Research
Diagnosis & Imaging
July 6, 2026
Validation of a New Clinical Prediction Rule for Diagnosis of Cervical Radiculopathy with Radicular Pain

Introduction
Cervical Radiculopathy (CR) is a frequent condition resulting from mechanical nerve compression, which may cause neuropraxia (nerve dysfunction without axonal damage) as well as chemical irritation of the nerve root. Its clinical presentation is highly variable across patients, making history-taking alone of limited diagnostic value. Although multiple clinical tests have been proposed to aid diagnosis, none have shown sufficient validity when used in isolation.
In 2023, Wainner et al. proposed a four-test clinical cluster (ULNT1, Spurling’s test, cervical distraction test, and cervical range of motion < 60° on the symptomatic side). However, this cluster has not yet undergone external validation, meaning its diagnostic performance has not been tested in broader and more heterogeneous populations with varying disease severity and demographic characteristics.
The present study aimed to externally validate the Wainner cluster for the diagnosis of cervical radiculopathy and to explore whether an alternative cluster of tests could achieve superior diagnostic accuracy.
Methods
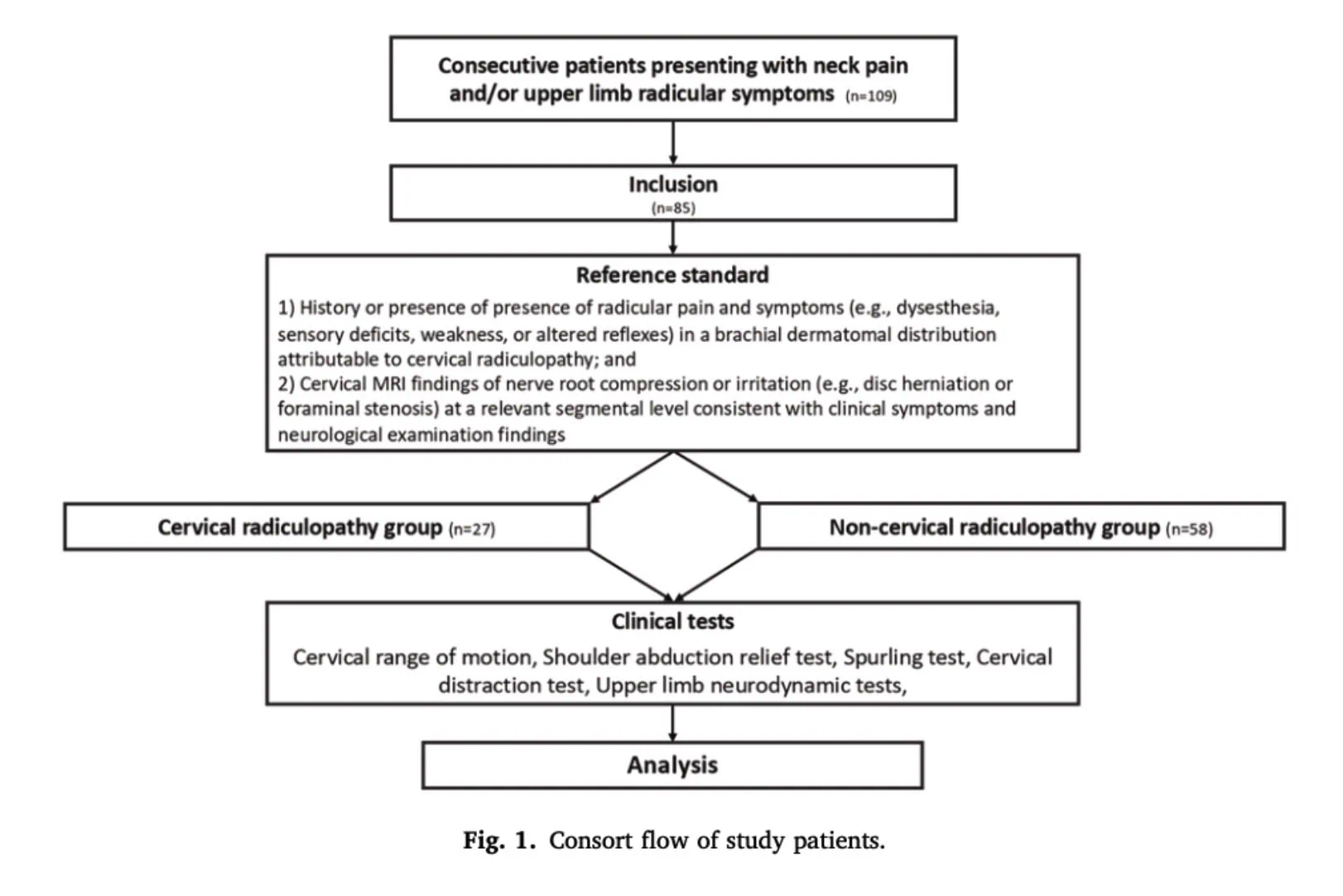
This prospective diagnostic accuracy study enrolled a consecutive cohort of patients presenting with neck pain and/or cervical radicular symptoms in the context of routine diagnostic uncertainty. The study adhered to the 2015 Standards for Reporting Diagnostic Accuracy Studies (STARD) guidelines.
