
Research
Diagnosis & Imaging
April 16, 2026
Persistent Low Back Pain Not Responding to Treatment? Screening Flags Suggesting Endometriosis in LBP Identified via a Delphi Study

Introduction
Endometriosis is a condition in which endometrial-like tissue grows outside the uterus and is associated with symptoms such as pelvic pain, infertility, dysmenorrhea, and dyspareunia. While imaging techniques such as MRI and ultrasound are commonly used, laparoscopy remains the gold standard for diagnosis, as lesions may not always be detected on imaging. Diagnosis is often delayed, typically taking 5 to 8 years, which can lead to suboptimal patient outcomes.
Patients with endometriosis may also present with non-specific low back pain (LBP), leading to potential overlap between the two conditions. Physiotherapists should be aware of these similarities and recognize flags suggesting endometriosis in LBP to support appropriate management and help reduce diagnostic delay.
Methods
Research on the relationship between low back pain and endometriosis is limited. Delphi studies provide a method to gather and compare evidence, and reach consensus among expert opinions in areas where evidence is scarce.
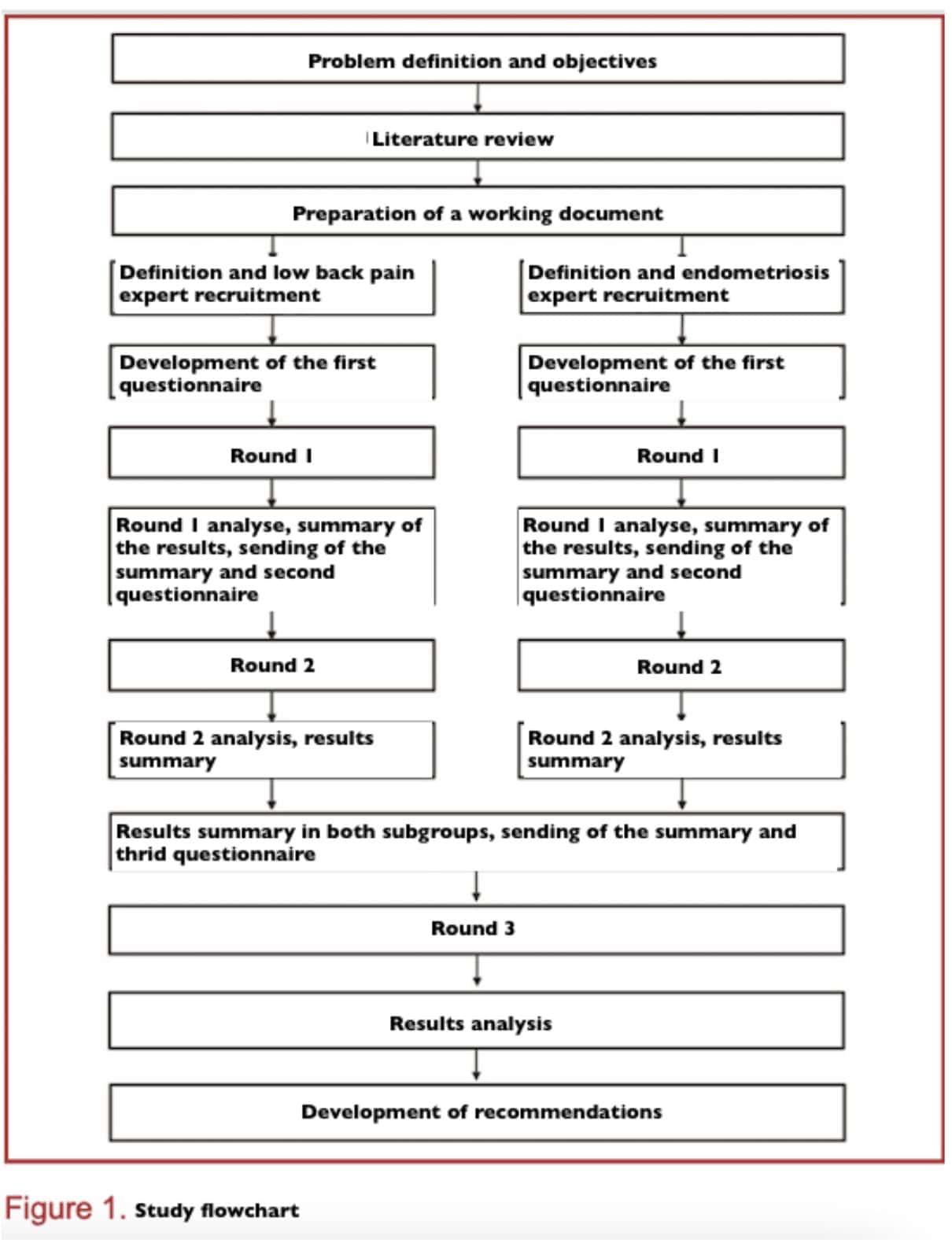
The study included three rounds of questionnaires (Fig. 1). The first two rounds were completed by two separate groups of experts, one specializing in endometriosis and the other in low back pain. In the third round, both groups were combined to reach a final agreement. A summary of the literature was provided with the first questionnaire, and summaries of the previous rounds were shared with each new round. The study was planned to include three rounds.
