
Research
Head/Neck
February 17, 2025
The influence of hamstring flexibility on CCFT endurance performance

Introduction
Fascia is a continuous network of connective tissue between muscles, bones, organs, nerves, and blood vessels in our bodies. It protects, connects and supports all connected tissues. Zügel et al in 2018 published a consensus statement about fascia and defined fascia as “A three-dimensional continuum of soft, collagen-containing, loose and dense fibrous connective tissue that permeates the body and enables all body systems to operate in an integrated manner.” Since fascia forms a network, many researchers have tried to find links between different body parts. The current study aimed to look into possible connections between the cervical spine and the flexibility of the hamstring muscle group. The authors hypothesized that since the deep neck flexors affect cervical posture, a transfer of tension along the so-called superficial backline could affect tension and flexibility of the hamstrings. Thus the current study used the well-known craniocervical flexion test (CCFT) and a range of motion assessment to investigate differences between people with and without hamstring flexibility limitations. The aim was to examine the influence of hamstring flexibility on CCFT endurance of the deep cervical spine flexor muscles and active cervical range of motion.
Methods
In this cross-sectional study, healthy college students between 18-25 years were enrolled. Using a smartphone application (Clinometer) on the anterior thigh proximal of the upper border of the patella, the participants were assessed for hamstring flexibility using the passive straight-leg raise test. The result was dichotomized into limited hamstring flexibility, when the angle of 70° could not be attained, or in normal flexibility for angles exceeding 70°.

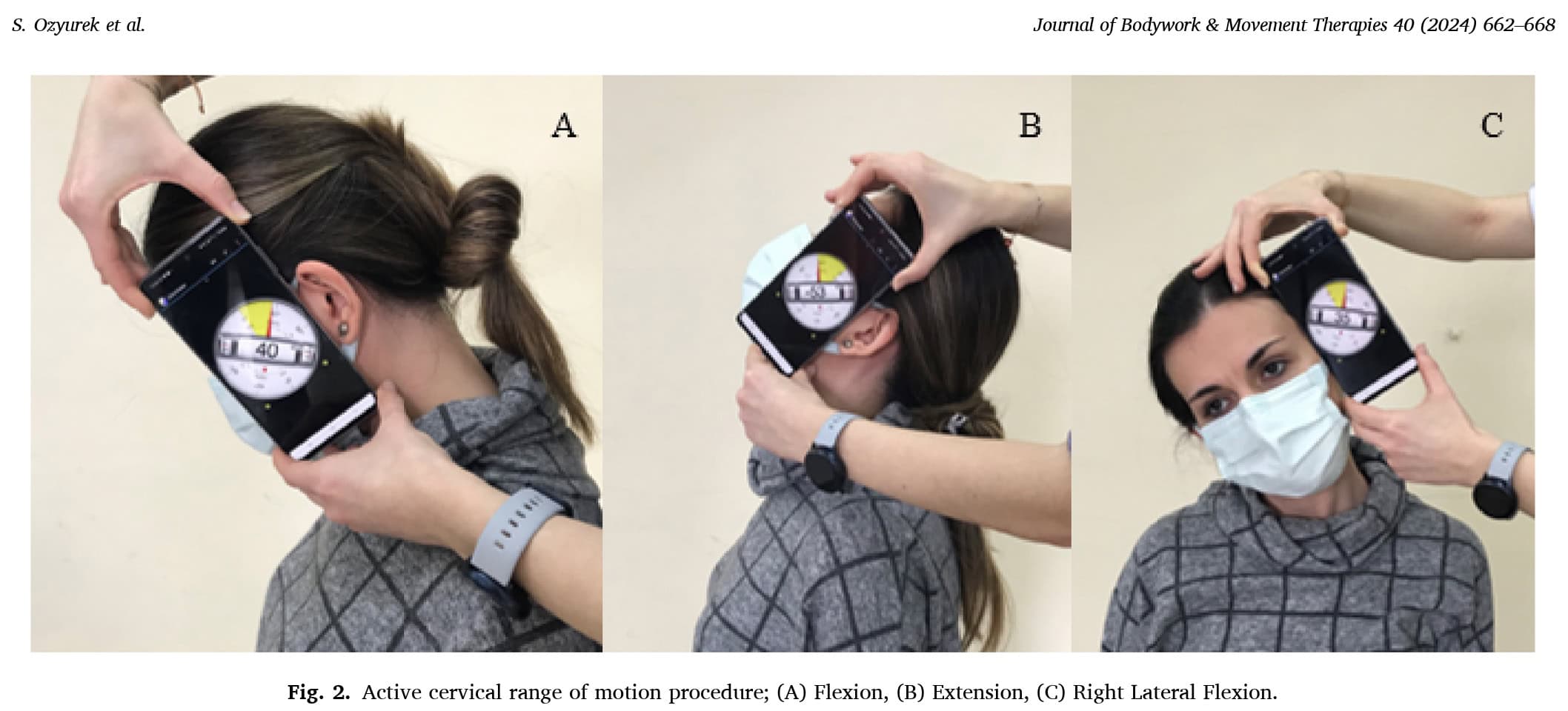
The same smartphone application was used to determine the participants’ active range of motion of the cervical spine. With the participants seated upright on a chair, the inclinometer app was placed “vertically in front of the participant’s ear for flexion and extension and on the contralateral side of the head aligned with the participant’s eyes for lateral flexion”. An average of three subsequent movements was calculated.