Participants
Consecutive patients referred to a neurosurgery department with chronic (≥3 months) neck pain and/or cervical radicular symptoms. Eligible participants were aged 18–65 years, had moderate pain (VAS 30–79/100) and neck disability (NDI ≥20%), and underwent a standardized diagnostic work-up including MRI. Patients with previous cervical surgery, significant trauma, cervical myelopathy, major comorbidities, pregnancy, or inability to communicate in French were excluded.
Index test
Twelve clinical tests and history findings were evaluated against the reference standard on the same day. These included the modified Bakody’s sign, Spurling’s test (neck and arm symptom reproduction), cervical distraction test, four upper limb neurodynamic tests (ULNT1, ULNT2a, ULNT2b, ULNT3), cervical rotation <60°, asymmetric cervical ROM, age >48 years, and symptom duration <62 weeks. Clinical testing was performed by a blinded, experienced physiotherapist using predefined criteria for positive, negative, or indeterminate results.
As age and symptom duration are continuous variables, receiver operating characteristic (ROC) curve analysis was used to determine the thresholds that best discriminated between patients with and without cervical radiculopathy. The resulting cut-offs (age >48 years and symptom duration <62 weeks) allowed these variables to be converted into binary diagnostic predictors for subsequent analyses.
All index tests were classified as positive or negative according to predefined criteria, while tests that could not be completed due to patient intolerance were considered indeterminate.
Reference standards
The reference standard diagnosis was established by a neurosurgeon with 15 years of experience who was blinded to the results of the index tests. Cervical radiculopathy was diagnosed based on the combination of compatible clinical findings (dermatomal radicular pain and/or neurological signs) and MRI evidence of nerve root compression or irritation at the corresponding cervical level.
Analysis
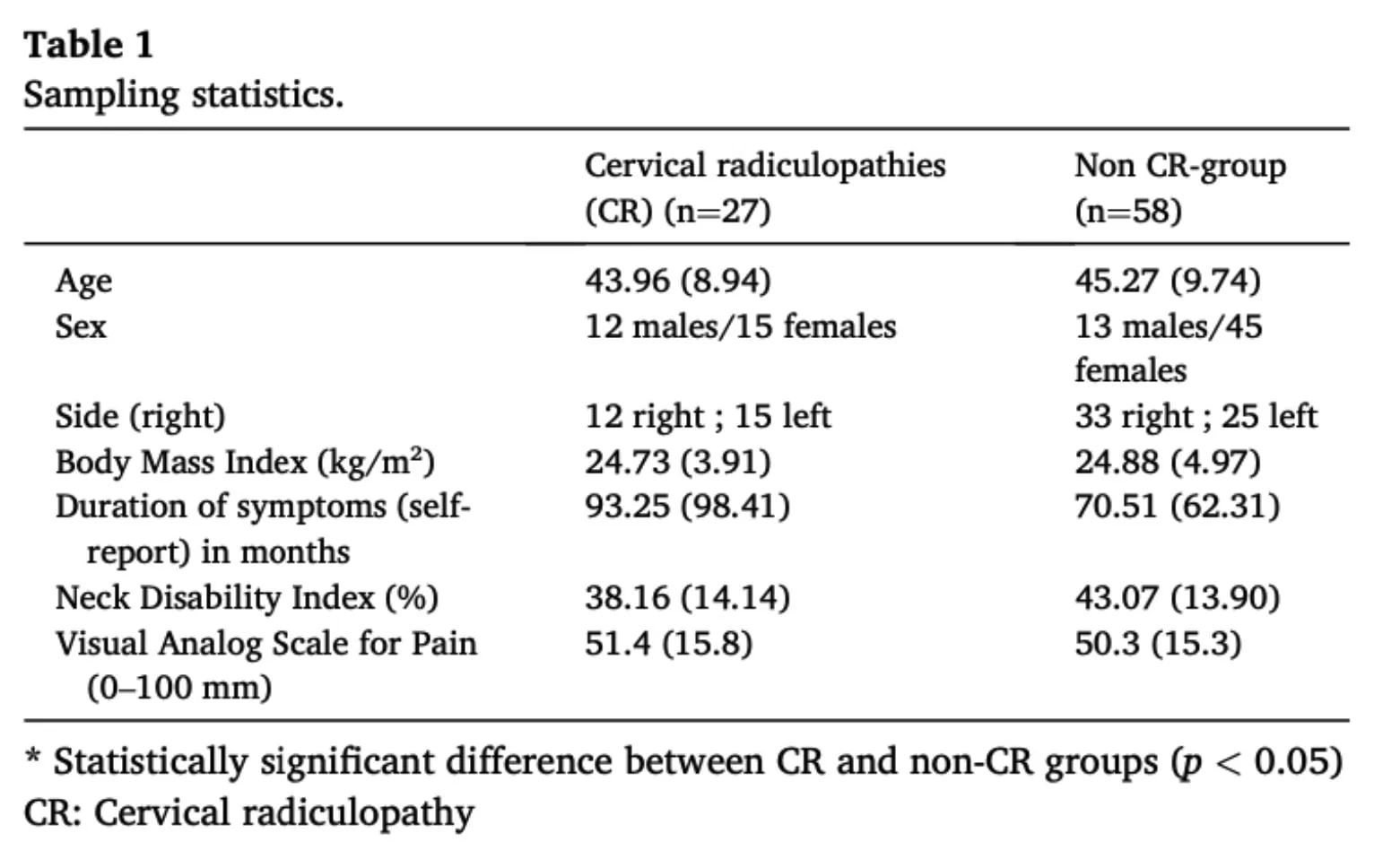