The study author prepared a shared document encompassing the objectives, methodology, a summary of knowledge regarding endometriosis and low back pain, and the established link between these two conditions. The compilation of this shared documentation involved a preceding scientific literature review.
Expert selection
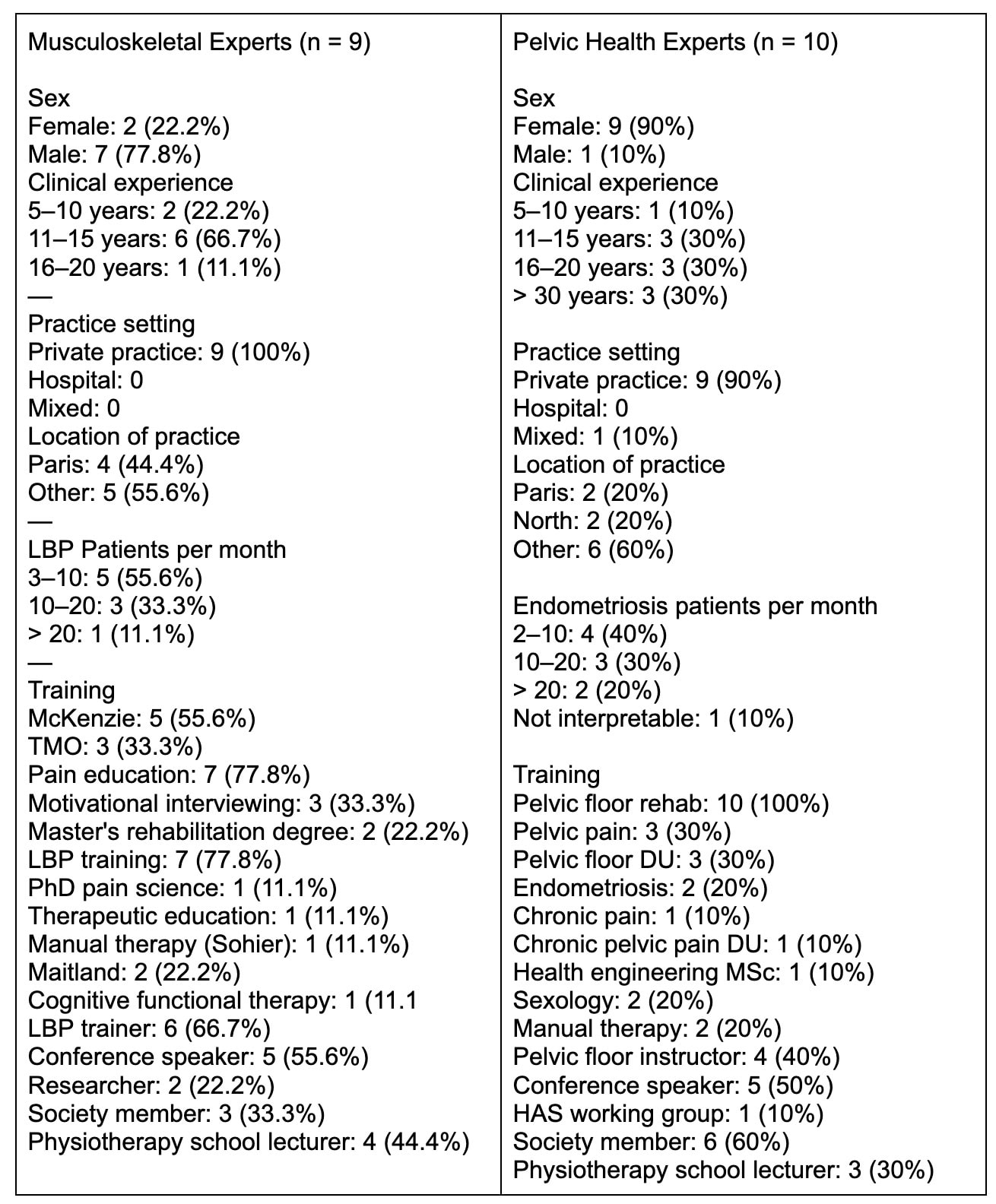
Experts in endometriosis (pelvic floor physiotherapists) and experts in low back pain (musculoskeletal physiotherapists, MSK group) were recruited based on inclusion criteria into two separate subgroups, each including at least nine experts. This number was chosen in line with the minimum number of participants recommended for Formalized Consensus Guidelines (RCF) by the French National Authority for Health (HAS).
