
Research
Diagnosis & Imaging
February 10, 2025
Identifying Cervical Nerve Root Involvement Based on History Taking and Examination

Introduction
Identifying cervical nerve root involvement can be challenging due to an overlap of common signs and symptoms between different pathological conditions. Therefore, a good history taking and clinical examination are essential to raise the probability of a correct diagnosis. The use of standalone tests or patient information has shown low diagnostic value. (Mizer et al., 2017) It was therefore advocated to investigate the best way to diagnose cervical nerve root involvement in a patient presenting with features of cervical radicular pain and/or radiculopathy. Three separate models were developed and compared to determine how they establish an accurate diagnosis of cervical nerve root involvement.
Methods
The study used prospectively collected data to construct a diagnostic predictive modeling study from Sleijser-Koehorst et al., 2021. In the 2021 study, the diagnostic accuracy was determined for several items derived from the patient history taking and clinical examination separately. The current study we review today aimed to develop a diagnostic model and determine the clinical usefulness of a combination of items that achieved good diagnostic properties individually. Items from the 2021 study that achieved sensitivity or specificity values of at least 0.80 were selected for the development of the three predictive models.
These predictors included:
- Patient History model:
- Arm pain worse than neck pain
- Patient-reported Paresthesia
- Patient-reported Paresthesia and/or numbness
- Provocation of symptoms by ironing
- Reduction of symptoms by walking with hand in pocket
- Clinical Examination model
- Spurling Test
- Upper Limb Neurodynamic Test 1 (Median Nerve)
- Cervical Distraction Test
- Neurological Tests
- Sensation
- Reflexes
- Muscle Weakness
The third predictive model was the combination of the patient history model and the clinical examination model altogether.
To determine the diagnostic ability of the three models, each predictive model is compared to the reference (gold) standard. In this study, the authors used two criteria for the reference standard:
- A clinical diagnosis of cervical nerve root involvement made by a neurosurgeon
AND
- An MRI scan objectifying nerve root compression or irritation at the same or adjacent level that conforms with the clinical diagnosis (based on the dermatomal distribution)
The models were analyzed and the diagnostic accuracy was calculated by the Area Under the Curve (AUC). The AUC was interpreted as follows:
- AUC ≥ 0.9: outstanding diagnostic accuracy
- AUC 0.80 to 0.89: excellent diagnostic accuracy
- AUC 0.70 to 0.79: acceptable diagnostic accuracy
- AUC 0.51 to 0.69: poor diagnostic accuracy
- AUC = 0.5: no discriminatory value
Results
