
Research
EBP & Statistics
August 22, 2025
CFT for Chronic LBP: Lessons from a 3-Phase, 3-Year Research Program.

Introduction
Chronic low back pain (CLBP) is a highly disabling condition, with 20–30% of acute episodes progressing to chronicity, leading to substantial healthcare costs and limited treatment success. CLBP is now widely acknowledged as a biopsychosocial disorder in which psychological factors play a central role. Conventional treatments typically achieve only modest improvements in pain and function, whereas Cognitive Functional Therapy (CFT) has emerged as a promising, patient-centered approach. CFT promotes self-management by addressing maladaptive cognitions, emotions, and behaviors associated with pain and disability.
Wearable movement sensors provide an opportunity to deepen the understanding of movement behaviors and their interaction with psychological drivers of pain and disability . When combined with biofeedback, they allow patients to gain awareness of maladaptive movement patterns during daily activities, supporting behavioral change and motor retraining.
Previous studies suggest that individualized rehabilitation with biofeedback outperforms usual care. To test this, a three-arm RCT compared CFT, CFT plus biofeedback, and usual care across three stages: the study protocol (2019) main trial results at 52 weeks (2023) and extended 3-year follow-up (2025). This review summarizes both short- and long-term findings to provide an overview of the evidence supporting CFT for chronic LBP.
Methods
The research trial was first introduced in a 2019 protocol comparing usual care, CFT combined with biofeedback and CFT for chronic LBP. Findings from the 52-week follow-up were published in 2023. The present paper reports the extended 156-week follow-up, assessing long-term outcomes on pain and function. The trial included three parallel groups—usual care, CFT, and CFT plus movement-sensor biofeedback—and was conducted across 20 primary care physiotherapy clinics in Perth and Sydney, Australia.
Inclusion criteria
Participants were adults (≥18 years) with chronic low back pain (>3 months), average pain intensity ≥4/10, and at least moderate interference with work/daily activities.
Exclusion criteria
exclusion criteria: if they had poor English literacy, if they were scheduled for upcoming surgery, or if they were unwilling to travel to the trial sites. Those with skin allergies to tape were excluded as well.
Randomization was centralized, stratified by site, sex, and baseline disability, with allocation concealed. Participants were aware of their group, physiotherapist were unblinded to patient group and delivered one type of treatment. Statisticians were masked, and outcome assessors were not involved in treatment delivery. Outcomes were self-reported via online questionnaires, collected from movement sensors, or drawn from government health registers.
Usual care group: Based on their therapist’s recommendations, participants selected their own treatment (such as physiotherapy, massage, chiropractic care, medications, injections, or surgery), which they pursued independently and paid for themselves. They received a small reimbursement for completing follow-up questionnaires.
CFT groups: Up to seven sessions over 12 weeks plus a 26-week booster, this later session was added because previous researched showed that persons with higher level of pain and decreased function had less long term CFT treatment effects. The approach was individualized, using patient narratives, physical examination, and patient-centered communication to target contributing biopsychosocial factors.
- Component 1 – Making sense of pain: Reframing pain from a biopsychosocial perspective, addressing unhelpful beliefs, and developing flare-up self-care plans.
- Component 2 – Exposure with control: Gradual exposure to feared/painful activities with movement retraining, relaxation, and postural modification, supported by daily exercise program. The objective was to enhance pain control and increase patients’ confidence in engaging in meaningful activities.
- Component 3 – Lifestyle change: Coaching on physical activity, sleep, diet, stress management, and social engagement.
Biofeedback subgroup: Movement sensors provided real-time feedback, data-guided retraining, and smartphone prompts to reinforce movement goals.
The intervention involved three main strategies:
- Movement assessment – During clinic sessions, physiotherapists could observe and record the patient’s spinal movements in real time to identify patterns potentially contributing to pain.
- Real-time feedback – Patients received visual and auditory cues during treatment sessions to help them modify movement and posture. This experiential learning aimed to reduce protective behaviors and increase confidence in movement.