First round
The first round included 3 sections:
- Participants’ characteristics and their expert status;
- Open-ended questions about clinical flags suggesting endometriosis in LBP patients. No items were provided to participants. They were asked to propose at least three elements for each step of clinical reasoning (history taking, clinical examination, and reassessment), and to rate their clinical importance (low, moderate, or high). Clinical importance was defined as follows:
- Low: slightly increases the likelihood of endometriosis and must be combined with other elements.
- Moderate: moderately increases the likelihood and should be combined with at least one other element.
- High: strongly increases the likelihood and is sufficient on its own to suspect endometriosis.
- Statements regarding patient referral, rated on a 7-point Likert scale.
Second round
The second round was conducted separately within each subgroup. It aimed to reach consensus on the items proposed in round one, to assess expert agreement on items that had reached near-consensus, and to evaluate new items resulting from reformulations suggested in the first round.
Third round
The objective of the third round was to reach a consensus between the two subgroups. The questionnaire, therefore, included items that had been accepted or remained uncertain in both subgroups during the first two rounds, as well as items derived from reformulations and comments.
Analysis criteria
Round 1
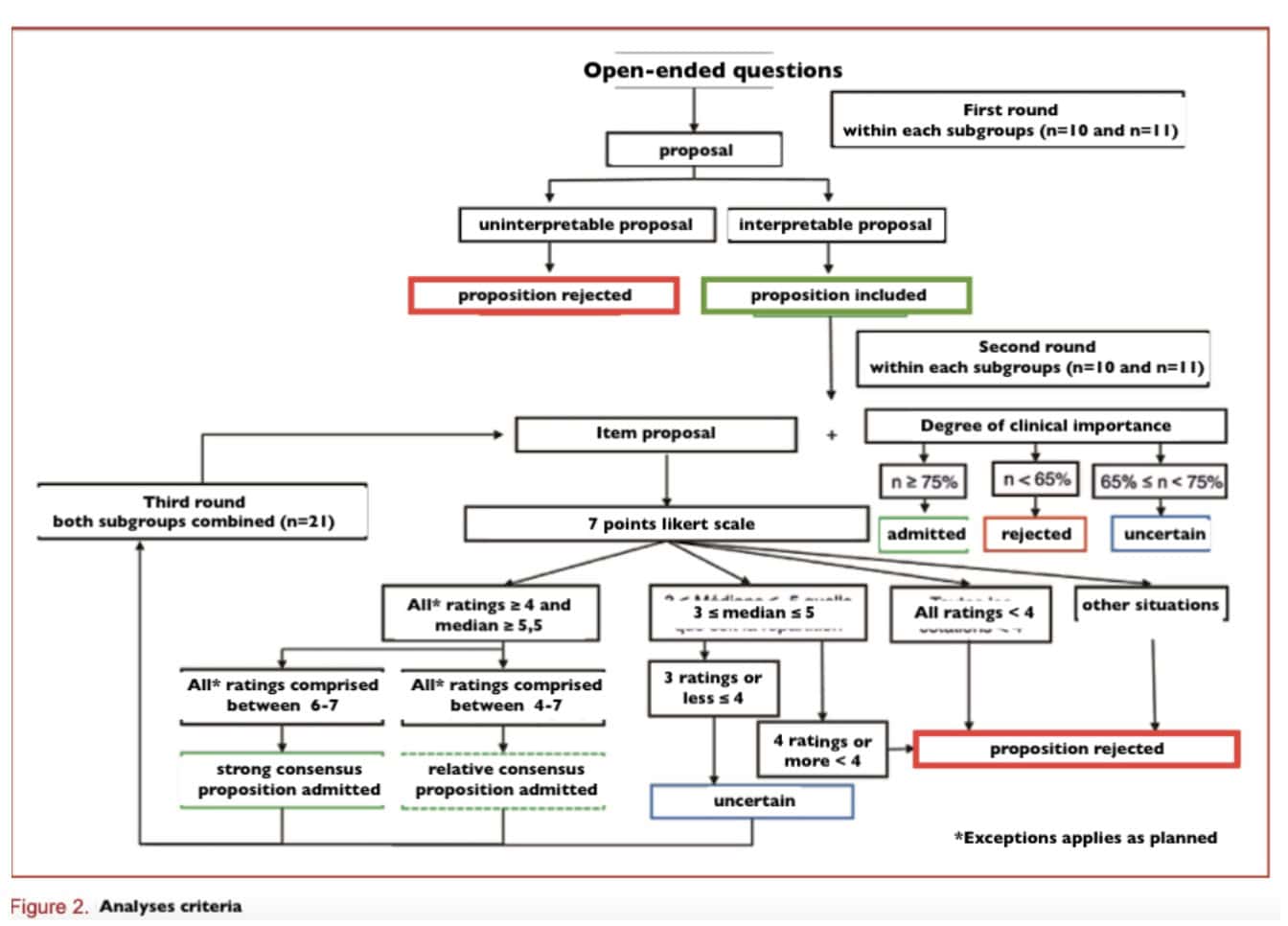
All proposed items were retained for the second round. They were grouped into a table and ranked according to how frequently they were suggested. This table was sent to the experts along with the second questionnaire. Non-interpretable or inappropriate responses were excluded. Items related to patient referral, assessed using a Likert scale, were analyzed according to the criteria defined for rounds 2 and 3.
