
Research
Exercise
November 20, 2023
How to make gluteal muscle strengthening progressions?

Introduction
Progressing loads to rehabilitate injuries is paramount to increase strength and tolerance. The main force producers for the hip are the gluteal muscles. Therefore, exercises are mainly hip-focused and aim to target the gluteus medius, minimus, and maximus. Often, people will have weakness in one or more gluteal muscles, and this may impede proprioception, propulsion, and balance. On the other hand, good gluteal muscle functioning is associated with good outcomes. Strength increases develop gradually when sufficient loads are applied, therefore bodyweight exercises can be progressed with increasing loads. But which exercise is more demanding and what exercise you can use best to start off with? That is what this study examined: how to make gluteal muscle strengthening progressions through analysis of muscle activity during eight hip-focused exercises.
Methods
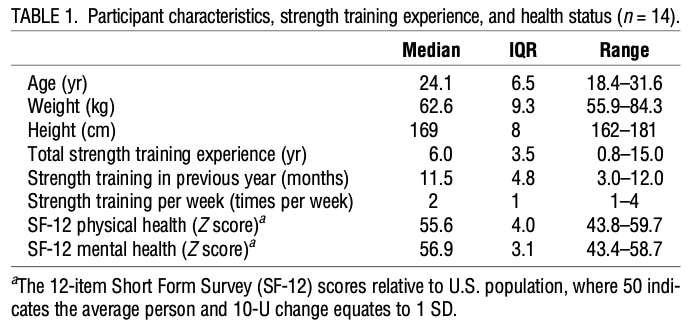
This cross-sectional study used a within-participant design to study the force production among different hip exercises. Fourteen female rugby players were recruited who were used to some form of strength training in the past three months and remained spared from injuries to the lower limbs. Further, they had no history of lower limb surgery.