- Daily-life biofeedback – Physiotherapists programmed smartphone alerts (beeps, messages) to support self-management outside the clinic. Prompts could remind patients to avoid prolonged static postures (e.g., slumped sitting), to achieve activity targets (sitting, standing, walking, lying), or to complete exercises at set intervals.
Both CFT groups wore movement sensors and in the CFT-only group, sensors were placebo. The sensors were two devices attached to the lumbar spine at sacrum level and L1.
During COVID-19 lockdowns, some follow-ups were conducted via telehealth, limiting the use of movement sensors. This may have affected up to 9% of sessions in the CFT plus biofeedback group. Recruitment was also paused for 9 weeks to ensure all participants received an initial face-to-face consultation.
Eighteen physiotherapists completed 80 hours of CFT for chronic LBP training over 5 months, supported by mentoring, quarterly virtual meetings, and online resources. Competency was assessed via checklists, a final workshop, and video reviews of treatment. To prevent cross-contamination, each physiotherapist delivered only one intervention. All therapists received a 2-hour workshop on sensor setup, while those in the CFT plus biofeedback group had an additional 4 hours on data interpretation and biofeedback programming.
Outcomes
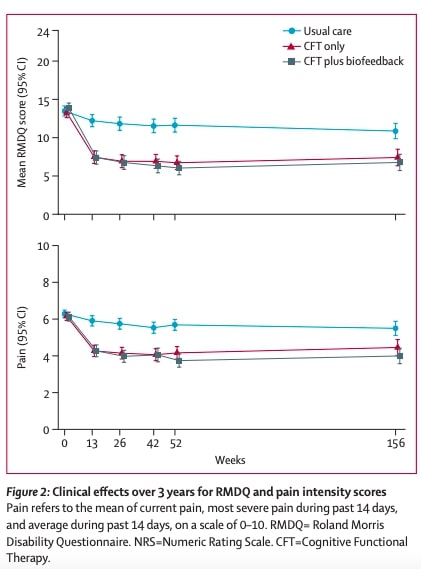
The primary outcome was pain-related physical activity limitation, measured with the Roland Morris Disability Questionnaire (RMDQ) on a 0 to 24 scale with higher score corresponding to greater disability. This was assessed at 13 weeks and again at 3 years for the extended follow-up.
The secondary outcome for the extended follow-up was pain intensity at 3 years, calculated as the mean of three numeric rating scales (current pain, worst pain in the past 14 days, and average pain in the past 14 days; all 0–10).
An economic analysis was conducted for the 2023 trials, the main measure was quality-adjusted life-years (QALYs) from EQ-5D-5L data. Costs included healthcare resource use (from Medicare and Pharmaceutical Benefits Scheme databases plus patient questionnaires) and productivity losses (iMTA questionnaire).
- Further secondary outcomes (measured only during the 52-week trial):
- Patient-specific functional limitation: Patient-Specific Functional Scale (0–10).
- Pain catastrophising: 3-item scale (0–12, all timepoints) and 13-item scale (0–52, baseline only).
- Pain self-efficacy: Pain Self-Efficacy Questionnaire (0–60).
- Fear of movement: physical activity subscale of the Fear Avoidance Beliefs Questionnaire (0–24).
- Global improvement: single-item patient-perceived measure (one question).
- Satisfaction with care/treatment: single-item measure (one question).
- Adverse events: reported by physiotherapists or participants.
- Treatment expectation: single tailored question after randomization.
- Treatment adherence (intervention groups): self-rated on a 0–10 scale.