Rounds 2 and 3
Experts rated each item using a 7-point Likert scale (1 to 7). Agreement was defined when all ratings were either ≤ 4 or ≥ 4. All other distributions were considered in disagreement.
Each item was classified as follows:
- Strong agreement (accepted): Median ≥ 6, agreement among experts, and all ratings within [6–7]
- Relative agreement (accepted): Median ≥ 5, agreement among experts, and all ratings within [4–7] OR all ratings within [4–7] except one
- Uncertain: Median between 4 and 7, with at most three experts rating ≤ 4
- Rejected: All other situations
Special cases (to limit the impact of outliers)
- If the median was > 5.5 and all ratings were within [6–7] except one (round 2) or two (round 3) lower ratings (< 7), the item was considered appropriate with strong agreement
- If all ratings were within [4–7] except one (round 2) or two (round 3) ratings < 4, the item was considered appropriate with relative agreement
Additional criterion
The consensus threshold for levels of clinical importance was set at 75%.
Results
Participation
In the MSK subgroup, 9/10 experts (90%) responded to round 1, and 7 (70%) to rounds 2 and 3. In the PP subgroup, 10/11 (90.9%) responded to rounds 1 and 2, and 7 (63.6%) to round 3. All experts had completed post-graduate training in endometriosis or low back pain. About half were educators or had given lectures, 47% were members of scientific societies, 37% taught in physiotherapy schools, and three had contributed to publications.
Rounds outcomes
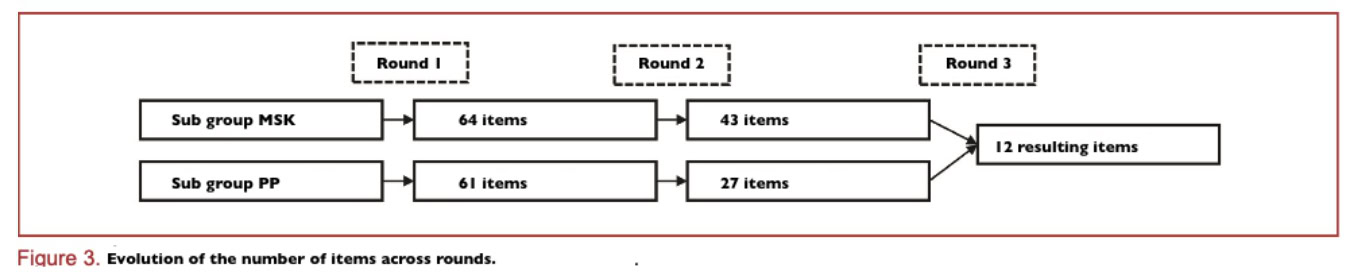
Round 1 generated 64 items (MSK) and 61 (PP). After round 2, 43 items (MSK) and 27 items (PP) progressed to round 3.