First, the authors compared the cervical radiculopathy (CR) and non-CR groups in terms of baseline demographic characteristics. Continuous variables (e.g., age) were described using means and standard deviations, while categorical variables (e.g., sex) were presented as frequencies and percentages. Between-group comparisons were performed using the Wilcoxon rank-sum test for continuous variables, and the chi-square test or Fisher’s exact test for categorical variables, depending on sample size. This step aimed to assess baseline differences between groups.
The diagnostic accuracy of each clinical test was then evaluated using 2 × 2 contingency tables constructed against the reference standard, as illustrated below:

From these tables, sensitivity and specificity were calculated. Sensitivity represented the proportion of patients with CR who tested positive, whereas specificity represented the proportion of patients without CR who tested negative.
Likelihood ratios were subsequently derived using standard formulas. The positive likelihood ratio (LR+) was calculated as sensitivity / (1 − specificity) and reflects the extent to which a positive test increases the probability of CR. The negative likelihood ratio (LR−), calculated as (1 − sensitivity) / specificity, indicates the extent to which a negative test decreases the probability of CR.
Post-test probabilities were then estimated using Bayes’ theorem, incorporating the pre-test probability (i.e., prevalence of CR in the sample) and the likelihood ratios. For positive and negative test results, post-test probabilities were calculated using the following equations:
Post-test probability (positive test) = (pre-test probability × LR+) / [(pre-test probability × LR+) + (1 − pre-test probability)]
Post-test probability (negative test) = (pre-test probability × LR−) / [(pre-test probability × LR−) + (1 − pre-test probability)]
In addition, receiver operating characteristic (ROC) curve analyses were performed for continuous variables (age and symptom duration) to determine optimal cut-off values. Multiple thresholds were tested, and the values providing the best balance between sensitivity and specificity were selected.