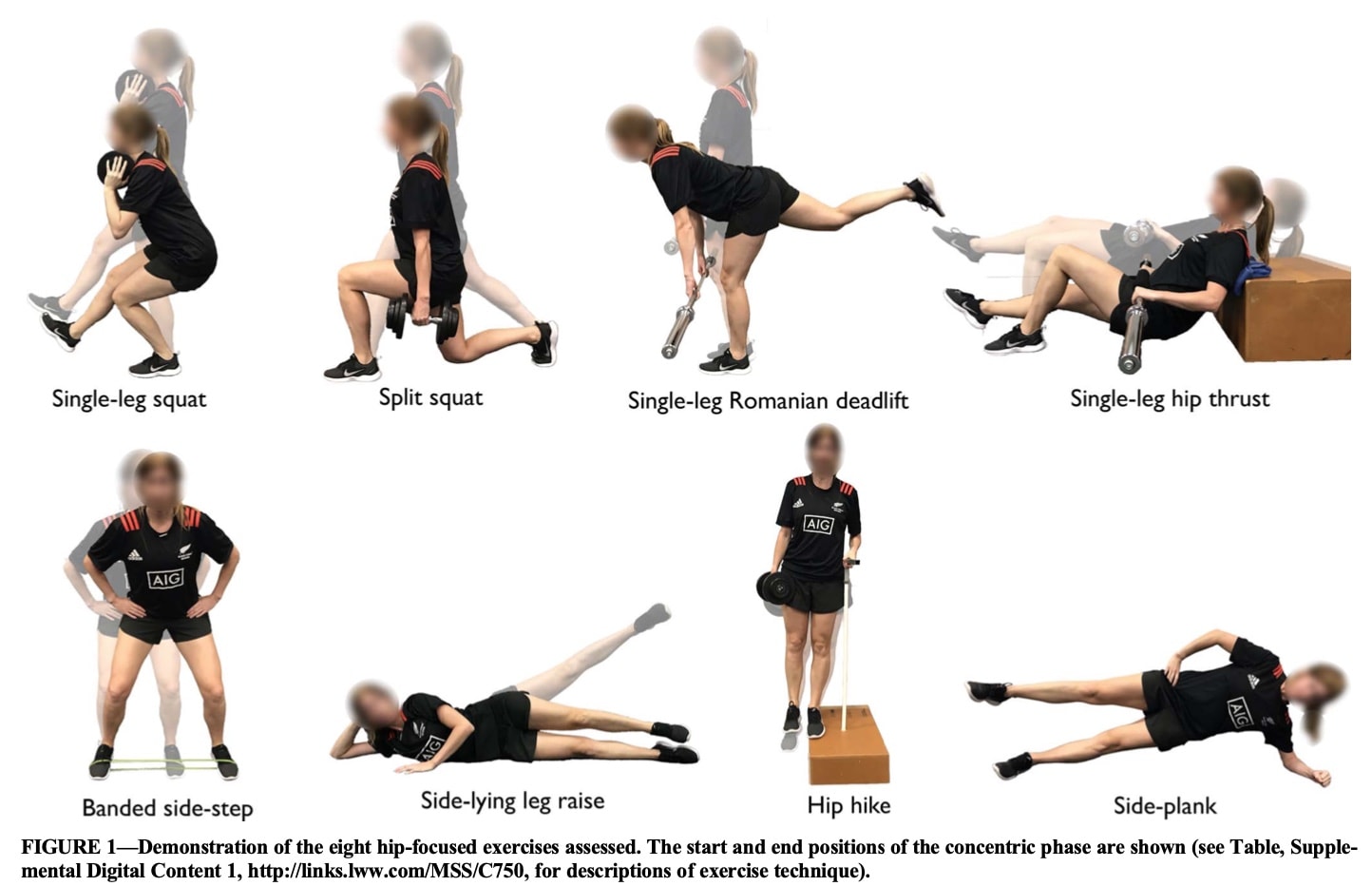
A total of eight hip exercises were studied per participant and repeated approximately one week later. The first week, the exercises were performed with the use of external resistance, and the other week, they were accomplished without. The session started with a familiarization to the exercises and thereafter, biomechanical data were collected. The eight exercises performed were:
- single-leg squat,
- split squat,
- single-leg Romanian deadlift (RDL),
- single-leg hip thrust,
- banded side step,
- hip hike,
- side plank,
- side-lying leg raise
In the exercise familiarization period, the 12-repetition maximum was determined using a ramp testing protocol to determine a relative intensity load for each exercise. Every exercise was done and in case 12 repetitions could be performed, weight was added by approximately 1.25–2.5 kg increments for dumbbell and barbell exercises after a 1–2 min rest period. The final resistance was determined when 12 repetitions could not be performed or strict technique could not be maintained.
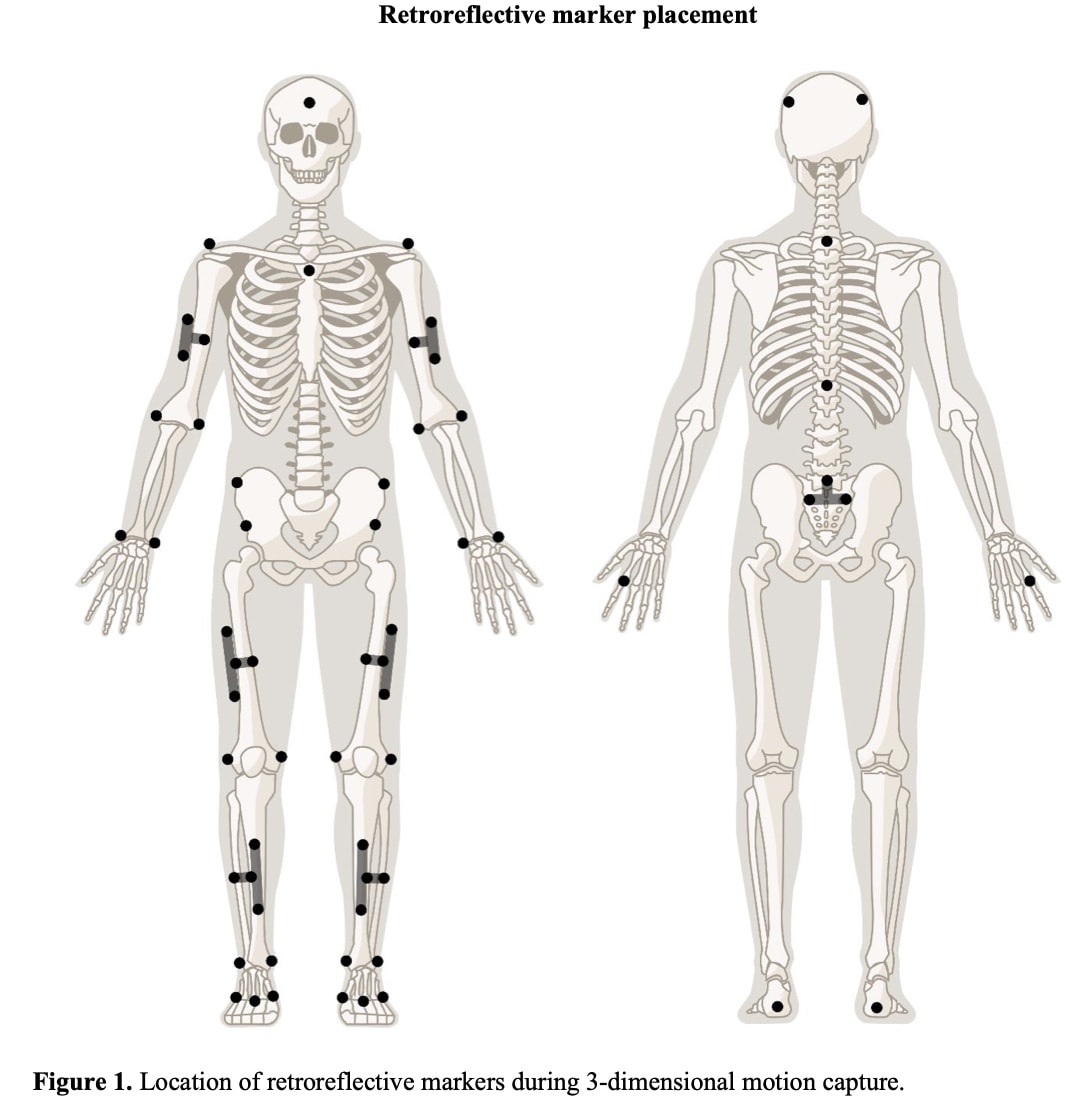