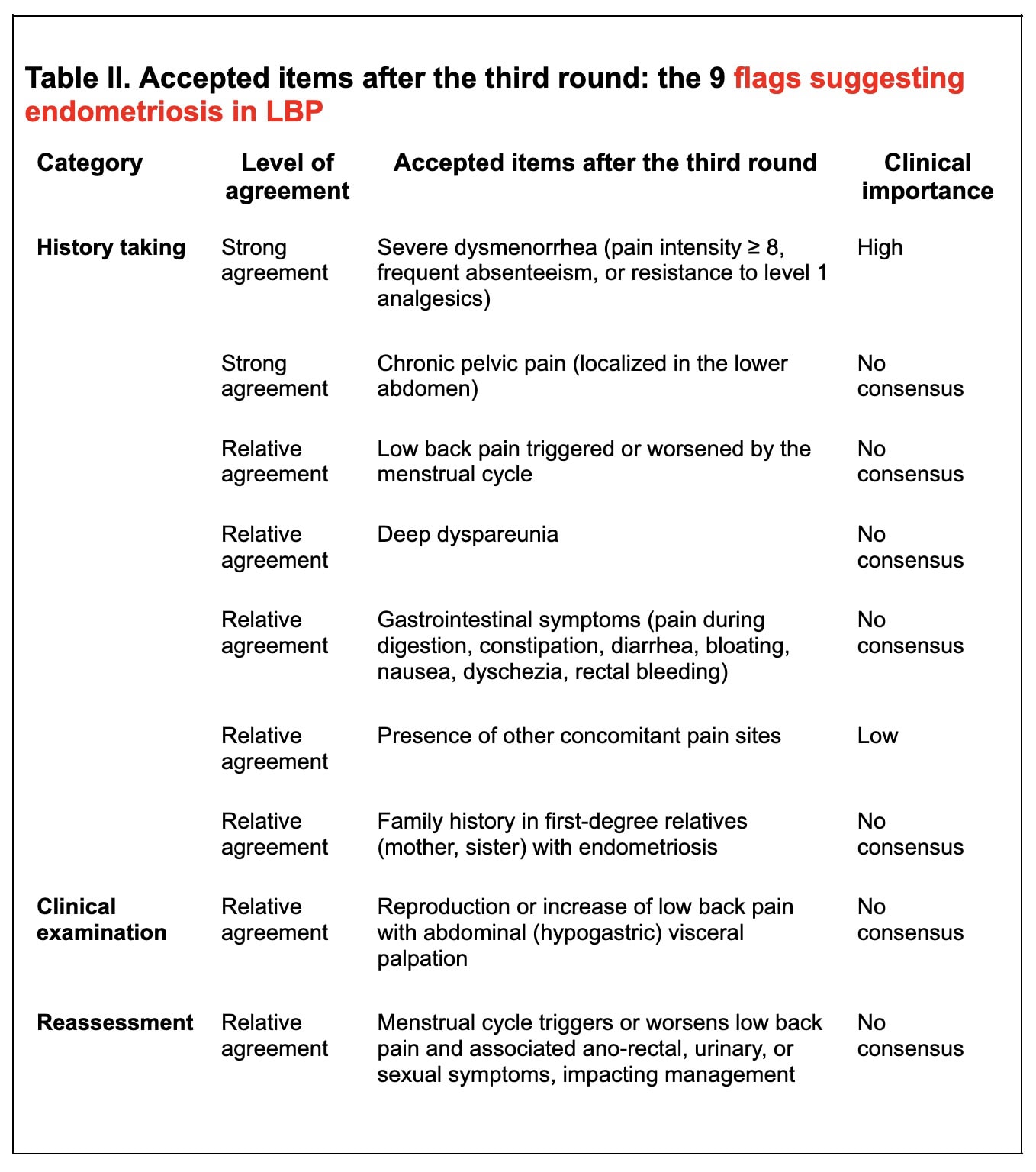
In round 3, 12 items were accepted (9 clinical flags suggesting endometriosis in LBP and 3 referral recommendations).
