challenging and therefore potentially more useful from a measurement perspective. An important distinction is that this study did not investigate whether lumbar movement control causes low back pain, nor whether improving movement control improves outcomes. Instead, it examined whether the tests themselves were psychometrically better at differentiating between participants with and without chronic low back pain.
Methods
This cross-sectional study included participants with nonspecific chronic low back pain (NSCLBP) and asymptomatic controls. Patients with NSCLBP reported low back pain for at least three months. Exclusion criteria encompassed people with specific spinal pathology, previous spinal surgery, neurological deficits, fractures, tumors, or inflammatory disorders.
Demographics and the Oswestry Disability Index (ODI), the Fear Avoidance Beliefs Questionnaire (FABQ), and the Fremantle Back Awareness Questionnaire (FreBAQ) were administered.
The participants performed eight flexion-related movement-control tests:
- Forward bend
- Unilateral knee extension
- Chest drop
- Rocking backwards
The 4 new tests were:
- Waiter’s bow
- Deep squat
- Box lift
- Bilateral knee extension
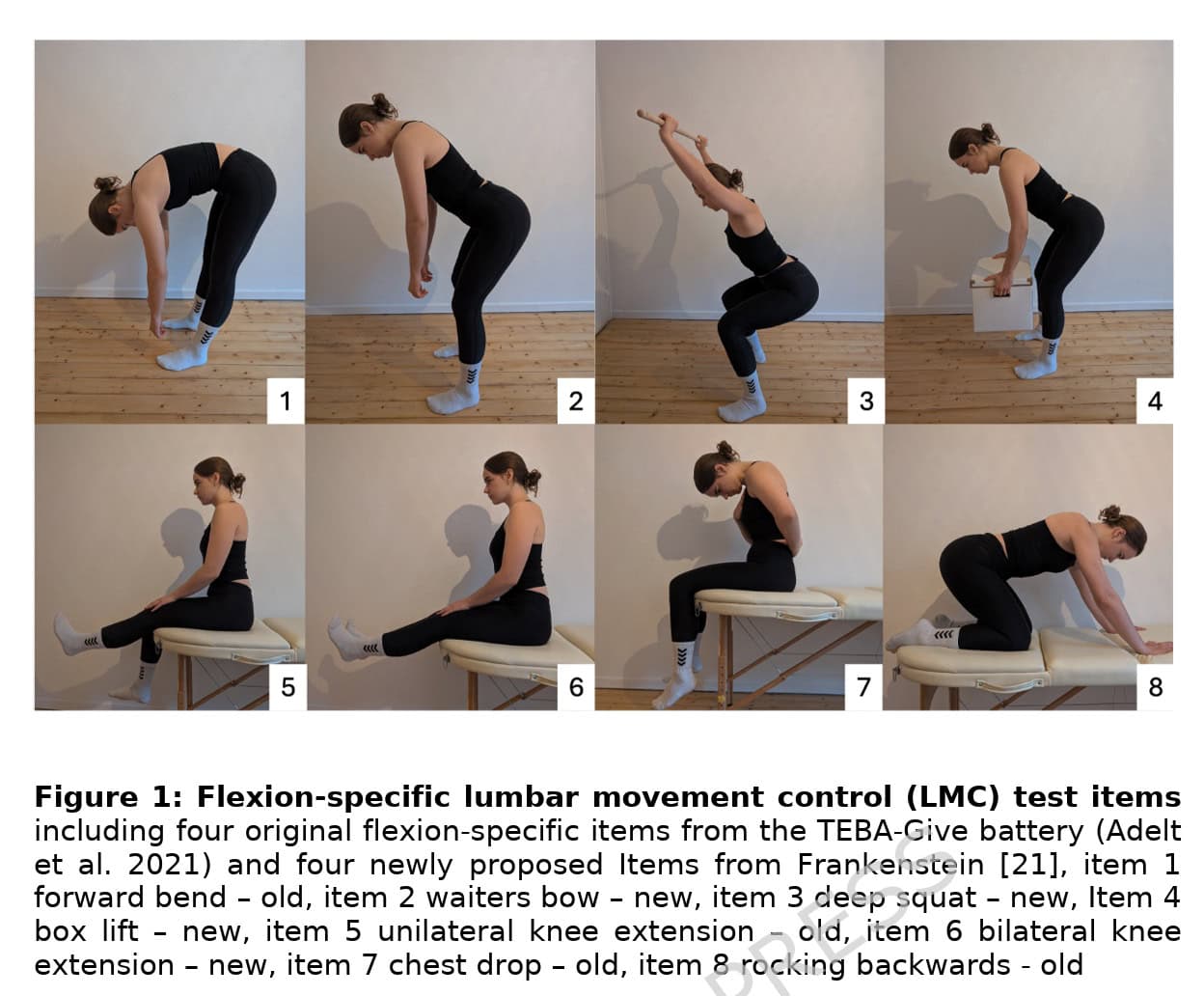
Each of these tests was explained to the participants using a standardized script. A physiotherapist blinded for group allocation rated the test execution visually in real time. The tests were dichotomously rated as either correct or incorrect, based on subjective visual inspection.