Results
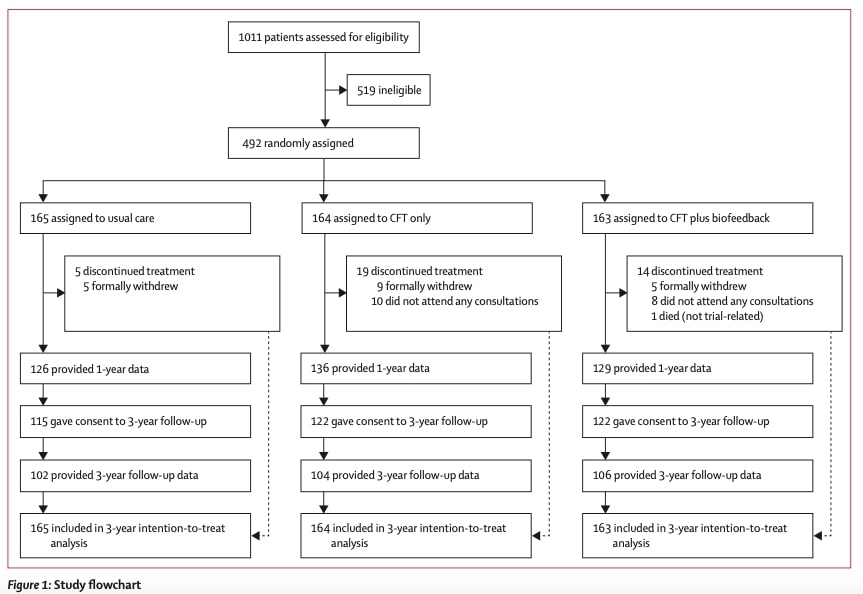
Between October 2018 and August 2020, 1011 patients were screened, and 492 were recruited: 165 allocated to usual care, 164 to CFT for chronic LBP only, and 163 to CFT plus biofeedback. About one-third (160 participants) declined consent for linkage to Medicare and Pharmaceutical Benefits Scheme data, more commonly in the usual care group. At the primary outcome timepoint (13 weeks), follow-up was achieved for 418 participants (85% overall), with similar retention across groups.
In both intervention groups, participants attended a median of seven consultations (IQR 4–8), though 8% in each group did not attend any sessions, partly due to COVID-19 disruptions. The median delay between baseline assessment and first consultation was 9 days in the CFT-only group and 8 days in the CFT plus biofeedback group.
In the usual care group, 56% were using medication for low back pain at baseline. By 13 weeks, 82% provided follow-up data, with 38% reporting care-seeking from a health professional. Among these, the median number of consultations was three (IQR 2–7, range 1–22), though care access may have been affected by pandemic-related lockdowns.
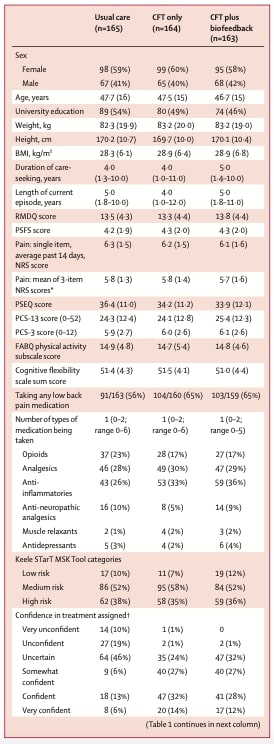
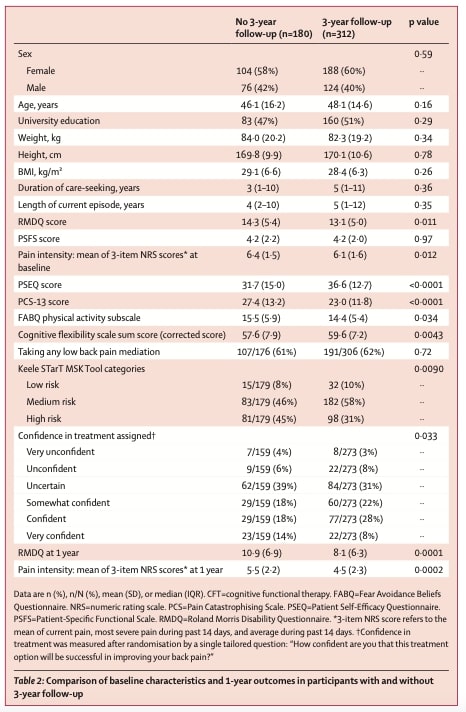
Baselines characteristics are presented in the three tables below. Interestingly, participants who completed the 3-year follow-up had milder baseline symptoms and better 1-year outcomes than those lost to follow-up. However, these differences were consistent across all treatment groups, with no evidence of differential loss to follow-up

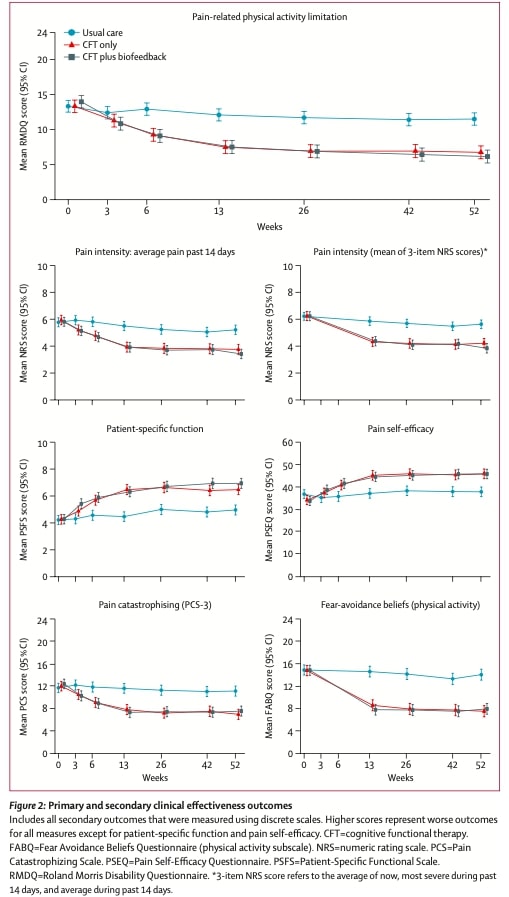