Referral consensus included:
- Informing patients about suspected endometriosis and suggesting discussion with a physician (strong agreement)
- Referring to a general practitioner with a written summary and continuing physiotherapy care (relative agreement)
Rounds analysis
Results were stable between rounds 2 and 3 (no significant changes).
Most final items (82%) were proposed by both groups initially; 18% came only from the MSK group.
Differences between groups:
- PP experts were more selective for history-taking items
- MSK experts were more selective for clinical examination items
- Less disagreement for reassessment and referral items
Questions and thoughts
Regarding pelvic pain, only history-related items concerning pelvic health and digestive symptoms reached consensus. Intense dysmenorrhea was the only symptom that reached consensus as a flag suggesting endometriosis in LBP, prompting patient referral. Concerning low back pain, only the presence of cyclical pain reached consensus. However, the other history elements mentioned above may still be clinically relevant and are easy to incorporate into the assessment of patients with low back pain.
These findings are consistent with the existing literature. A narrative review highlights that menstrual-related symptoms are key indicators and should prompt referral. Digestive symptoms and potential genetic factors are also supported in the literature, alongside well-established symptoms such as dysmenorrhea, chronic pelvic pain, dyspareunia, and infertility.
Although no single clear mechanism explains the association between endometriosis and low back pain, several hypotheses exist. One possible explanation is referred pain from the pelvis to the lumbosacral region. In addition, central sensitization—commonly observed in patients with endometriosis—may further contribute to the presence of low back pain.
Interestingly, a case report described endometrial tissue located on the L3 vertebral body in a 33-year-old patient presenting with cyclical recurrent low back pain, confirmed by MRI and surgical biopsy.
Talk nerdy to me
This study originates from a master’s thesis and therefore has inherent limitations. It was conducted by a single researcher, which may have restricted the scope of the work. As acknowledged by the author, this could also have introduced confirmation bias, with the possibility that some questions were oriented and open to subjective interpretation.
Despite these limitations, the study provides a valuable foundation for identifying clinical features suggestive of endometriosis in patients presenting with low back pain. However, the inclusion of only French physiotherapists may limit the generalizability of the findings. Future Delphi studies involving a broader and more diverse panel of experts from diverse regions and backgrounds—including gynecologists, midwives, and other relevant healthcare professionals—could offer more comprehensive insights and allow for a more exhaustive identification of overlapping features between these conditions.
Methodologically, the use of structured questions may have introduced bias. Incorporating open-ended responses alongside qualitative methods, such as thematic analysis, could allow for a more in-depth exploration of the relationship between low back pain and endometriosis. Additionally, further validation studies are needed to assess the sensitivity and specificity of the identified clinical features.
Take-home messages
Key flags suggesting endometriosis in LBP
- Severe dysmenorrhea (severe pain, absenteeism from school/work, or resistance to first-line analgesics) – strongest consensus for referral.
- Low back pain influenced by the menstrual cycle – a cyclical pattern may indicate endometriosis.
- Deep dyspareunia (pain during sexual intercourse).
- Chronic pelvic pain localized in the lower abdomen.
- Gastrointestinal symptoms such as bloating, constipation, diarrhea, nausea, or pain during digestion.
- Family history in first-degree relatives (mother, sister) with endometriosis.
- Other concomitant pain sites – may increase suspicion, but are less specific.
Flags from clinical examination
- Reproduction or increase of low back pain with abdominal (hypogastric) visceral palpation – may suggest visceral contribution.
Reassessment considerations
- Monitor whether menstrual cycle triggers or worsens low back pain, particularly if associated with ano-rectal, urinary, or sexual symptoms.
Clinical integration
- Include menstrual and pelvic symptom screening in low back pain assessments, even when patients present with apparently musculoskeletal pain.
- Be aware that referred pain from the pelvis and central sensitization may contribute to low back pain in endometriosis.
Limitations to keep in mind
- Most evidence is based on expert consensus among French physiotherapists; findings may not generalize globally.
- High-quality research is needed to investigate in greater detail the link between low back pain and endometriosis.
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Watch this FREE video lecture on Nutrition & Central Sensitisation by Europe’s #1 chronic pain researcher Jo Nijs. Which food patients should avoid will probably surprise you!
