Research
Exercise
March 6, 2023
Effects of adding exercise to usual care in hypertension, diabetes or cardiovascular disease

Introduction
Exercise has been shown to have many benefits. Not only does physical activity help prevent diseases and related comorbidities. It can also play an important role in the secondary and tertiary prevention of various health conditions. Recently, we published a blog about exercise in people with osteoporosis. In the same light, here we present a study that attempts to answer the question of whether exercise is beneficial or harmful in people already known to have various health conditions. What can we conclude? Can adding exercise to usual care improve the outcomes in people with hypertension, diabetes, and cardiovascular disease?
Methods
To know if you need to get people with hypertension, type 2 diabetes, and cardiovascular disorders moving, we need to know first if there is an additional benefit of exercising compared to usual care for these conditions. Therefore, this systematic review was conducted.
To answer this research question, randomized controlled trials assessing the effects of adding exercise to usual care were included and compared to usual care alone. The participants had a known diagnosis of either hypertension, type 2 diabetes, or cardiovascular disease. The primary outcomes of interest were all-cause mortality, serious adverse events, and quality of life.
Results
The search yielded 248 articles studying 21,633 participants. The study sample was mainly constructed of people with a diagnosis of cardiovascular disease (76.2%). Type 2 diabetes and hypertension formed the minority of the sample with 16.5% and 6.5% included, respectively. Half of the included studies investigated the effects of dynamic aerobic exercise. Ten percent of the studies investigated the effects of dynamic resistance training and nearly a quarter studied combined forms of exercise. The median intervention period was 3 months and follow-up mainly was 6 months.
The primary outcome of all-cause mortality was investigated in 98 trials including 12 976 participants. In the experimental group, 6.5% died, compared to 8.3% in the usual care group. Adding exercise to usual care resulted in a risk ratio of 0.82, meaning a beneficial risk reduction of 18% of early death.
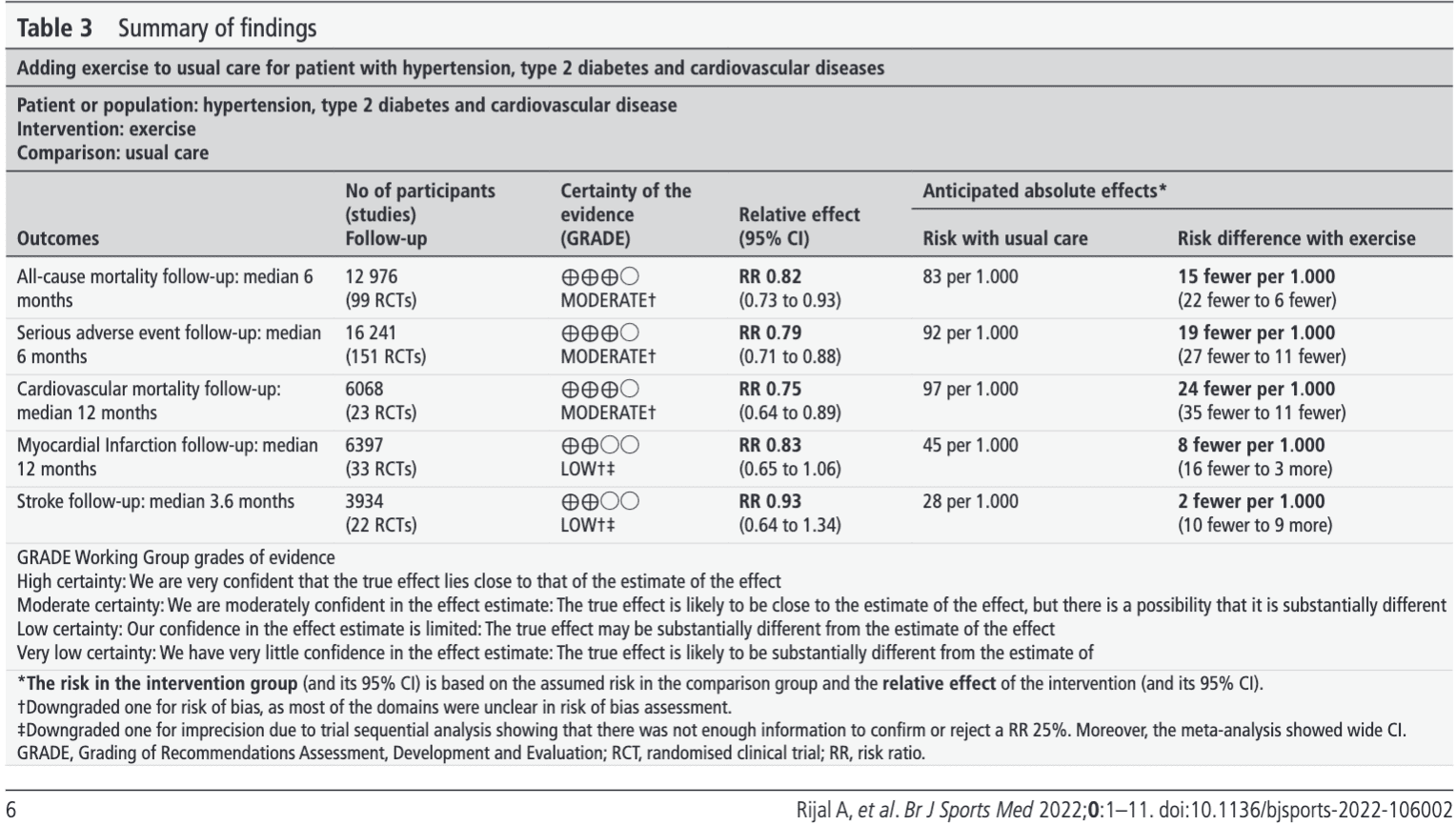
Considering the outcome of reported serious adverse events, 150 trials were included with 16 241 participants. Here 6.8% of the participants doing exercise reported a serious adverse event compared to 9.2% in the usual care groups. This resulted in a risk ratio of 0.79 when adding exercise to usual care, meaning that participants in the exercise group reported 21% fewer serious adverse events.
Quality of life was studied in 96 trials including 7676 participants. There were 7 different scales used to define the quality of life. Adding exercise to usual care improved quality of life when assessing 4 of the 7 scales. These scales were the SF36 Mental and Physical components, the Barthel Index of Activity of Daily Living, and the Minnesota Living with Heart Failure Questionnaire. On these scales, exercise showed a significant increase in quality of life but only the Barthel Index exceeded the predefined clinically important difference.