Results
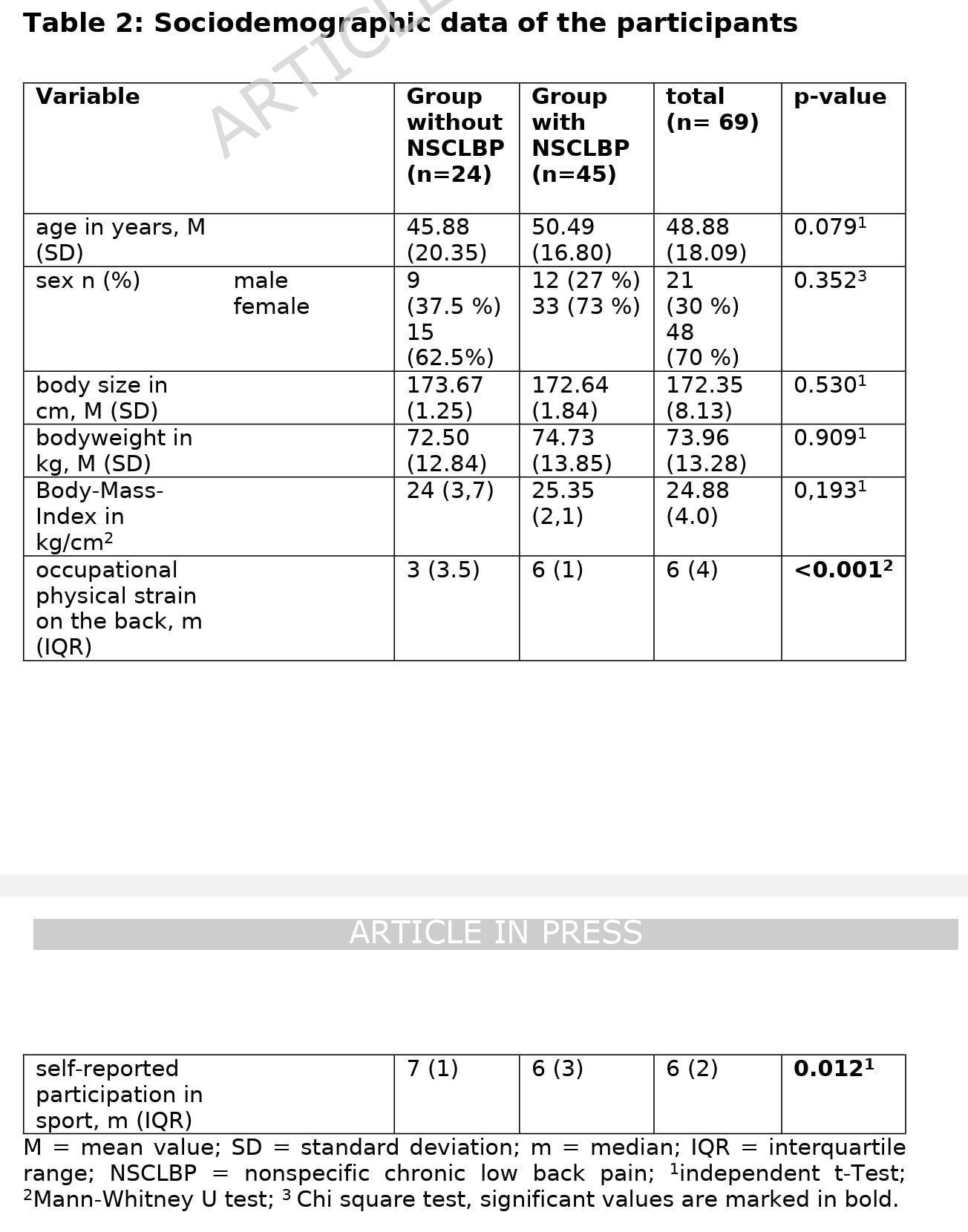
Sixty-nine participants were included, of whom 45 had NSCLBP, and 24 were healthy controls. The comparison of their data at baseline revealed that patients with NSCLBP reported higher physical strain than those without, and on the other hand, the healthy controls had a slightly higher self-rated participation in sports on a 0-10 numeric rating scale.