For the first study objective, the authors validated the existing Wainer’s clinical prediction rule by creating combinations of positive findings (1 of 4, 2 of 4, 3 of 4, and 4 of 4 positive tests). For each combination, diagnostic accuracy measures, including sensitivity, specificity, likelihood ratios, and post-test probabilities, were recalculated.
For the second objective, the authors developed a new clinical prediction rule. Initially, each variable was assessed individually using 2 × 2 analyses, and only those demonstrating potential diagnostic utility (LR+ > 1.5 and/or LR− < 0.5) were retained. A backward stepwise logistic regression model was then applied to identify independent predictors, with variables entering the model at p < 0.10 and removed at p > 0.15. Finally, the retained variables were combined to construct a new cluster for cervical radiculopathy diagnosis.
Results
The study included 85 participants, of whom 31.7% (n = 27) had a cervical radiculopathy diagnosis (CR). The non-CR group comprised 58 participants, including 42 with neck pain without a cervical radiculopathy diagnosis, 12 with peripheral nerve entrapment, and 4 with diffuse shoulder pain. The proportion of female participants was higher in the non-CR group, whereas symptom duration was longer among participants with CR.
The diagnostic accuracy of the 12 selected clinical tests is presented in Table 2, including their sensitivity, specificity, likelihood ratios, and post-test probabilities. Among the individual tests, the highest sensitivity (96.3%) was observed for the criterion of at least one positive upper limb neurodynamic test (ULNT) out of four.
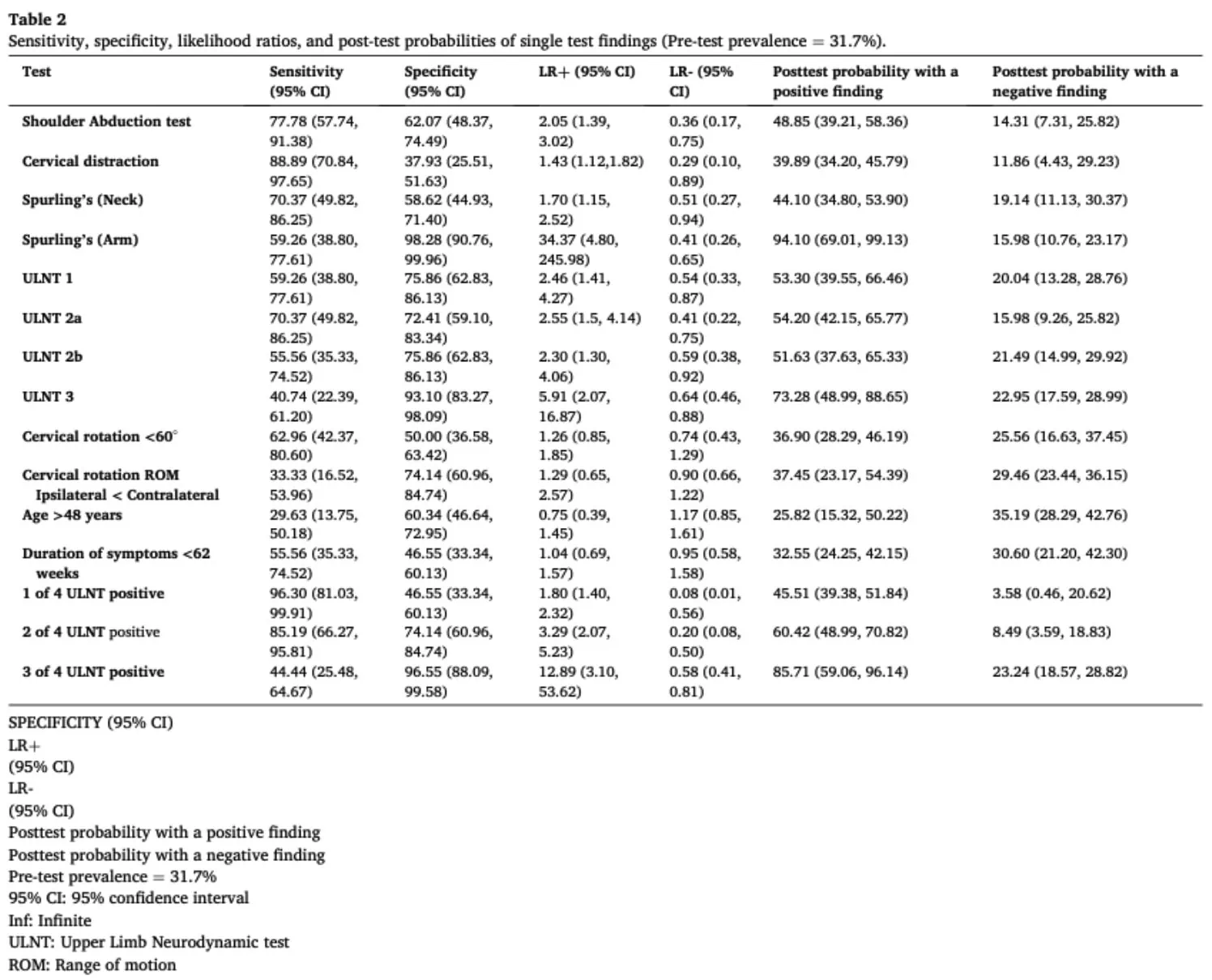
The Spurling arm pain test demonstrated the highest specificity (98.3%), with a positive likelihood ratio (LR+) of 34.37, corresponding to a post-test probability of 94.1% following a positive result. Conversely, the cervical distraction test was the most effective individual test for ruling out CR, with a negative post-test probability of 11.9%.