Questions and thoughts
Secondary outcomes were cardiovascular mortality, myocardial infarction, and stroke. These form 3 potential barriers to exercise as people are often scared to worsen their health condition through exercise. The review concluded a significant risk ratio of 0.75 for cardiovascular mortality, meaning that those participating in exercise had a risk reduction of 25% compared to the usual care participants. The other 2 secondary outcomes failed to reach significance.
The intervention period was relatively short. This was of a median duration of 3 months. Furthermore, the volume of the exercise intervention was low. It had a median duration of 135 minutes per week. This is an excellent finding that may help motivate your patients: they don’t have to complete years of training before benefiting from the intervention. After only 3 months of completing 135 minutes of exercise training per week, there is already an important risk reduction.
The authors even mentioned that this risk reduction is as high as the effect sizes observed with pharmacological interventions to reduce systolic blood pressure with 10 mm Hg. It is indeed easier to take a pill every day, yet, these medications have a lot more side effects than exercise…
Talk nerdy to me
As a side note, we have to mention that the findings of the review were supported by moderate evidence. The risk of bias was high for all-cause mortality, serious adverse events, and cardiovascular mortality. Mainly, this was due to the lack of blinding of participants (which is hard in exercise trials), and inadequate reporting of randomization, allocation concealment, and loss to follow-up. This doesn’t mean that the trials did poorly on these aspects, rather they received this score because it was not reported and thus, the systematic review was not able to rate the extent to which it was performed correctly. Yet, in all three outcomes, heterogeneity was low (0%). Importantly, the majority of trials studied dynamic forms of aerobic exercise and thus, the evidence will most likely be skewed towards these forms of training.
Take home messages
Adding relatively short periods of exercise training to usual care for approximately 2 hours per week results in a decreased risk of serious adverse events and death, compared to usual care alone in people with known hypertension, type 2 diabetes or cardiovascular disease. In this study, the most studied type of exercise was aerobic, followed by a combination of aerobic and strength training. Exercise is therefore safe in this population and adding exercise to usual care may lead to improved care of people with these known conditions.
Reference
100% FREE POSTER PACKAGE
Receive 6 High-Resolution Posters summarising important topics in sports recovery to display in your clinic/gym.