
Research
Knee
April 10, 2023
Does early ACL reconstruction protect the meniscus?

Introduction
More and more evidence suggests that conservative management of a torn ACL is as effective as early ACL reconstruction. For many years, ACL reconstruction was seen as an essential step in the recovery of athletes. Today, more and more studies point to the natural healing capacity of the torn ACL. The recent secondary analysis from the KANON trial even indicates better clinical outcomes after conservative management in healed ACLs. Others postulate that a torn ACL causes ongoing instability in the knee, which may predispose the meniscus to tear. Tearing of the meniscus is undesirable as the risk of later-life osteoarthritis of the knee increases. Therefore, his study sought to answer whether early ACL reconstruction protects the meniscus from new tears.
Methods
The COMPARE trial data was used to determine whether or not early ACL reconstruction protects the meniscus from new tears. In this large COMPARE trial patients aged 18 to 65 with an acute rupture of the ACL were included. They were randomized to either early ACL reconstruction or rehabilitation followed by optional delayed ACL reconstruction after a three-month period of primary non-operative treatment. The results of this RCT found that those who underwent early surgical reconstruction had improved perceptions of symptoms, knee function, and ability to participate in sports at the two-year follow-up. But the authors stressed that the clinical importance of this finding was rather unclear as half of the patients randomized to the rehabilitation group did not need surgical reconstruction.
This secondary analysis was interested in whether or not people with early ACL reconstruction had reduced risk for later meniscus reconstruction. This was used as a proxy to determine the risk of new meniscus injuries.
So let’s COMPARE what results were found.
Results
A total of 167 people with a torn ACL were included. Eighty-five of them underwent early ACL reconstruction, while 82 were managed conservatively and could opt for delayed reconstruction. Baseline characteristics show comparable groups.
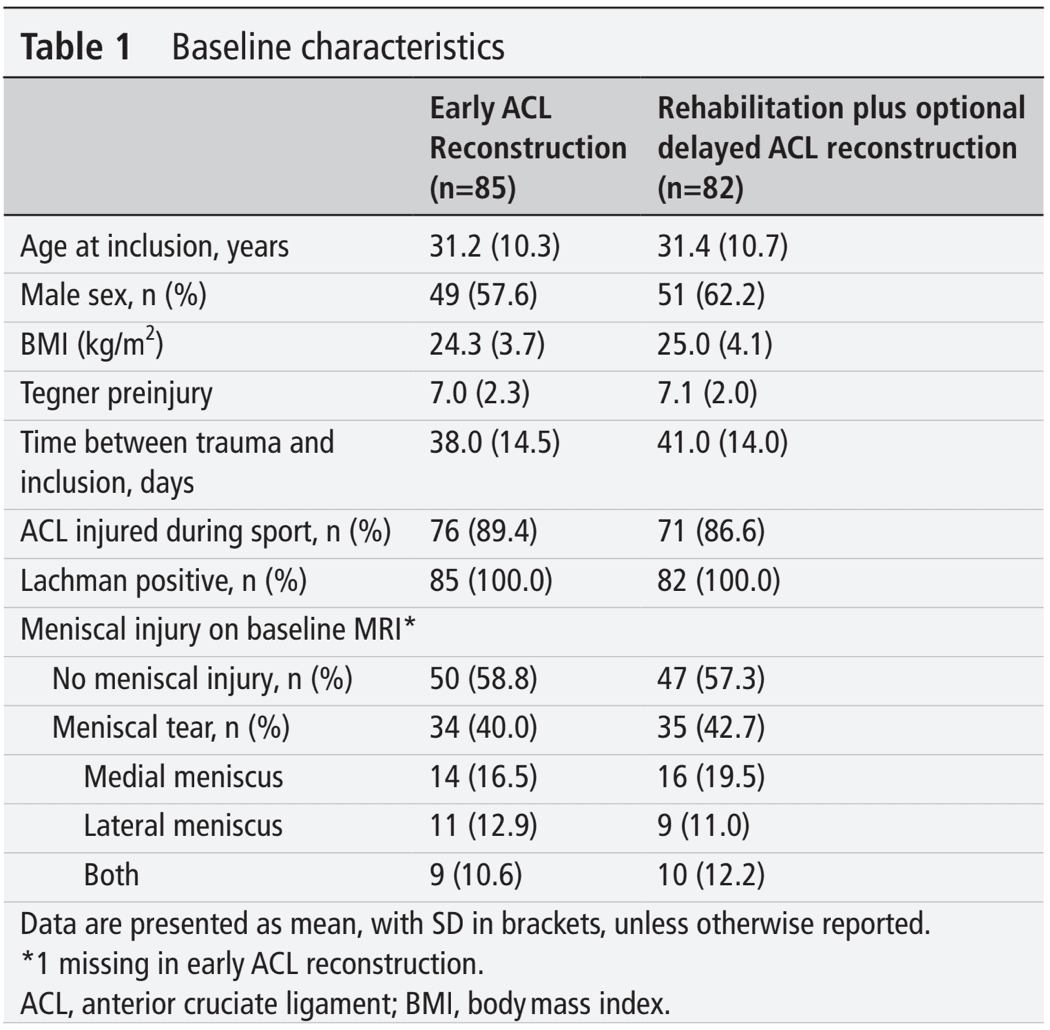
Some patients had a meniscal tear beside their torn ACL at baseline. Again this was equally distributed over the 2 groups.