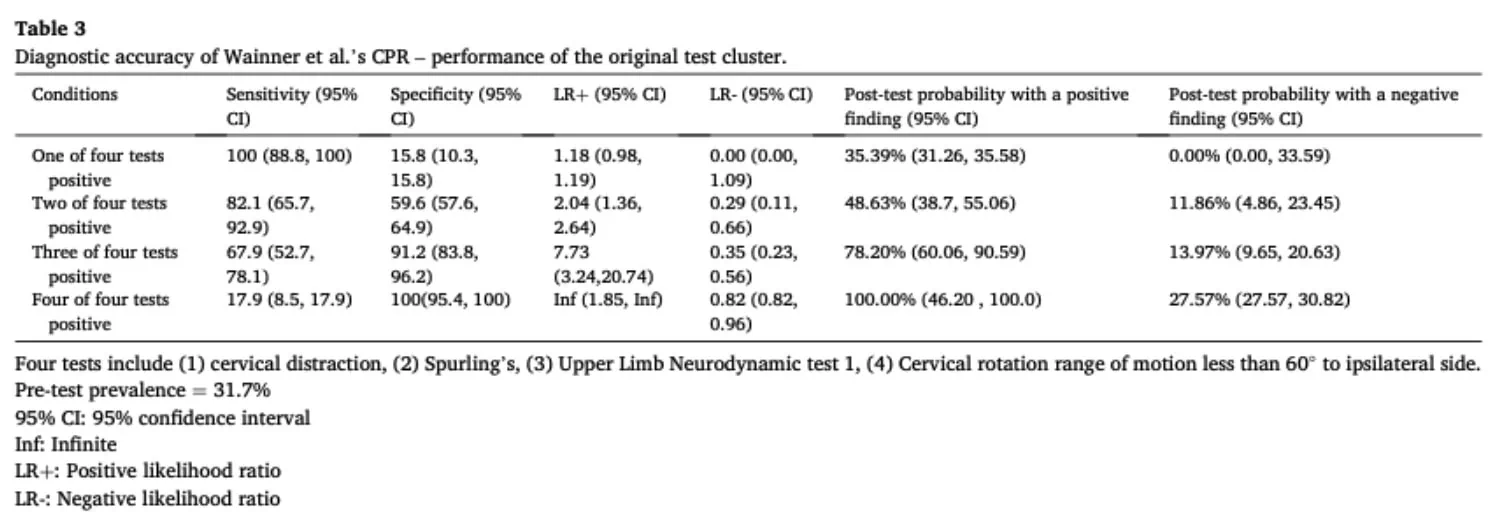
To evaluate the diagnostic validity of the Wainner test cluster, the authors examined different combinations of positive findings. The most sensitive criterion was the presence of at least one positive test out of the four, whereas the most specific required all four tests to be positive. Notably, when none of the four tests were positive, all cases of CR were correctly excluded (LR− = 0; post-test probability = 0%). Conversely, when all four tests were positive, the positive likelihood ratio approached infinity, resulting in a post-test probability of 100%. However, requiring all four tests to be positive identified only 17.9% of patients with CR, reflecting limited sensitivity despite excellent specificity.