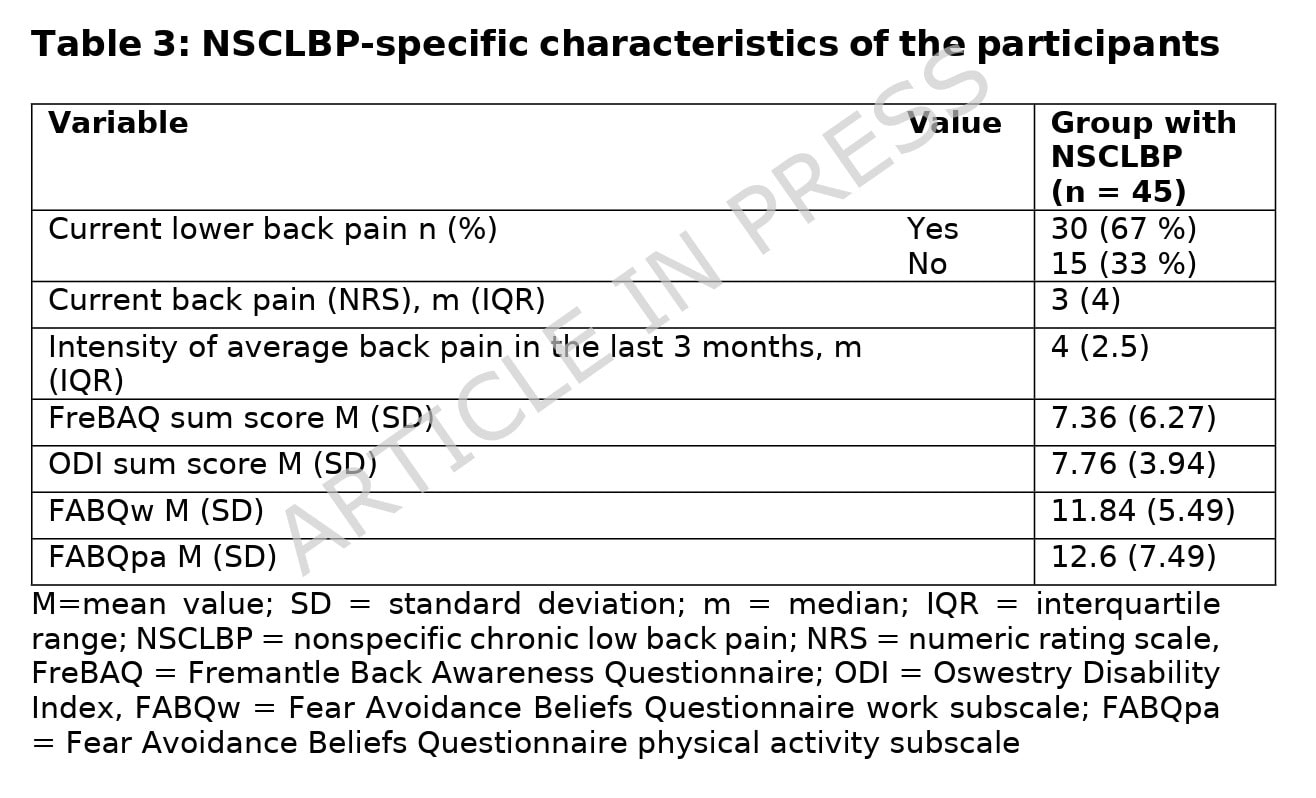
The patients with NSCLBP were relatively mildly affected with a low median pain intensity of 3/10 and a mean ODI of 7.8 points.
Across all participants, 22% of the movements were rated as incorrectly performed. When the group was divided into NSCLBP patients and healthy controls, the results showed that those affected had 25% of items performed incorrectly, compared with 17% in the controls.