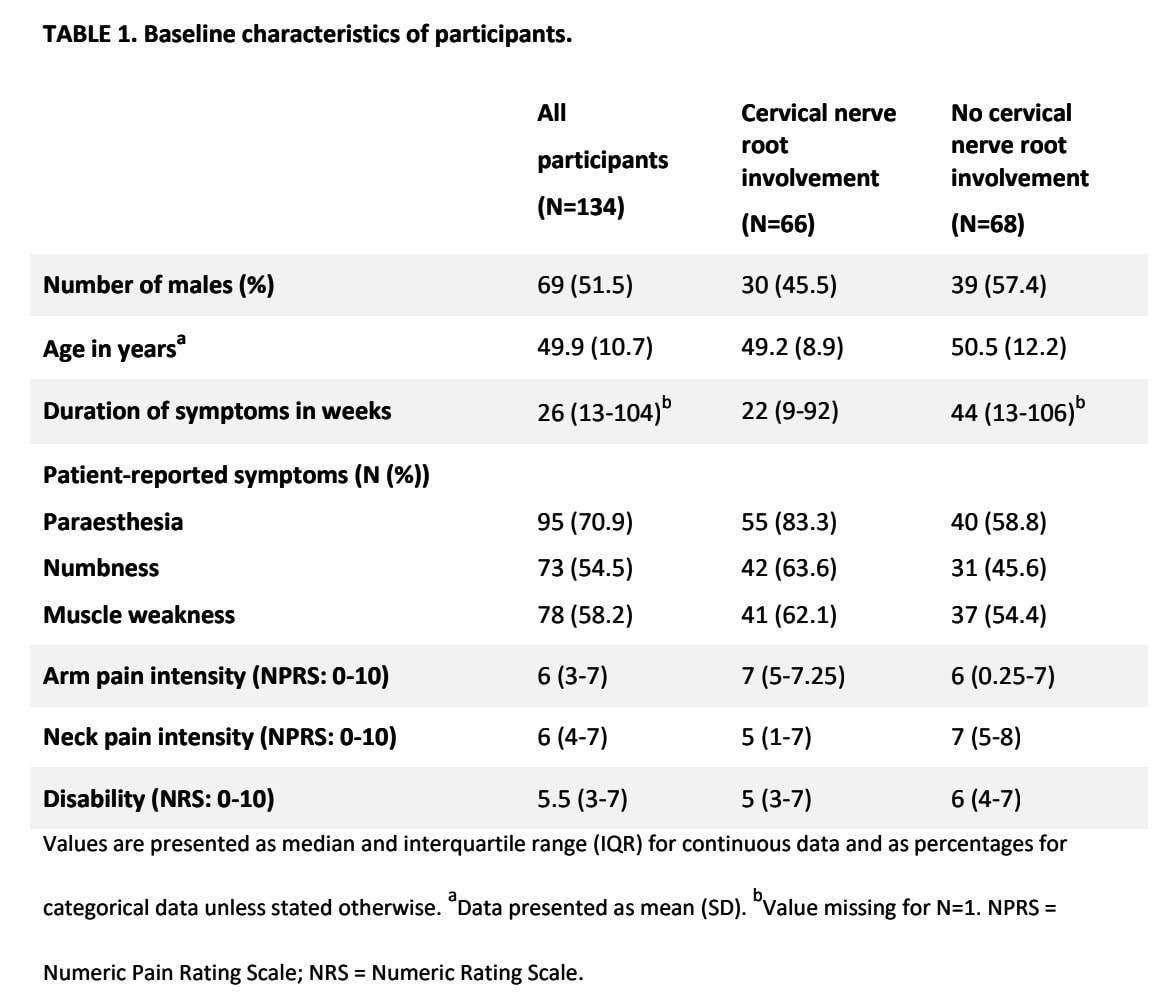
Hundred and thirty-four patients with suspected nerve root involvement were included in the study. The median symptom duration was 26 weeks and the sample had a mean age of 49.9 years. The population was almost equally divided into both sexes. In sixty-six patients a cervical nerve root involvement was identified by the reference standard and 68 had no cervical nerve root involvement based on the reference standard.
The multivariate regression analysis retained the following variables in the prediction models:
Patient History prediction model
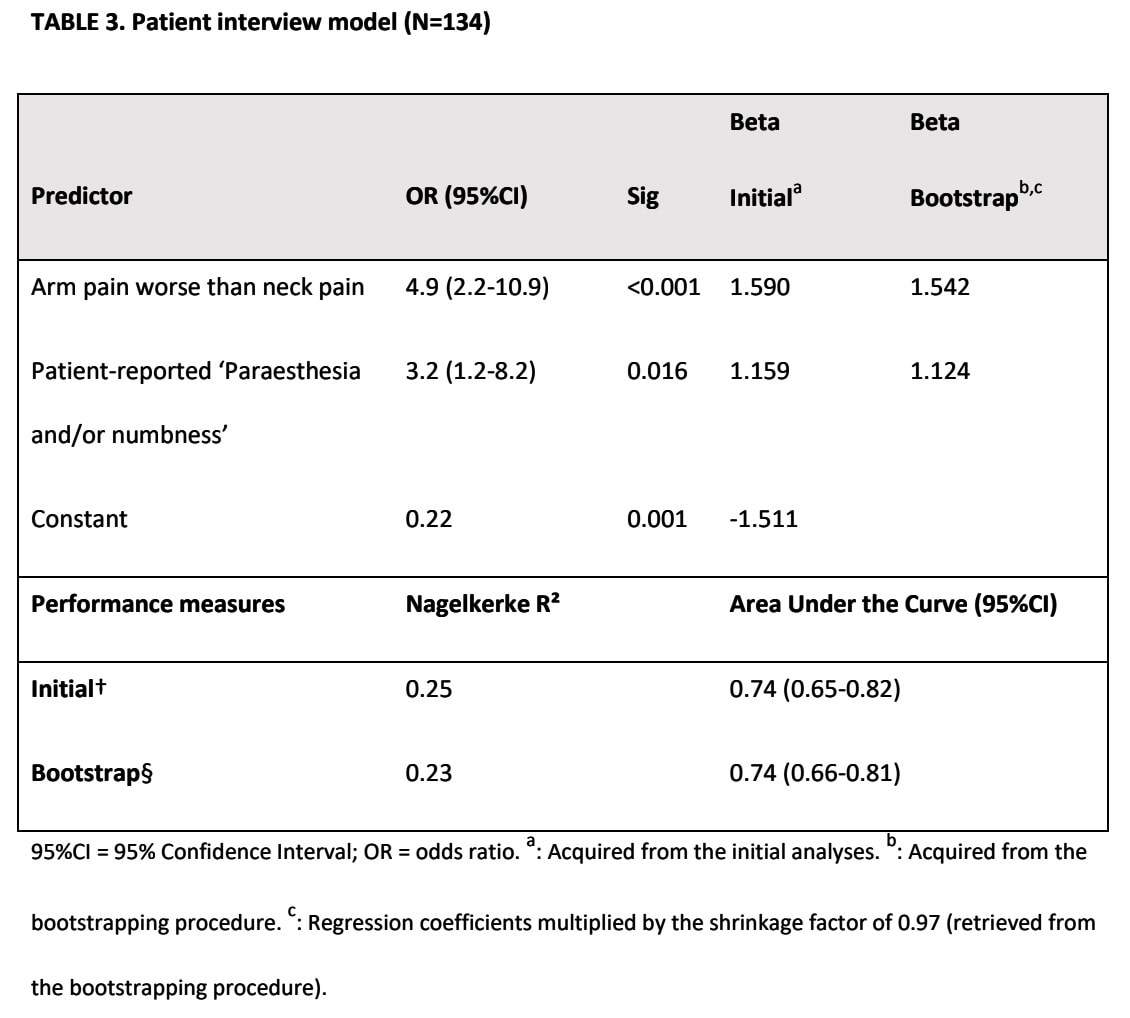
The predictors “arm pain worse than neck pain” and “patient-reported paresthesia and/or numbness” were retained in the patient history model. Together, they achieved an AUC of 0.74, indicating acceptable diagnostic accuracy.
Clinical Examination model
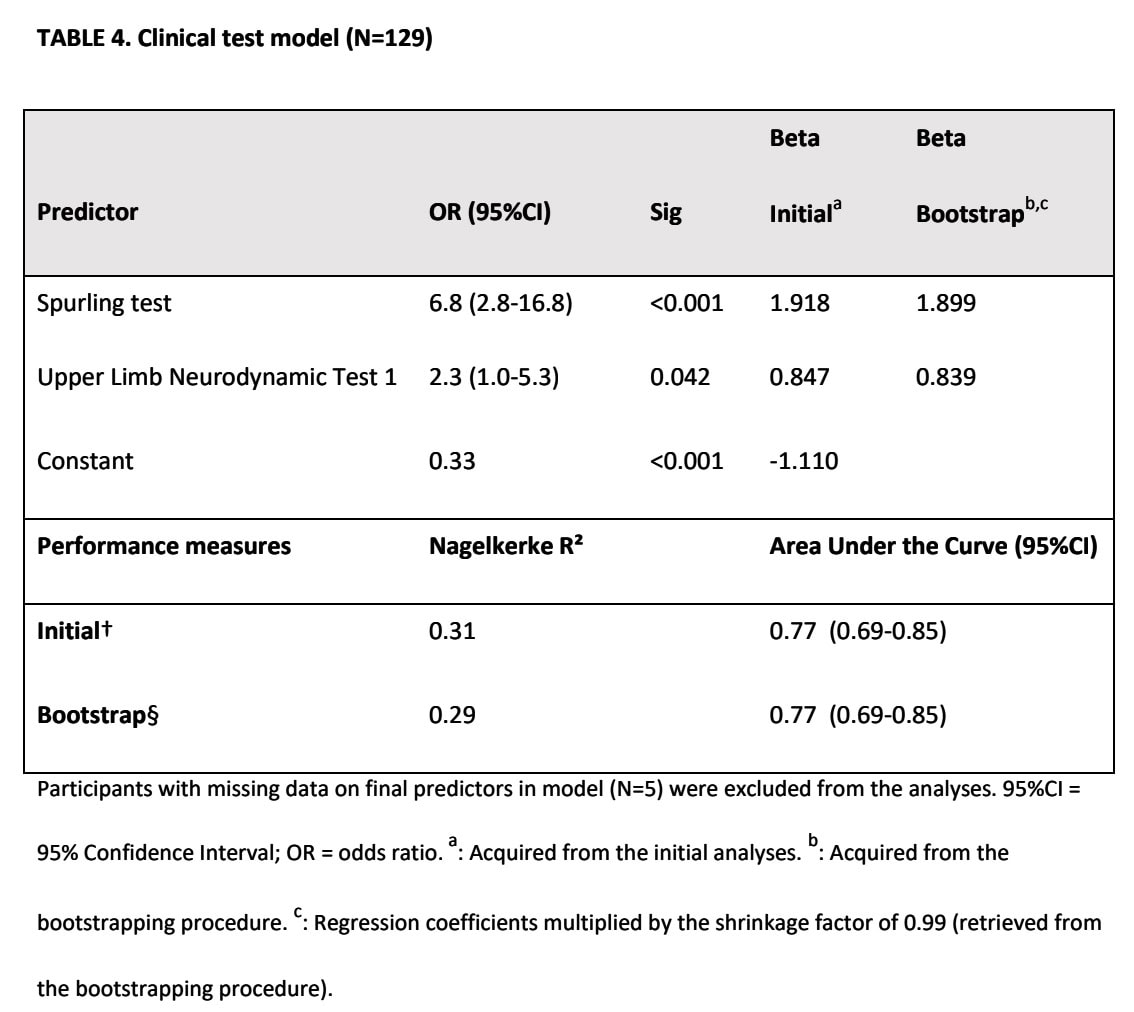
The Spurling test and the ULNT1 test were retained after the multivariate analysis. An AUC of 0.77 was calculated, indicative of acceptable diagnostic accuracy.
Combined model
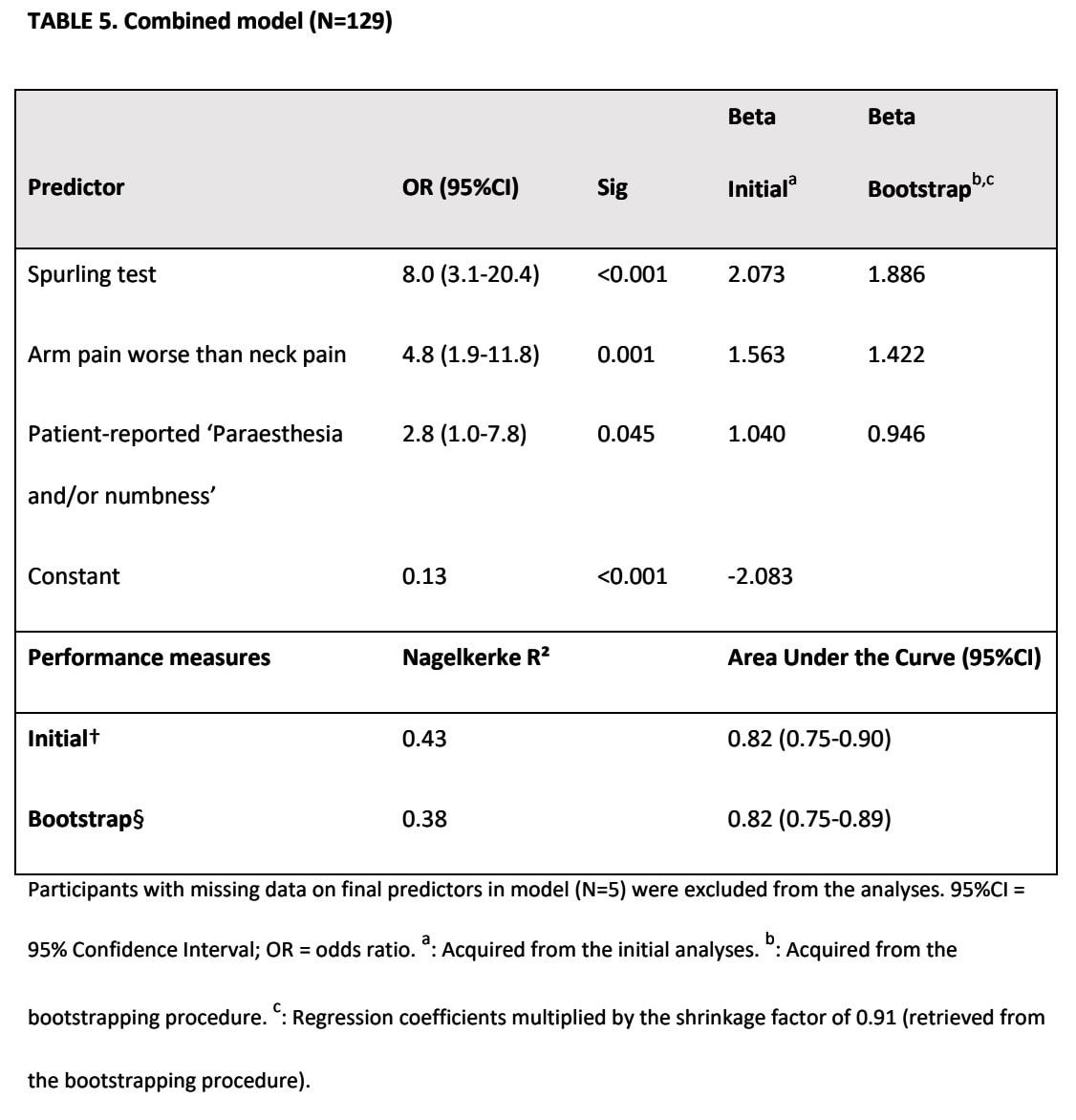
Three predictors were retained in the combination of the patient history model with the clinical examination findings model:
- Arm pain worse than neck pain
- Patient-reported presence of paresthesia and/or numbness
- Spurling test
This model had an AUC of 0.82, reflecting excellent diagnostic accuracy.
Questions and thoughts