At 13 weeks, both CFT alone and CFT for chronic LBP combined with biofeedback led to substantially greater improvements in activity limitation compared with usual care, with patients in the CFT groups reporting an average reduction of 4–5 points on the RMDQ—a difference reflecting a large effect size. These improvements were not only clinically significant but also durable, remaining stable through the 52-week follow-up. At 3 years follow up, clinically important improvement in activity limitation (≥5-point RMDQ reduction) was achieved by 62% of participants in the CFT group and 74% in the CFT plus biofeedback group, compared with only 33% in the usual care group.
Critically, there was no meaningful difference between CFT alone and CFT enhanced with biofeedback. Both interventions performed equally well, suggesting that the addition of biofeedback did not amplify treatment effects.
When examining clinically meaningful improvement (defined as a ≥5-point reduction on the RMDQ) at 52 weeks, the results were striking: while only 19% of usual care patients achieved this threshold, 61% of the CFT-only group and 60% of the CFT plus biofeedback group met this benchmark. This translates to a number needed to treat (NNT) of just 2–3, meaning that for every 2–3 patients treated with CFT (with or without biofeedback), one additional patient attained meaningful improvement compared to usual care.
These patterns were consistent across secondary outcomes, including pain, function, and patient satisfaction. At 13 weeks, satisfaction rates were markedly higher in the CFT groups (79–84%) than in usual care (19%), further underscoring the patient-centered benefits of CFT.
cost utility analysis
The economic analysis showed clear advantages for both CFT treatments compared to usual care. When looking at CFT alone versus usual care, the results demonstrated that CFT was not only more effective – providing an additional 0.12 quality-adjusted life years (QALYs) per patient – but also less expensive, saving $5,276 per patient on average. These savings came primarily from reduced productivity losses. There was a 97% probability that CFT alone was both more effective and less costly than usual care.