Deep neck flexor endurance was assessed using the craniocervical flexion test (CCFT), using a visual biofeedback device (Stabilizer).
The execution of the CCFT is described in the video below, but an additional calculation method was used, which I explain under the video.
The only difference between the video and the study was that in the study currently under review, the progression to the next pressure level was only made when the participant could successfully maintain a craniocervical flexion movement ten consecutive times 10 seconds. In the video, only three 10-second hold repetitions are mentioned.
From the CCFT, the performance index and the highest pressure score were calculated accordingly:
- The highest pressure score in mmHg is the maximal pressure level (22, 24, 26, 28 or 30 mmHg) the participant can maintain 10 repetitions for 10 seconds with correct execution.
- The performance index is calculated by multiplying the pressure level by the number of correct repetitions performed. For example, when a participant reaches the level of 24 mmHg (being the 4th level from 20 mmHg) and can hold it correctly for 10 seconds for 6 times, the performance index is 4×6=24. When the pressure level of 30 mmHg is achieved for 10 correct 10-second repetitions, the performance index reaches its maximum of 10×10=100.
Results
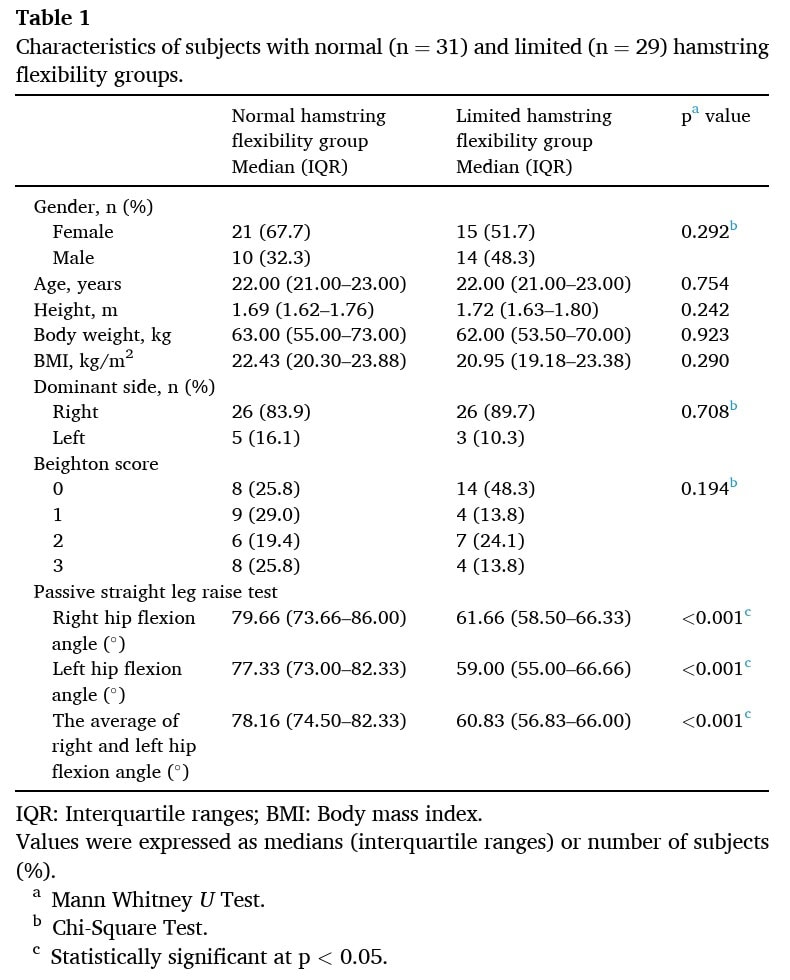
Sixty participants were included in the cross-sectional study. A total of 36 females and 24 males were included. At baseline, their characteristics were equal, except for the number of participants showing a higher Beighton score in the normal hamstring flexibility group.