To address the second study objective, the authors performed backward stepwise regression analysis on eight candidate variables: the shoulder abduction test, cervical distraction test, Spurling’s neck pain test, Spurling’s arm pain test, and the four ULNTs. This analysis identified three variables for the final diagnostic model:
- Modified shoulder abduction test
- Spurling arm pain test
- Two or more positive ULNTs out of four
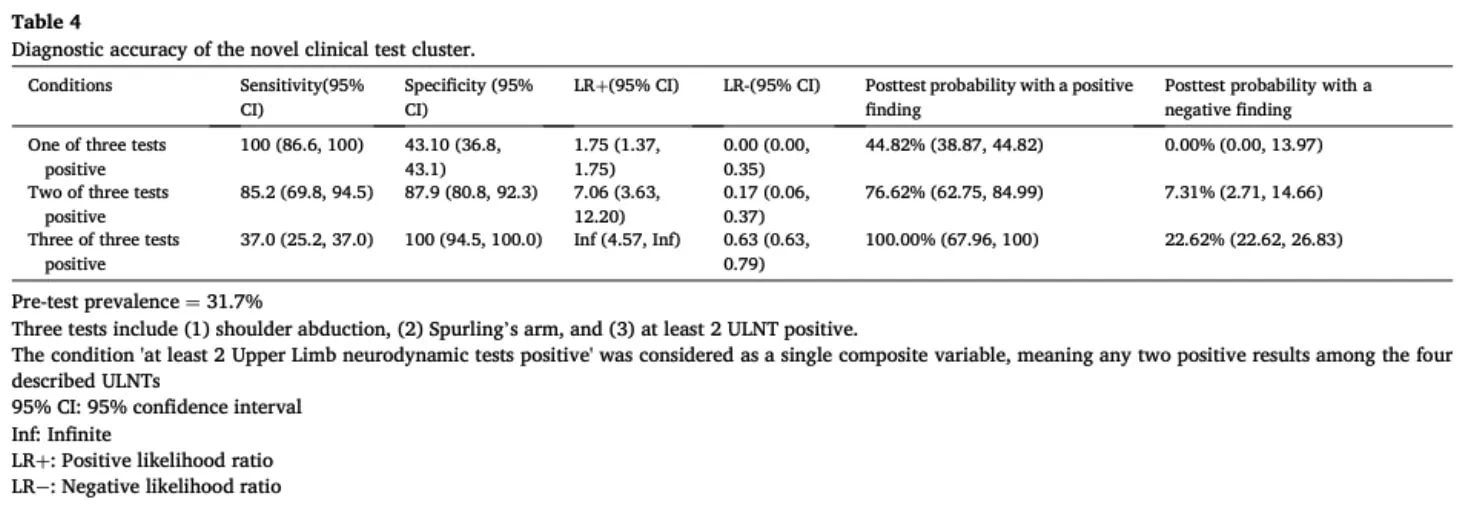
This simplified diagnostic cluster demonstrated promising diagnostic performance. When none of the three criteria were positive, all cases of CR were correctly ruled out. Conversely, when all three criteria were positive, the positive likelihood ratio was infinite, yielding a post-test probability of 100%. A result of two positive findings out of the three produced an LR+ of 7.06 and an LR− of 0.17.
Importantly, compared with the original Wainner cluster, the simplified three-test model improved sensitivity at its highest diagnostic threshold. Requiring all three tests to be positive correctly identified 37% of patients with cervical radiculopathy, more than doubling the proportion identified by the original four-test cluster (17.9%) while maintaining perfect specificity.
Questions and thoughts
The test conditions proposed by the study authors suggest that this new cluster may be useful for both ruling in and ruling out cervical radiculopathy. When none of the three criteria are positive, all cases of cervical radiculopathy were correctly ruled out, whereas the presence of all criteria resulted in a 100% rule-in rate.
However, in clinical practice, test results are rarely so clear-cut. Individual test findings must therefore be interpreted in combination to better guide clinical reasoning. Tests with high sensitivity are particularly valuable for ruling out cervical radiculopathy diagnosis, such as the cervical distraction test and the modified shoulder abduction test. It should be noted, however, that both are symptom-relieving maneuvers; consequently, patients who are asymptomatic at rest may not exhibit a response, which could reduce their diagnostic performance in practice.