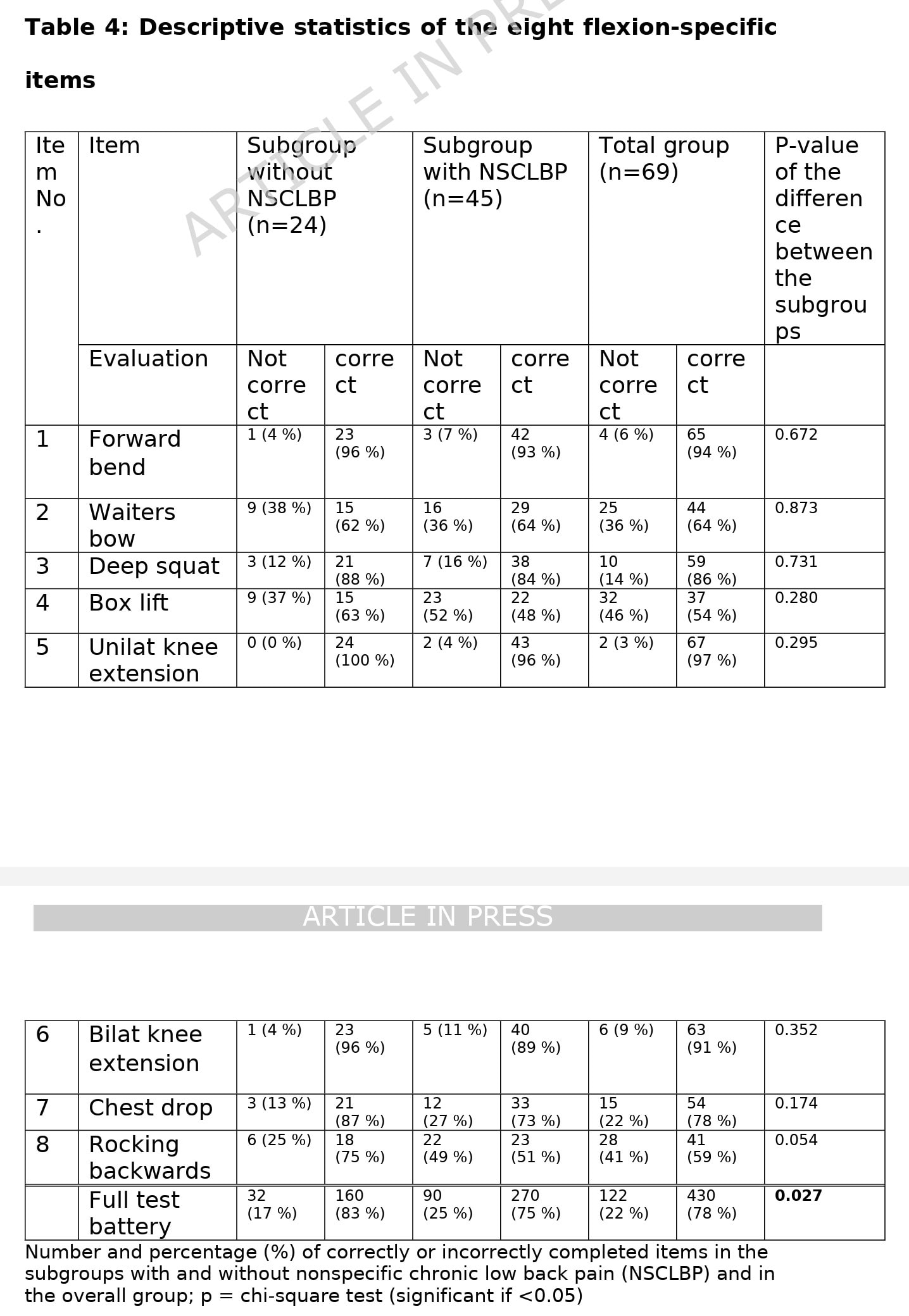
The rates of correctly performed movements were monitored, and revealed that the forward bend was the test item most often performed correctly (and thus the easiest). The hardest movement performed correctly was the box lift, with 46% of the participants performing it incorrectly: 37% of the controls and 52% of the participants with NSCLBP.