Similarly, CFT with biofeedback showed even greater savings ($8,211 per patient) while delivering slightly better outcomes (0.13 QALYs gained) compared to usual care, with a 99.8% probability of being cost-effective.
However, when comparing the two CFT approaches directly, the results were less definitive. Some analysts suggested biofeedback might be preferable (with an 80-85% probability of being cost-effective), while other methods showed CFT alone might be slightly better (33% probability). This inconsistency means we can’t confidently say one approach is economically superior to the other.
Adverse events are described in the following Table 3 and were evenly distributed across groups.

Questions and thoughts
Within the study protocol, the close monitoring of therapists delivering CFT for chronic LBP ensured strong treatment fidelity and enhanced the reliability of the results. This standardization reinforces the conclusion that CFT for chronic LBP is both effective and promising. Furthermore, the broad inclusion criteria and minimal exclusions improved the generalizability of the findings. Nonetheless, it remains essential to replicate these outcomes across diverse cultural and healthcare settings to better understand the international applicability of CFT.
Another crucial consideration is the need for comprehensive clinician training, as consistent and effective delivery of CFT for chronic LBP depends on therapist expertise. Finally, given that CFT is a highly individualized intervention, the use of standardized and quantifiable clinical assessments is vital for evaluating progress and refining treatment strategies.
Some limitations must be acknowledged. Patients were not blinded to their treatment allocation or to the study hypotheses, which raises the possibility of performance bias and response bias, since the clinical outcomes were mainly based on self-reported measures. This could have inflated the observed effects. However, the 3-year follow-up results, which demonstrated sustained improvements in pain and disability with both CFT and CFT plus biofeedback, reduce the likelihood that these findings were solely due to bias. Interestingly, a randomized controlled trial (reviewed on Physiotutors) have shown that even when patients were blinded, CFT remained superior to CFT sham treatment in improving pain and function, further supporting the robustness of its effects. The authors noted that patients completing the 3-year follow-up generally reported lower disability. Similar findings have been observed in other studies reviewed on Physiotutors. This pattern suggests that individuals with higher baseline disability may gain greater benefit from CFT compared to those with milder limitations. Future research should investigate why patients with fewer activity restrictions respond less effectively to CFT.
Talk nerdy to me
The research team employed several advanced statistical techniques to ensure their findings about Cognitive Functional Therapy (CFT) were robust and reliable. First, they used an intention-to-treat (ITT) approach, which means every participant was analyzed according to their original treatment group assignment, regardless of whether they completed the full treatment protocol or dropped out early. This method preserves the real-world applicability of the results and prevents bias that might occur if only the most compliant patients were included.
For analyzing the outcomes over time, the researchers chose linear mixed models (LMM), a sophisticated statistical method particularly well-suited for this type of research. These models accounted for several important factors: they handled repeated measurements from the same participants at different time points, adjusted for the fact that some therapists treated multiple patients (what statisticians call “nesting”), and managed missing data in a way that minimized potential bias. The LMM approach is powerful because it uses all available data to estimate likely values for missing follow-up measurements, assuming the data was missing randomly after accounting for known factors.
The study didn’t adjust for multiple comparisons, which might sound concerning at first, but was actually a thoughtful decision. Since all three group comparisons (usual care vs. CFT alone vs. CFT with biofeedback) were pre-specified as equally important primary questions, the researchers maintained their original statistical thresholds rather than making adjustments that could unnecessarily reduce their ability to detect real differences.
To handle missing data – a common challenge in long-term studies – the team used multiple imputation. This technique creates several plausible versions of the complete dataset by predicting missing values based on all the other available information from participants. They generated ten of these complete datasets, analyzed each one, and then combined the results. This approach is more reliable than simply excluding participants with missing data, as it preserves the study’s original sample size and power while accounting for uncertainty about the missing values.
When interpreting the size of treatment effects, the researchers calculated standardized mean differences (SMDs). This statistic expresses the difference between groups in terms of standard deviation units, allowing comparison across different measures. In this study, SMDs greater than 0.8 indicated large treatment effects – meaning CFT wasn’t just statistically better than usual care, but the improvements were substantial enough to be clinically meaningful.