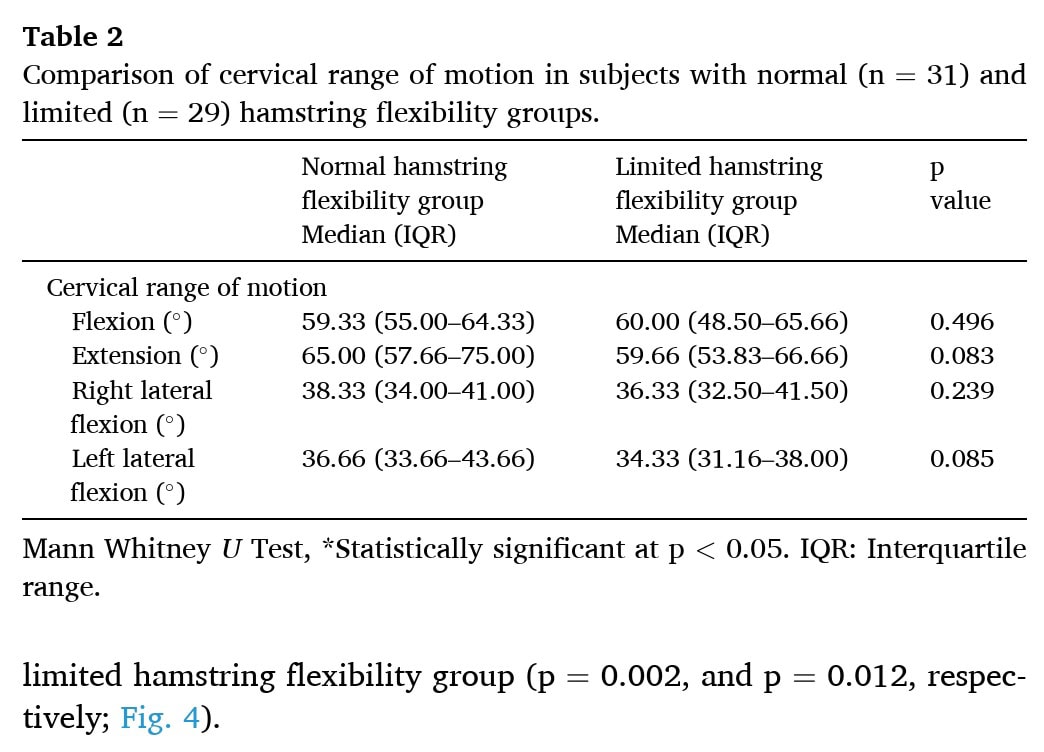
No significant differences in active cervical range of motion emerged between the groups.