Each of the lumbar motor control movements was compared between those with and without NSCLBP, but none reached a significant between-group difference. The authors, however, reported that the difference in total correct performance between the groups was statistically significant: patients with NSCLBP performed on average 5 out of 7 movements correctly, compared to 6 out of 7 in the control group. Item 5 was excluded from this analysis because, apparently, a very high correlation with item 6 could have led to model distortion.
Questions and thoughts
First things first. Statistical significance is not always clinically meaningful. Interestingly, none of the individual motor control tests differed significantly between participants with and without NSCLBP. Only when the tests were combined into a total score did this lead to a statistically significant difference. While this may reflect the accumulation of multiple small between-group differences, it also suggests that no single motor control test was able to meaningfully distinguish the groups on its own. Furthermore, the difference of having only one more correctly performed test (5 vs. 6 out of 7) raises questions about the clinical relevance of the finding despite its statistical significance. Combined with the uncertain validity of motor control constructs, these results indicate inter-individual differences, possibly related to movement variations and adaptations, rather than evidence of a motor control impairment associated with NSCLBP.
Interestingly, none of the individual tests significantly differentiated participants with and without NSCLBP. The statistically significant finding only emerged after combining all items into a total score. This raises the question of whether the field is attempting to optimize measurement precision for a construct that demonstrates only modest group differences to begin with. If individual tests cannot meaningfully distinguish between people with and without NSCLBP, it becomes reasonable to ask whether the primary limitation lies in the tests themselves or in the underlying construct they are intended to measure.
Although we must be clear that the purpose of this cross-sectional study was to determine the item-difficulty of flexion-related lumbar motor control tests and compare them against one another, we also must remain critical of the purpose of the tests for clinical practice. Lumbar motor control is a topic that emerged primarily from the work of Panjabi, Hodges, Richardson, O’Sullivan, Sahrmann, and others during the 1990s and early 2000s. The theory proposes that some individuals with low back pain have an impaired ability to control movement and loading of the lumbar spine. Panjabi’s influential spinal stability model suggested that spinal stability depends on the interaction between passive structures (vertebrae, discs, ligaments), active structures (muscles and tendons), and the neural control system. According to this model, dysfunction in one subsystem requires compensation from the others to maintain spinal stability. This concept led to the idea that altered muscle activation or movement patterns could contribute to pain or injury.
The theory gained considerable popularity after studies reported delayed activation of the transversus abdominis and multifidus muscles in some patients with low back pain. These findings were interpreted as evidence that the deep stabilizing muscles of the spine were not functioning optimally, leading to the development of motor control exercises and “core stability” training to restore normal activation patterns.
Over time, however, several criticisms of the theory have emerged. One major issue is the lack of a clear definition of what “normal” movement is. Human movement is highly variable, and healthy individuals often use very different movement strategies to perform the same task. As a result, it remains unclear when movement variation should be considered dysfunctional. Think of different tennis players: while they all play the same game with forehands and backhands, they can show different movement strategies to produce the same strike of the ball. And even in the top players, a lot of movement variation exists.
So, while many studies have identified movement differences in people with low back pain, these findings do not establish causation. Movement changes may be a consequence of pain, a protective adaptation, or simply a preferred movement strategy rather than the cause of symptoms.
Another challenge is that research findings regarding motor control impairments have been inconsistent. Studies have reported delayed, earlier, increased, and decreased muscle activation patterns in people with low back pain, suggesting that there is no single motor-control deficit that characterizes all patients. This has led researchers to argue that motor-control adaptations in low back pain are highly diverse and individualized rather than representing a dysfunction. Additionally, although motor control exercises can be effective for chronic low back pain, they generally do not outperform other active interventions such as strength training, walking programs, or general exercise by large margins.
The most important criticism, in my opinion, is that movement-control frameworks can (unintentionally) reinforce unhelpful beliefs about the spine. When patients are told that they have poor movement control, an unstable spine, or faulty movement patterns, they may develop fear, hypervigilance, and movement avoidance. These psychological responses are themselves associated with persistent pain and disability. Consequently, many modern researchers now view altered movement patterns less as pathological deficits and more as context-dependent adaptations that may reflect an individual’s response to pain, previous experiences, physical demands, or beliefs. The field has therefore shifted from asking how to correct “motor control deficits” toward questioning whether the identified movement patterns are truly dysfunctional and whether they are clinically meaningful drivers of pain in the first place.