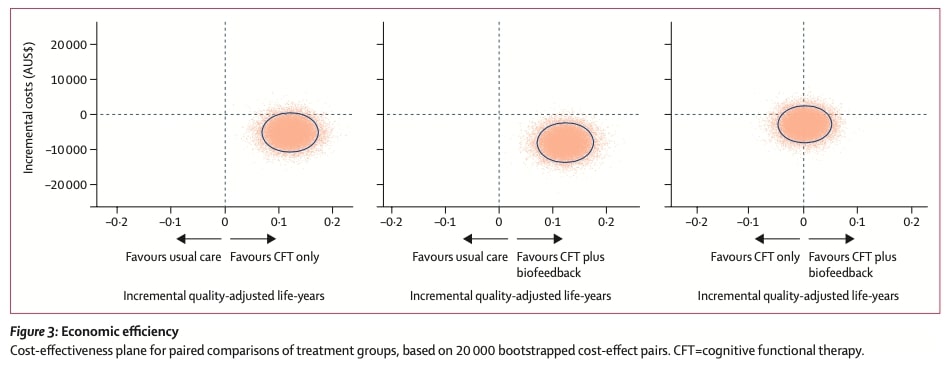
For the economic analysis, the team used bootstrapping, a resampling technique that helps estimate the precision of cost-effectiveness results. By repeatedly simulating the study results (20,000 times in this case), they generated the data shown in Figure 3, where each dot represents one simulated comparison of costs and effectiveness (QALYs).
To interpret Figure 3:
- The X-axis shows incremental QALYs (health benefits), where values further right indicate greater effectiveness
- The Y-axis shows incremental costs in AUS$, with values below zero representing cost savings
- The four quadrants reveal key relationships:
- Lower-right (more effective + cheaper): Where 97-99.8% of dots fell for CFT vs. usual care
- Upper-right (more effective but more expensive)
- Lower-left (less effective but cheaper)
- Upper-left (less effective + more costly)
The high concentration of dots in the lower-right quadrant (97-99.8% of simulations) gave strong confidence that CFT was truly more cost-effective than usual care. This visual clustering in Figure 3 powerfully demonstrates both the economic and clinical superiority of CFT.
Takes home messages
CFT (Cognitive Functional Therapy) is highly effective for chronic low back pain, producing large, clinically meaningful improvements in pain and activity limitation—both short-term (13 weeks) and long-term (3 years). These sustained benefits are rare among conservative interventions.
Biofeedback adds no extra benefit—CFT alone is just as effective as CFT with sensor-based biofeedback. Resources may be better spent on high-quality CFT for chronic LBP
delivery rather than additional technology.
Cost-effective & societal savings: Both CFT approaches are cheaper than usual care from a societal perspective, primarily due to reduced productivity losses (fewer work absences). The intervention pays for itself over time.
Key mechanisms of success:
-
- Targets psychological factors (fear avoidance, catastrophizing, self-efficacy).
- Emphasizes self-management coaching (biopsychosocial approach, movement retraining).
- Includes a booster session (at 6 months), which likely contributes to long-term effects.
Training matters:
-
- Therapists were trained to competency with mentoring and real-patient practice.
- This level of training may be critical for replicating results
Implementation opportunity:
-
- CFT offers a high-value, low-risk alternative to opioids, surgery, or multidisciplinary programs.
- Policy changes could improve access, reducing the global burden of low back pain.
For a deeper understanding, CFT is comprehensively described by its creators in this open-access article
You can also gain additional insights through this Physiotutors podcast episode
Finally, this Physiotutors webinar provides practical guidance on applying CFT for chronic LBP in clinical practice
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Watch this FREE video lecture on Nutrition & Central Sensitisation by Europe’s #1 chronic pain researcher Jo Nijs. Which food patients should avoid will probably surprise you!