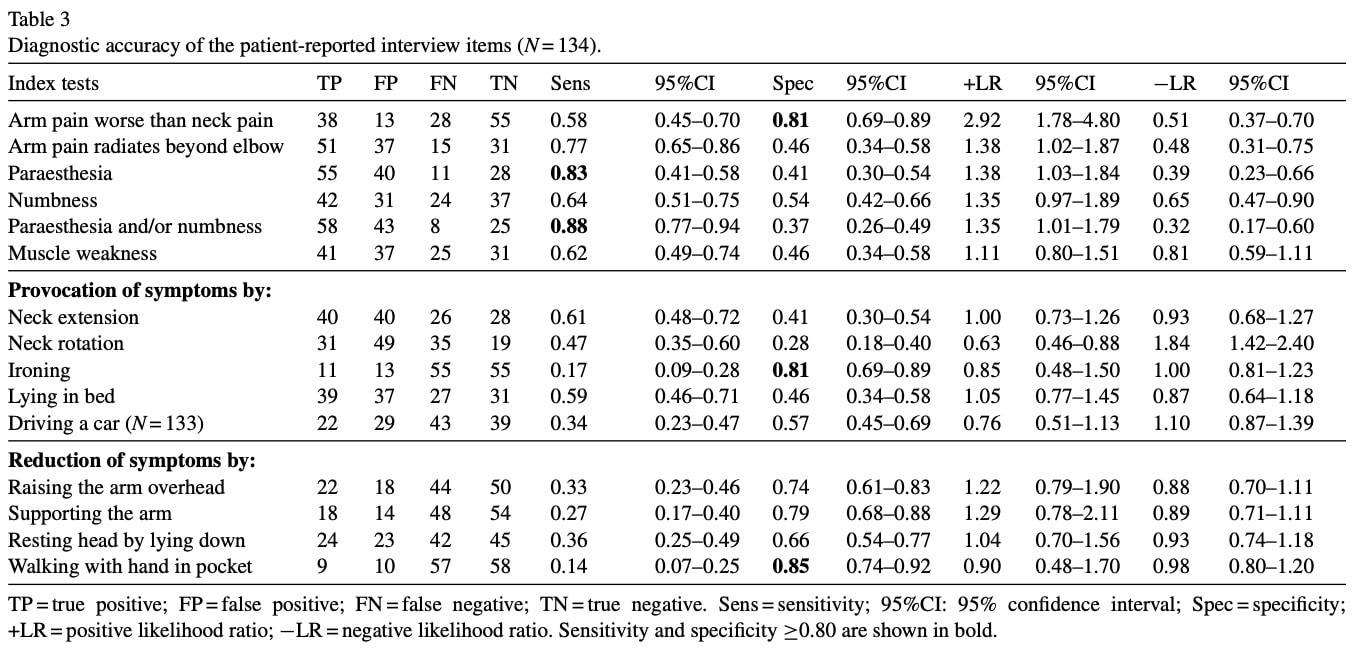
As there are yet several clinical prediction rules and clusters of tests examining the likelihood of cervical nerve root involvement (for example the Cluster of Wainner), at first glance, this study doesn’t add much new information. However, in the case of the Cluster of Wainner, information is obtained from clinical examination findings. We all know that a good clinical examination is paramount and the selection of accurate tests is imperative. Yet, these clusters can be useful for clinicians who are already experienced with pattern recognition of cervical nerve root involvement problems. For most novice and less experienced clinicians, it skips certain steps in the hypothetico-deductive clinical reasoning process. This study helps in recognizing certain signs and symptoms from the patient history taking and helps increase or decrease suspicion of cervical nerve root involvement. After all, “history taking is still the most important part of acquiring accurate medical data, knowing the patient, and establishing trust”. (Flugelman et al. 2021) Differential diagnosis requires establishing a set of hypotheses some of which must be excluded and others confirmed and to come to these hypotheses, you should be able to identify which information can be derived from the patient interview. As the current data was collected from an earlier study by the same author (Sleijser-Koehorst et al. 2021), you can take a look at the underlying table, where different patient-reported interview items might help you get clues about when to think of possible cervical nerve root involvement.