A broader concern is that motor control frameworks often begin with the assumption that there is a correct and incorrect way to move. Once movement variation is classified as a deficit, clinicians may feel compelled to identify and correct it, even when evidence linking that movement pattern to pain, injury, or prognosis is lacking. In this way, normal human movement variability risks becoming medicalized. The consequence is that patients may leave the consultation believing that their spine is unstable, vulnerable, or dependent on constant conscious control. Such beliefs may ultimately be more disabling than the movement pattern itself.
I often see patients in practice who are desperately trying to fix their postures, but who seek help because they can not tolerate the so-called perfect-picture posture for long periods of time. In many cases, these attempts to be “upright” are creating increases in their muscle tone, hypervigilance, fear of movement, and most often, despair. Telling them to try and move more naturally, switching positions, standing up, and walking around frequently is sometimes such a mind-blowing cure for their self-determined “bad” posture and movement.
The authors investigated which flexion-related movement-control tests are more difficult to perform. However, before refining these tests, we should first ask whether they actually measure a clinically meaningful impairment. The study assumes that lumbar motor control is a construct that can be identified through visual observation and that impairments are relevant to chronic low back pain. Yet this assumption remains debated. In fact, the authors themselves cite a recent systematic review concluding that the validity of clinically assessed lumbopelvic sensorimotor control tests is supported by low to very low-quality evidence. If the underlying construct is uncertain, improving the psychometric properties of the tests may simply make us better at measuring something whose clinical relevance remains unclear.
The findings also resemble those of Larsson et al. (2024), who found no differences in lumbopelvic movement-control test performance between powerlifters with and without low back pain. This raises the possibility that what clinicians often interpret as motor control deficits may sometimes represent normal movement variability, task-specific adaptations, or simply different movement strategies rather than dysfunction.
Another concern is how movement-control frameworks are translated into clinical practice. If a patient is told that they have “poor movement control” or that they are moving “incorrectly,” this can easily reinforce beliefs that the spine is fragile, unstable, or requires constant protection. Such narratives may contribute to fear, hypervigilance, and movement avoidance, factors that are themselves associated with persistent pain and disability. Ironically, the consequences of believing that movement is dangerous may be more clinically relevant than the so-called “wrong” movement pattern itself.
Importantly, this study did not show that these movements such as lumbar flexion or lifting were harmful. Yet, these kinds of research articles may be easily mistranslated as “movement faults” or uncontrolled movements of the spine, a type of nocebo language that may be more harmful for the patient than intended, but possibly intertwined with the lived experience.
Talk nerdy to me
The authors used Item Response Theory (IRT), a psychometric approach that evaluates how informative a test is across different levels of ability. Instead of simply looking at pass/fail percentages, IRT estimates how difficult each test item is and how well it discriminates between people with different levels of the underlying construct, in this case, flexion-related lumbar motor control.
The box lift was the most difficult item, while the forward bend was the easiest. However, all tests demonstrated negative difficulty values, meaning that even individuals with below-average motor control ability still had a reasonable probability of performing them correctly. This suggests the flexion subscale primarily targets lower levels of ability and has limited usefulness for identifying subtle deficits in higher-functioning individuals.
While the psychometric analysis was rigorous, it cannot solve a more fundamental issue: construct validity. A test can be reliable, statistically sophisticated, and internally consistent while still measuring something that lacks clinical relevance. This problem is similar to what we discussed in our review of Areeudomwong et al. (2020) on clinical lumbar instability. There too, diagnostic accuracy calculations were built upon a construct without a universally accepted gold standard.
Another limitation is that all movement assessments relied on visual observation. Although the authors standardized procedures and blinded assessors, visual movement analysis remains subjective. Without objective biomechanical measures, it remains difficult to determine whether an observed movement pattern reflects impaired control, pain-related adaptation, normal variability, or merely a preferred movement strategy.
Take-home messages
This study found that people with chronic non-specific low back pain performed slightly worse on flexion-related motor control tests than asymptomatic controls. The newly proposed tests, particularly the box lift and waiter’s bow, were more difficult than the original flexion tests and improved the psychometric characteristics of the test battery. However, the difference between groups was small, with only one test item, which is likely clinically irrelevant.
Reference
MASSIVELY IMPROVE YOUR KNOWLEDGE ABOUT LOW BACK PAIN FOR FREE
5 absolutely crucial lessons you won’t learn at university that will improve your care for patients with low back pain immediately without paying a single cent