Next, reflective markers were attached to the participant’s legs, arms, and torso. The ground reaction forces were measured using two force plates. Muscle activation was measured using surface EMG of the following muscles:
- anterior gluteus medius,
- upper gluteus Maximus,
- tensor fascia lata,
- rectus femoris,
- vastus lateralis,
- vastus medialis,
- semitendinosus,
- biceps femoris long head,
- tibialis anterior,
- gastrocnemius medial,
- gastrocnemius lateral,
- soleus.
The EMG signal was normalized by performing maximal voluntary isometric contractions of the following movements:
- seated knee extension (70° knee flexion),
- prone knee flexion (30° knee flexion),
- supine dorsiflexion,
- prone plantar flexion,
- seated plantar flexion,
- supine straight-leg hip abduction
- standing glute squeeze.
To begin the testing protocol two sets of five body weight-only repetitions were performed and followed by two sets of five loaded repetitions (12RM). Between the sets, a 30-60-second rest period was held.
Finally, a musculoskeletal model was constructed.
Results
The mean loads applied to obtain the 12RM for these participants were:
- 18.0 ± 2.0 kg for hip hike,
- 4.6 ± 1.1 kg for side-lying leg raise,
- 8.2 ± 6.0 kg for single-leg hip thrust,
- 19.3 ± 6.1 kg for single-leg RDL,
- 13.6 ± 3.3 kg for single-leg squat,
- 30.0 ± 6.2 kg for split squat.