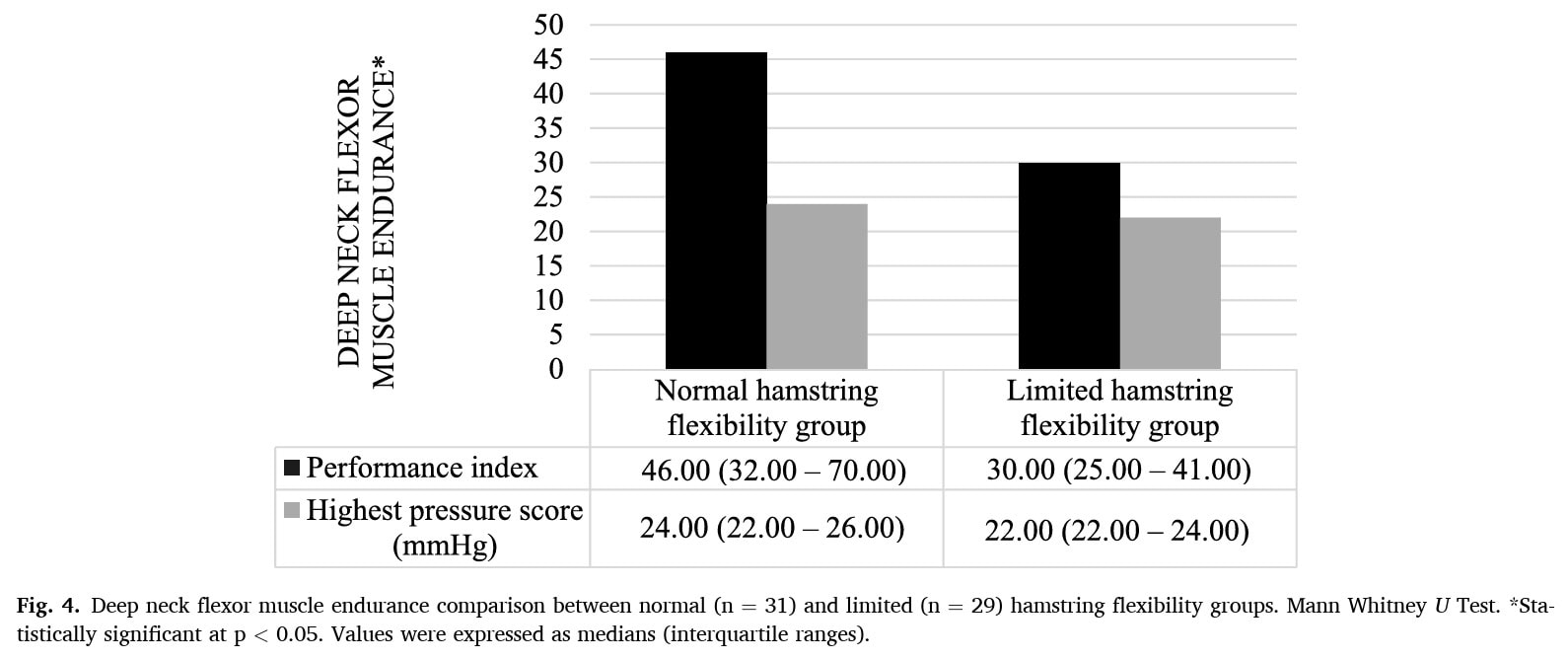
There was a significant difference between the CCFT endurance scores. The performance index achieved by the participants in the normal hamstring flexibility group was 46, compared to 30 in those with hamstring flexibility limitations.
Questions and thoughts
What immediately caught my eye was the presence of author bias. The aim of this study was to find a relationship between the deep cervical flexor muscles and the hamstrings via a myofascial network. The authors concluded that those with limited hamstring flexibility had worse performance on the CCFT. They conclude: “This study is the first to identify reduced deep neck flexor endurance in subjects with limited hamstring flexibility. Its preliminary clinical value supports the hypothesis of a myofascial network between the hamstring and deep neck flexor muscles”. Although the passive straight-leg raise test can give an indication of hamstring length, the lack of a structural differentiation maneuver in this study makes it impossible to assign a positive straight-leg raise test to reduced hamstring flexibility only. Neural tensioning may equally be causing deficits in the straight-leg raise performance but is of a totally different etiology. This was not even considered by the authors, and this altogether refrains me from supporting the conclusions.
When observing the participant’s characteristics, it stands out that in the normal hamstring flexibility group a 70-30 female-to-male ratio was included, compared to a 50-50 female-to-male ratio in the limited hamstring flexibility group. This may imply that the group classification based on normal flexibility could have been influenced by gender. Alam et al. 2023 found significant gender differences in the relation between trunk flexor flexibility (measuring the flexibility of the lower back and the hamstring muscles) and two different measures of hamstring flexibility (Active Knee Extension Test and passive straight-leg raise test). In females, there was a significant correlation between the tests, while this was not true in men, concluding that there are significant gender differences in the relationship between hamstring tightness and trunk flexion flexibility. In 2022, Miyazaki et al. confirmed that females have higher flexibility in the ovulatory and luteal phases of their menstrual cycle compared with during the follicular phase. Furthermore, Yu et al. in 2022 confirmed that hamstring stiffness was always worse in males than females in their study. This imbalance is potentially a limiting factor and may undermine the findings. Another relevant point to consider is that double the participants from the normal hamstring flexibility group had a Beighton score of 3, compared to participants in the limited hamstring flexibility group.