Highly sensitive tests, such as ULNTs, are especially useful for excluding radiculopathy. In this study, at least one positive ULNT among the four tested yielded a sensitivity of 96.3% and a negative likelihood ratio of 0.08. In comparison, the cervical distraction test and modified shoulder abduction test showed weaker rule-out capacity, with LR− values of 0.29 and 0.36, respectively. This suggests that ULNTs represent a particularly valuable clinical tool, especially in patients with ambiguous presentations where cervical involvement may contribute to upper limb symptoms.
ULNTs are particularly relevant given that cervical disorders can mimic peripheral musculoskeletal conditions. They should therefore be included in the assessment of patients presenting with unclear upper limb symptoms. Neuromeningeal testing can help identify neural mechanosensitivity and guide clinical reasoning. Subsequently, cervical distraction and Spurling’s test may be used in combination to further assess whether the cervical spine is a potential source of nerve root involvement or entrapment.
Talk nerdy to me
To derive a new clinical prediction rule (CPR), the authors used a stepwise logistic regression approach. This method begins with a set of candidate variables (in this case, clinical tests) and sequentially selects or removes predictors based on statistical criteria to identify the model that best predicts the outcome (cervical radiculopathy diagnosis). In essence, stepwise regression aims to identify the smallest combination of variables that optimally predicts the outcome within the study dataset.
A limitation of this approach is that it prioritizes statistical optimization over clinical interpretability and reproducibility. Because variable selection is driven by statistical significance within a single sample, the resulting model may overfit the data and overestimate diagnostic performance. In particular, rare or sample-specific patterns may disproportionately influence variable selection, leading to unstable or non-replicable results.
Consequently, findings derived from stepwise regression should be interpreted as sample-dependent and primarily exploratory. The resulting diagnostic performance may therefore be overly optimistic and not fully generalizable to other patient populations.
In addition, stepwise regression may exclude clinically relevant tests if they do not provide independent predictive value beyond other variables in the model. For example, although the cervical distraction in this sample demonstrated high sensitivity (88.89%), it was not retained in the final model. This is likely due to statistical redundancy, as it does not contribute additional independent information once other correlated tests (e.g., Spurling’s test and ULNT) are included. These tests may reflect overlapping constructs, such as cervical nerve root mechanosensitivity, which contributes to collinearity among predictors.
Therefore, external validation is essential to assess the robustness and generalizability of the proposed clinical prediction rule. While the diagnostic accuracy of the original Wainner cluster appears broadly comparable to that reported in this study, its low sensitivity in identifying cervical radiculopathy (17.9% when all four tests are positive) limits its clinical utility. The new proposed cluster may improve diagnostic performance, but its validity remains contingent on replication in independent samples.
Take-home messages
- No single clinical test can confidently include or exclude cervical radiculopathy. Diagnostic confidence is improved by combining patient history, neurological findings, and a cluster of physical examination tests.
- Upper limb neurodynamic tests (ULNTs) remain one of the most valuable screening tools for cervical radiculopathy. Their high sensitivity means that a negative ULNT substantially reduces the likelihood of cervical nerve root involvement.
- The Spurling arm pain test demonstrated excellent specificity, making it particularly useful for ruling in cervical radiculopathy when positive.
- The proposed three-test cluster (modified shoulder abduction test, Spurling arm pain test, and ≥2 positive ULNTs) identified more patients with cervical radiculopathy than the original Wainner cluster while maintaining excellent rule-in performance.
- Because the new clinical prediction rule was developed using stepwise logistic regression in a single cohort, its diagnostic accuracy should be interpreted cautiously until it is externally validated in independent populations.
- Cervical radiculopathy can mimic shoulder disorders and peripheral nerve entrapments. Including cervical screening and neurodynamic testing in the assessment of patients with unexplained upper limb symptoms may help identify cervical nerve root involvement and guide appropriate management.
Reference
TWO MYTHS BUSTED & 3 KNOWLEDGE BOMBS FOR FREE
What university doesn’t tell you about shoulder impingement syndrome and scapula dyskinesis and how to massively level up your shoulder game without paying a single cent!