Note that the confidence intervals are wide for most of the underlying signs. The patient presentation can demonstrate huge differences and this is not a limitative list as there are many overlapping symptoms with other pathologies. Also, certain signs from the patient interview were selected based on diagnostic superiority, and these were further analyzed and refined by the 2025 study.
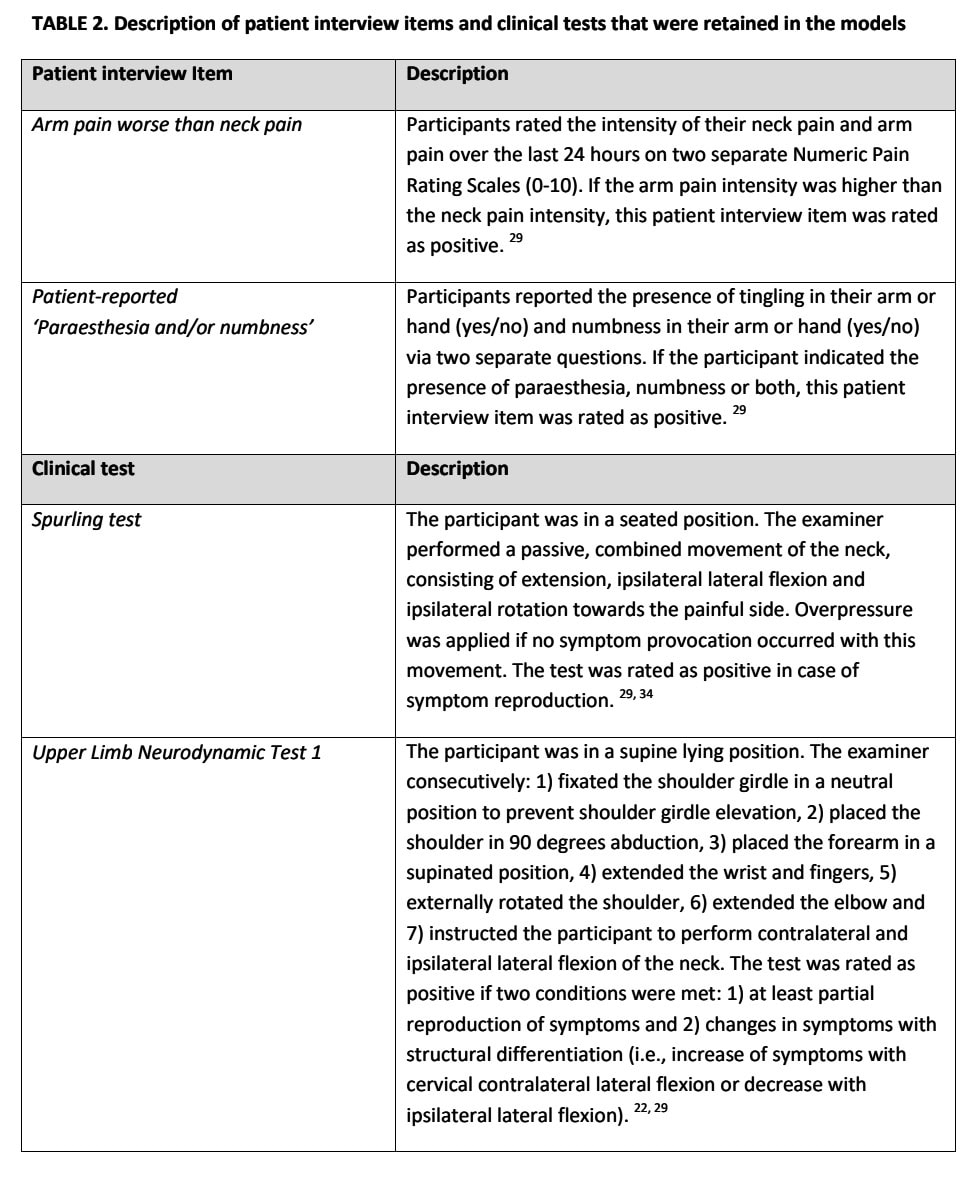
It is very important to sufficiently understand the exact description of history-taking information and clinical test execution and interpretation. Table 2 here describes the way the authors interpreted the clues from history taking and clinical examination.
Talk nerdy to me
The authors selected patient history findings from their 2021 study that showed sensitivity and specificity of at least 0.80 for identifying cervical nerve root involvement, although for the clinical examination findings tests below the 0.80 accuracy threshold were also included, but no rationale was provided.
The combined model achieved the best diagnostic accuracy. This means that using a positive Spurling test, together with patient-reported arm pain worse than neck pain and symptoms of paresthesia and/or numbness, gives the best accuracy to