- For the banded side step, 12 of 14 participants used a moderate stiffness band, and 2 of 14 participants used a high stiffness band.
The exercises with the highest peak gluteus maximus muscle force were the loaded split squat (95% CI = 495–688 N), loaded single-leg RDL (95% CI = 500–655 N), and loaded single-leg hip thrust (95% CI = 505–640 N).
The exercises with the highest peak gluteus medius muscle force were body weight side plank (95% CI = 338–483 N), loaded single-leg squat (95% CI = 278–422 N), and loaded single-leg RDL (95% CI = 283–405 N)
The exercises with the highest peak gluteus minimus muscle force were single-leg RDL (95% CI = 267–389 N) and body weight side plank (95% CI = 272–382 N)
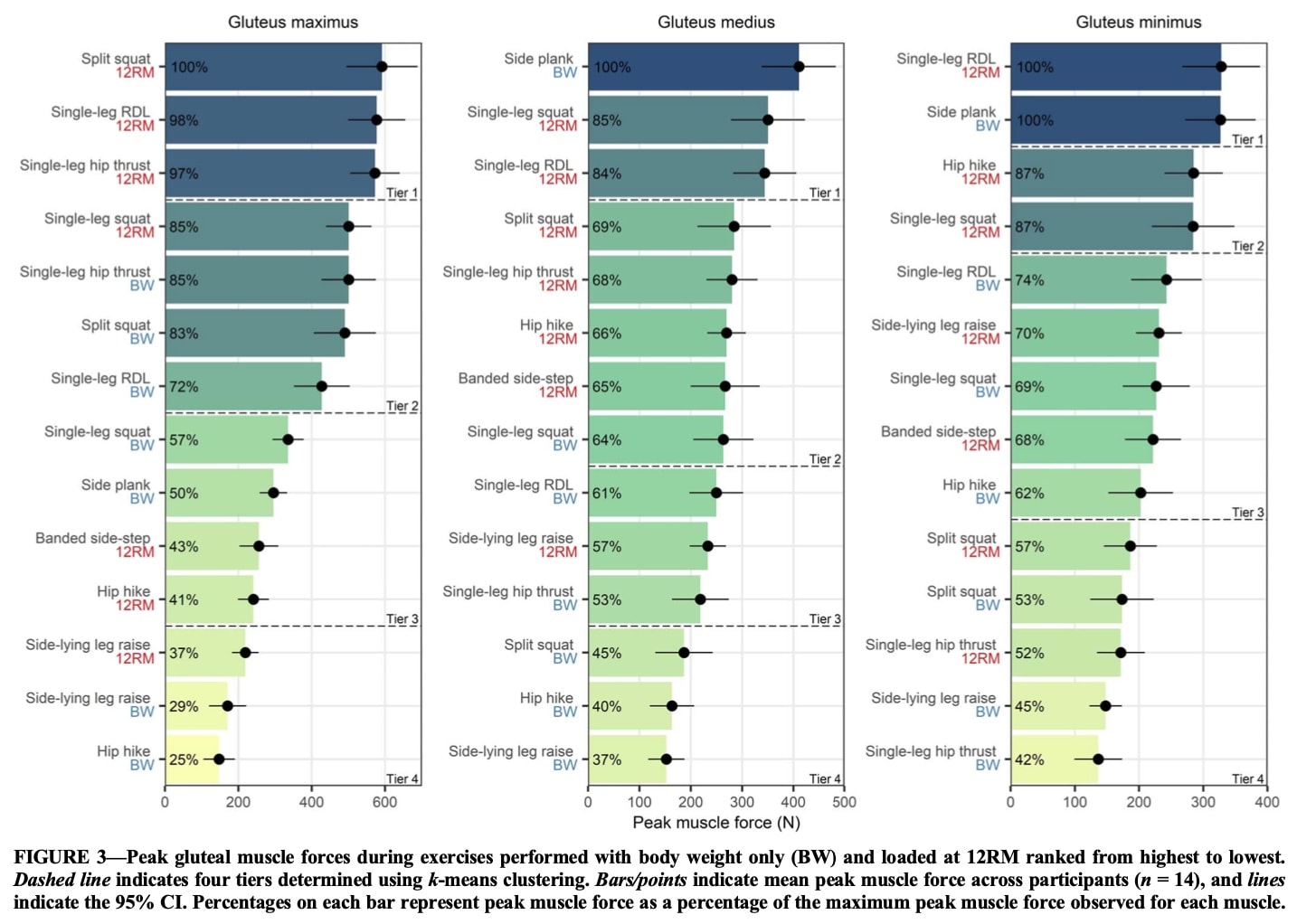
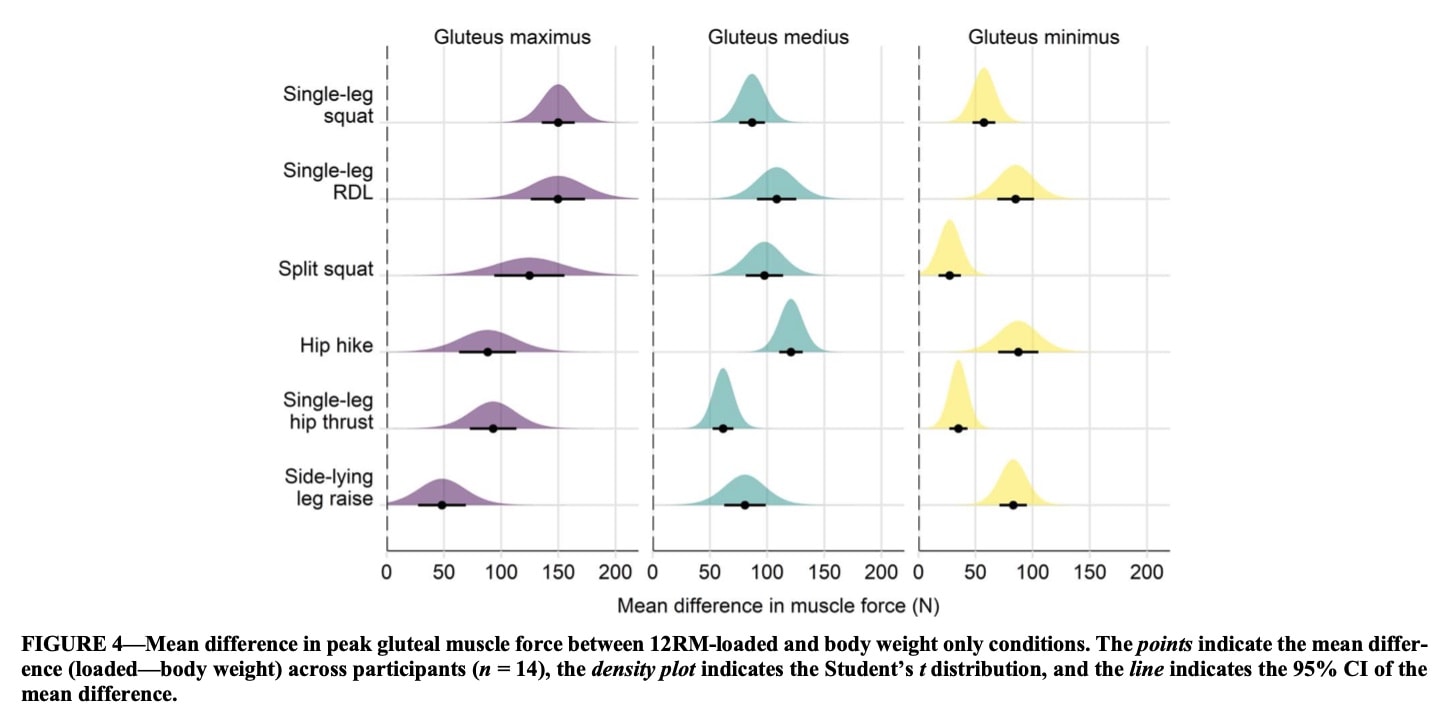
When the loads were increased so that the exercises were performed at a 12RM intensity, the peak forces in the gluteal muscles increased significantly. So adding loads would be suitable for making gluteal muscle strengthening progressions. Figure 4 displays the mean added forces on the hip when the 12RM loads are added.