When looking at the need for meniscus surgery during the 2-year follow-up, respectively 29% and 21% of patients in the early ACL reconstruction group and in the rehabilitation group needed meniscal surgery. This leads to a non-significant risk ratio of 0.67 (95% CI 0.40 to 1.12), meaning that early ACL reconstruction does not protect the meniscus more than rehabilitation with optional delayed ACL reconstruction. Also, After ACL reconstruction, in both treatment groups, no new meniscal procedures were performed in parts of the meniscus other than the area that was already damaged as seen during ACL reconstruction. This means that no new meniscus lesions occurred.
Questions and thoughts
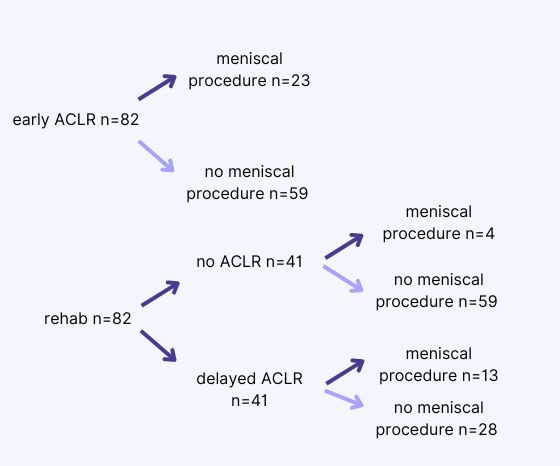
But there is more. When you look at what the authors report, 23 meniscus procedures are performed during the early ACL reconstruction, which equals 28% (23/82). After rehabilitation, of the 41 people who got a delayed ACL reconstruction, 13 received a procedure to their meniscus. That equals 13/41=32%. Of those 41 who did not get their torn ACL operated on, 4 had meniscus surgery, thus 4/41= 10%. Reading this quickly would make you think that those people in the rehabilitation group had a 32%+10%= 42% chance of having to have their meniscus operated on. However, if you calculate the percentage of people having meniscus surgery this gives another result. Then, in the rehabilitation group, 17 (4+13) people out of 82 give you 20% of people needing meniscus surgery. Here you can see the importance of looking at the absolute numbers. While at first glance, you would think that more meniscus surgery is performed in the rehabilitation group, the total numbers reveal otherwise.
What did the conservative intervention consist of?
The conservative arm of this trial consisted of 3 months of supervised physiotherapy, following the Dutch ACL guideline. Exercises were focused on balance and proprioception. This guideline was however from 2012 already. Since then, the rehabilitation of the ACL has moved forward. Check out the webinar by Bart Dingenen to learn more about the current rehabilitation of ACL injuries.
How can I know my torn ACL will spontaneously heal?