recognize a cervical nerve root involvement. However, the explained variance was low: 0.38. If the explained variance is low, it means a lot of other unknown factors are influencing the diagnosis that the model isn’t capturing. This means that, although the combined model does a great job in telling us who has nerve root involvement with confidence, it is not a perfect model.
Even the best model only explained 38% of the variation in diagnoses. This tells us:
- The model is useful but not perfect, implying that other factors likely play a role in diagnosing this condition.
- Clinical judgment is still important—a physiotherapist or doctor can’t rely only on this model alone but rather should use it as one tool among others in their decision-making.
Diagnosing cervical nerve root involvement isn’t 100% predictable from interviews or clinical tests alone. Some patients may have clear symptoms but no nerve compression. Others might have a positive clinical test but don’t have the condition. There might be differences between examiners conducting the tests, or patients might use other wording to describe their symptoms or there might be differences in how the patient’s response is interpreted. Yet, this study had only one examiner performing the clinical examination tests, so the variance in the results can not be coming from differences between examiners.
To conclude, although not a perfect tool was developed, the use of a combination of patient history, clinical tests, and possibly imaging (like MRI) might be better for identifying cervical nerve root involvement, compared to standalone tests, history findings, or solely based upon MRI scans.
The authors have designed a rigorous study protocol, including adequate blinding, no delay between the assessment of the tests and the comparison with the reference standard which avoids disease progression/regression bias, and no treatment in between the testing and imaging, so we can raise our hats. The only aspect you should bear in mind is to carefully determine whether the prevalence of 49% (reflecting thus the pre-test probability) is generalizable to your clinical practice.
Take-home messages
Using the presence of patient-reported paresthesia and/or numbness, the finding of arm pain that is worse than neck pain and a positive Spurling test as predictors for identifying cervical nerve root involvement reached the threshold for excellent diagnostic accuracy. External validation of the current model is still necessary, especially since the best predictive model could only explain 38% of the variance. The current study helps in hypothetico-deductive reasoning.
Reference
Learn more
21 OF THE MOST USEFUL ORTHOPAEDIC TESTS IN CLINICAL PRACTICE
We have comprised a 100% Free E-Book containing 21 of the hands-down most useful orthopedic tests per body region guaranteed to help you reach a proper diagnosis today!