Questions and thoughts
In 2020 Moore et al. also conducted an EMG study on this topic, which we reviewed back then. They used a definition of low, moderate, and high muscle activation when the EMG was between 0-20% of the MVIC, 21-40% MVIC or 41-60% of the MVIC, respectively. Although not the same exercises were studied here, a comparison of these results suggests that indeed side-lying hip abduction can be seen as an exercise creating a moderate activation of the gluteus medius and the hip hike creates a high gluteus medius activation. In contrast, a single-leg squat was reported by Moore to demand a moderate muscle activation of the gluteus medius, but this study showed a rather high demand with 61% of the MVIC. The same was true for the split squat, however, in Moore’s study, it was more of a forward lunge, so this can be the reason for the difference.
The systematic review by Ebert et al. in 2017 largely confirms the findings of this study. They found that indeed the side plank generated a very high gluteus medius activation. Hip hikes and single-leg RDL respectively caused moderate to high and high levels of gluteus medius activation.
What was interesting about this study was that it ranked the exercises per gluteal muscle group into four tiers. This can be used to adapt the exercises for making gluteal muscle strengthening progressions or regressions. Interestingly, the tier 1-loaded exercises produced greater peak gluteus maximus muscle force (3.3–3.6 times body weight) than a maximal effort sprint acceleration that produces an average of 1.9–3.3 times body weight.
Hip extension–dominant movements (split squat, single-leg squat, RDL, and hip thrust) created similar muscle forces in the gluteus medius and minimus compared to hip abduction movements (hip hike, banded side step, side-lying leg raise). Thus when you want to target the lateral stabilizers of the hip, you can use more functional hip-extension dominant exercises.
The results indicate that for many exercises, the gluteus minimus produced more force compared to the gluteus medius, when the force production was normalized to the muscle size, particularly for hip hikes, side-lying leg raises, and side planks. As the gluteus minimus is more of a hip stabilizer by helping the capsule hold the femoral head in the acetabulum, you can use these exercises to increase local hip stabilization.
Talk nerdy to me
By using a within-participant cross-sectional design, the study could use a control situation (no external resistance) to compare against the loaded situation.
Interesting to see was the use of relatively high loads, for example, 18kg was applied to increase the intensity of the hip hike to 12RM. Yet, this study included uninjured participants who may tolerate much more loading.
Subjects with gym experience and playing rugby were included and this may not be generalizable to people suffering from hip pathology or injury. The same is true for sex as all players in this study were female.
Surface EMG data were obtained, which may be subject to movement artifacts and cannot exclude crosstalk signals from other muscles. Yet being a non-invasive study method, it can more closely resemble clinical practice. Another limitation is that a musculoskeletal model was used, which is a simplification of the real anatomy. However, despite being a simplification, these models are constructed and based on data from medical imaging and cadaveric studies and may therefore be an interesting way to visualize what (may) be going on in our bodies during real-time movements.
Take home messages
This study compared eight different hip exercises to create a progressive rank of loads omitted to the gluteal muscles. As such, this info can be used to make gluteal muscle strengthening progressions as the ranked exercises may help you to increase or decrease the demands. This study was however done using healthy participants without lower limb injuries and may therefore not be generalized to an injured population directly.
Reference
Additional References
LEVEL UP YOUR DIFFERENTIAL DIAGNOSIS IN RUNNING RELATED HIP PAIN - FOR FREE!
Don’t run the risk of missing out on potential red flags or ending up treating runners based on a wrong diagnosis! This webinar will prevent you to commit the same mistakes many therapists fall victim to!