Around 50% of torn ACLs were found to heal naturally in the study of Filbay et al. (2023). But this also means that the other half of patients have torn ACLs without spontaneous healing. In this study, half of the patients in the optional delayed ACL reconstruction group got their ACL reconstructed. Was this based on the non-healing of the torn ACL alone, or was it based on patient outcomes and preference? The authors indicate that it was possible in case of persistent instability after a minimum of 3 months of supervised physiotherapy or in case they did not reach their desired activity level after this period. But we do not know what their ACL looked like on MRI.
When do I have a higher chance that I won’t benefit from ACL reconstruction?
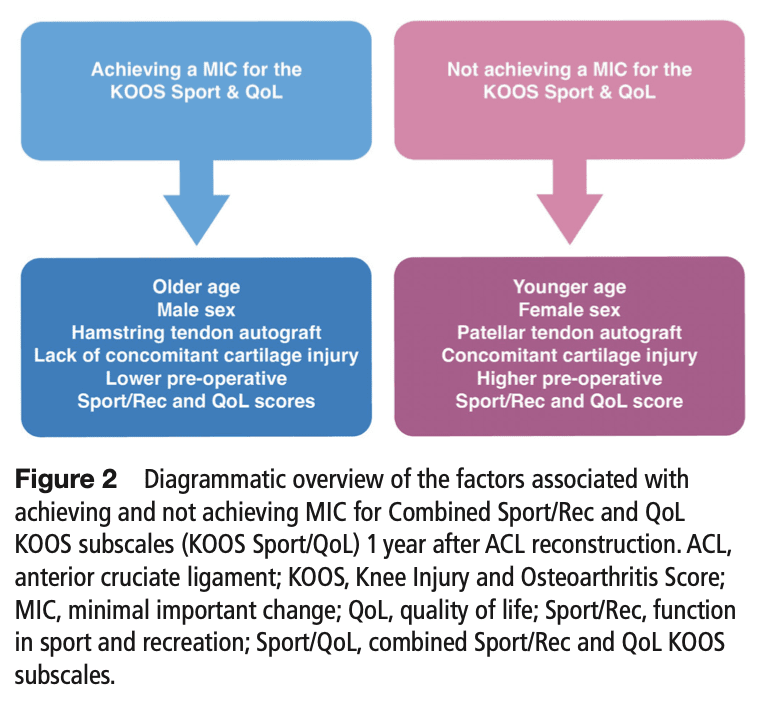
The recent study by Kaarre et al. (2023), found that 44% of the more than 16.000 people included failed to achieve the minimal important change on the KOOS Sport/Rec and Quality of Life subscales. They found that younger patients, females, and those with higher baseline scores on these 2 KOOS subscales had higher odds of not reaching the Minimal Important Change 1 year after their ACL reconstruction. Furthermore, cartilage injuries were also related to higher odds of not achieving the Minimal Important Change.
Is there a difference in outcomes in females or in males? And what about age?
Yes, According to the study by Kaarre et al. (2023). However, this can also be influenced by differences in rehabilitation strategies used and differences in self-efficacy and psychosocial barriers. Younger patients had higher odds of not attaining the Minimal Important Change. This may be reasoned to be because they can have higher knee demands than older patients, who may have lower expectations for knee functioning after ACL reconstruction.
Talk nerdy to me
These findings differ from other large trials such as the KANON trial. This trial found an increased risk of medial meniscal tears in patients randomized to rehabilitation plus optional ACL reconstruction after 5 years (but not after 2 years). This can be explained by the fact that in the KANON trial, a part of the surgeries was counted per individual meniscus, so a meniscal surgery on both the medial and lateral meniscus was counted twice. But also because of the longer follow-up. In time, more traumatic events can occur to the knee, which may cause the meniscus tears to become symptomatic over time.
Take home messages
Early ACL reconstruction protects the meniscus not more than rehabilitation plus delayed optional ACL reconstruction. The number of meniscus procedures in patients with an ACL tear who are treated with rehab is not different from those who undergo early ACL reconstruction. Your patient should therefore not fear damaging their meniscus more by following conservative rehab
Reference
Additional references
LEARN TO OPTIMIZE REHAB & RTS DECISION MAKING AFTER ACL RECONSTRUCTION
Sign up for this FREE webinar and top leading expert in ACL rehab Bart Dingenen will show you exactly how you can do better in ACL rehab and return to sport decision making