Talk nerdy to me
Two outcomes were studied: deep neck flexor endurance and active neck range of motion, but no primary outcome of interest was specified. Active ROM was not different between the groups. There appeared an influence of hamstring flexibility on CCFT performance. Despite two different outcomes being chosen, no correction for multiple comparisons was used (for example Bonferroni). The authors did not provide any table to look at the data. Still, they included figure 4 to show the performance of the participants in the CCFT test, categorized into those with normal and limited hamstring flexibility.
This dichotomization of the participant’s hamstring flexibility, being a continuous outcome into two categories: normal and limited hamstring flexibility leads to a loss of information and an increased risk of finding false positive findings. (Austin and Brunner, 2004)
Highest pressure score
Since the interquartile ranges completely overlap, no significant difference was seen, meaning that hamstring flexibility does not influence peak pressure scores.
Performance Index
The significant difference (p < 0.05) suggests a relationship between hamstring flexibility and neck flexor endurance, but without Bonferroni correction, the result should be interpreted cautiously. The difference between the groups is only moderate given the partial overlap of the interquartile ranges between the groups. As there was higher variation in performance index of the normal hamstring flexibility group, this gives an indication that some individuals had much higher endurance of the deep cervical flexors, and this could be driving the significance.
There was a difference in the performance index scores between the participants with and without limited hamstring flexibility. With a performance index of 46 in participants with normal hamstring flexibility, and a highest pressure score of 24, this indicates that they were able to perform 10 repetitions at the 4th level (4×10=40) and that they managed to do 1 repetition at the 6th level (6×1), totaling 40+6=46.
Meanwhile, in the participants with limited hamstring flexibility a performance index of 30 and a highest pressure score of 22 was observed. This indicates that they were able to perform 10 repetitions at the 2nd level (2×10=20) and 2,5 repetitions at the 4th level (since 4×2,5=10) and 20+10=30. Maybe this seems minor but no half-repetitions are possible in this test. Or, the performance index of 30 was calculated by performing 15 repetitions at the 2nd level, but the test had been described by Jull et al in 2008 that after 10 correct repetitions, progression to the next level is made. Hence it is unclear whether the authors used a correct calculation of the performance index in the participants with limited hamstring flexibility.
As this was a cross-sectional study, there was only 1 measurement at 1 specific time. Therefore, this comparison only reflects one particular moment in time. Moreover, cross-sectional designs are not able to capture cause-effect relationships (Wang et al. 2020), for which longitudinal studies are required. There might be bias in the results, and also the timing of the outcome measurement collections can have influence on the present findings. For example, as this study was conducted in healthy university students, the timing of their assessment (before versus after classes/internships) can influence the obtained results. Furthermore, since the order of the assessments was always the same, with the deep neck flexor endurance (which is already difficult for many healthy people) always being the last assessment, this could also have influenced the findings. An important part to consider as well is the use of five different assessors, although they were blinded, for only 3 measurements. This can create inconsistency in the findings.
Take-home messages
The study suggests a potential link between limited hamstring flexibility and reduced deep neck flexor endurance, still, causality is not proven, given the impotence of cross-sectional studies in proving causality. Since multiple comparisons were made, the alpha level p < 0.05 may not be enough to claim a true effect. Future studies should use Bonferroni corrections and longitudinal or experimental designs to confirm these findings. Confounding factors (for instance gender) may help explain the observed differences. Thus, no influence of hamstring flexibility on CCFT can yet be demonstrated.
Reference
DISCOVER FASCIA FROM ITS HISTORY TO ITS VARIOUS FUNCTIONS
Enjoy this free 3x 10min Video Series with Renowned Anatomist Karl Jacobs who will take you on a trip into the world of Fascia
