
Research
Ankle/Foot
May 1, 2025
Achilles Tendinopathy Diagnosis: Key Domains, Red Flags & Differential Diagnoses.

Introduction
Achilles tendinopathy diagnosis has traditionally relied on pathoanatomical findings, including imaging and histology, alongside validated physical examination and clinical tests. However, structural tendon abnormalities do not always correlate with pain, raising questions about the validity of a purely tissue-based diagnostic approach. Despite the continued prominence of this model among clinicians and researchers, there remains a need to standardize assessment criteria for posterior ankle pain—particularly to distinguish tendinopathy from other conditions and identify cases requiring medical intervention.
This Delphi consensus study aimed to establish expert agreement on three critical aspects of Achilles tendinopathy diagnosis:
- Key diagnostic criteria – Defining essential clinical features,
- Differential diagnoses – Distinguishing tendinopathy from other causes of posterior ankle pain,
- ‘Red flags’ – Identifying signs warranting further medical evaluation.
Methods
Let’s first define what a Delphi consensus study is. A Delphi study is a structured method used to gather expert opinions and achieve consensus on a topic when definitive evidence is lacking. It’s especially useful in healthcare for developing guidelines, treatment protocols, or defining best practices.
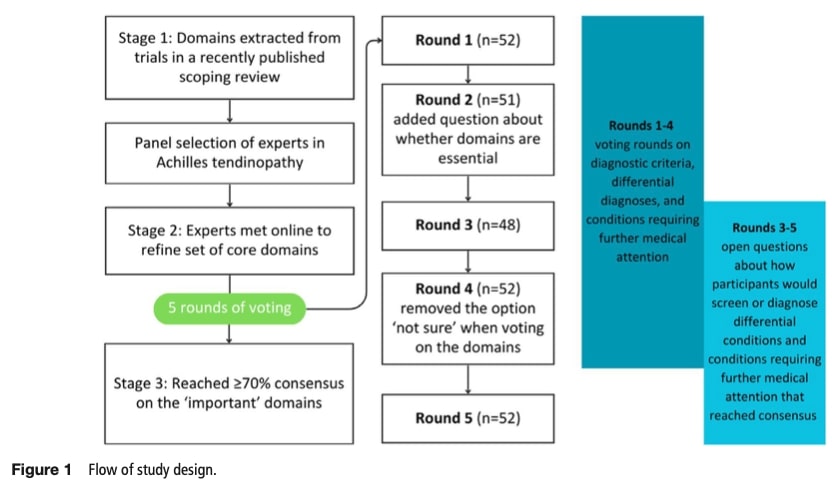
Researchers conducted an online Delphi survey involving four rounds of discussion focused on diagnostic domains, differential diagnoses, and conditions requiring medical attention in Achilles tendinopathy. Health professionals with clinical or research expertise in Achilles tendinopathy were recruited through multiple channels: International Olympic Committees, Expertscape’s database, and snowball sampling. While aiming for 50-60 participants, they prioritized diverse representation across gender, professional disciplines, and geographical regions. As this study focused on diagnostic criteria requiring clinical expertise, they exclusively recruited healthcare professionals and researchers without patient involvement.
Stage 1: identifying diagnostic domains and criteria, differential diagnostic conditions and conditions requiring further medical attention
Diagnostic domains were broad categories (e.g., pain history or clinical tests), while diagnostic criteria were specific details within those domains (e.g., gradual pain onset or mid-tendon tenderness).
Researchers identified diagnostic categories (e.g., pain patterns) and specific exam criteria (e.g., tender spots) from published Achilles review, while compiling differential diagnoses and red flags from guidelines. Experts could suggest additional items during initial rounds.
Stage 2: generation of survey questions
Participants rated the importance of each diagnostic domains element for midportion, insertional, or both tendon subtypes. They were presented with diagnostic domains and were asked to evaluate for importance of Achilles tendinopathy using fives responses options: relevance to midportion tendinopathy, insertional tendinopathy, both, neither, or unsure (with the “unsure” option removed in the final round as per Delphi methodology). Over five survey rounds, they progressively refined criteria through structured voting and open-ended feedback, with imaging use specifically debated (e.g., “Does normal imaging rule out tendinopathy?”).
Questions on differential diagnosis and conditions requiring further medical attention
Participants evaluated whether each proposed condition should serve as: (1) a differential diagnosis for Achilles tendinopathy, or (2) a medical referral indicator. They specified relevance to midportion, insertional, or both tendon subtypes using structured responses (“yes/no/unsure”), with “unsure” removed in the final round. In later rounds (3-5), experts provided open-text details about: (a) clinical scenarios warranting consideration of these conditions, and (b) specific diagnostic methods (history, exams, imaging) to identify them.
Stage 3: the five survey rounds
Items reaching 70% agreement were locked in early, while remaining elements underwent further discussion. Final rounds addressed remaining unresolved items and focused on practical application – exactly when and how to identify complicating factors through history, exams, or imaging.
Data analysis
Participant characteristics and responses were analyzed descriptively using frequencies and percentages with IBM SPSS Statistics (v29). For qualitative data from open-text responses, researchers conducted inductive content analysis. Differential diagnosis and medical referral suggestions were additionally analyzed through deductive coding into four predefined categories: history, physical examination, imaging, and other.
The coding process followed three stages:
- Preparation: Compiling responses in Excel
- Organization: Independent coding by two researchers (PM/VK/JB) with cross-verification
- Reporting: Presenting categorized results with representative quotes
Results
Participants
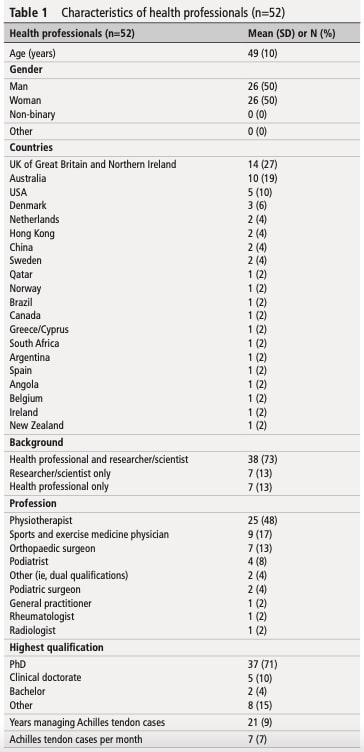
Among 59 invited experts, 52 (88%) participated in at least one voting round, with full attendance in rounds 1, 4, and 5. The cohort comprised equal gender representation, primarily physiotherapists (48%), sports medicine specialists (17%), and orthopedic surgeons (13%), with an average of 21 years’ experience in Achilles tendinopathy management. Minor attrition in rounds 2 (n=51) and 3 (n=48) resulted from scheduling conflicts.
Diagnostic domains and criteria
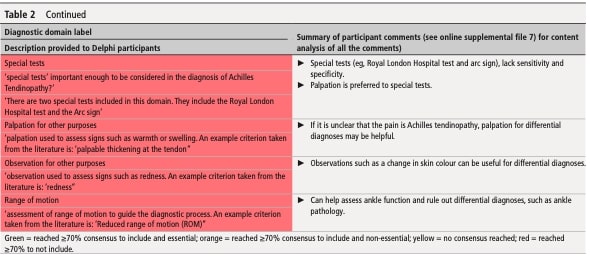
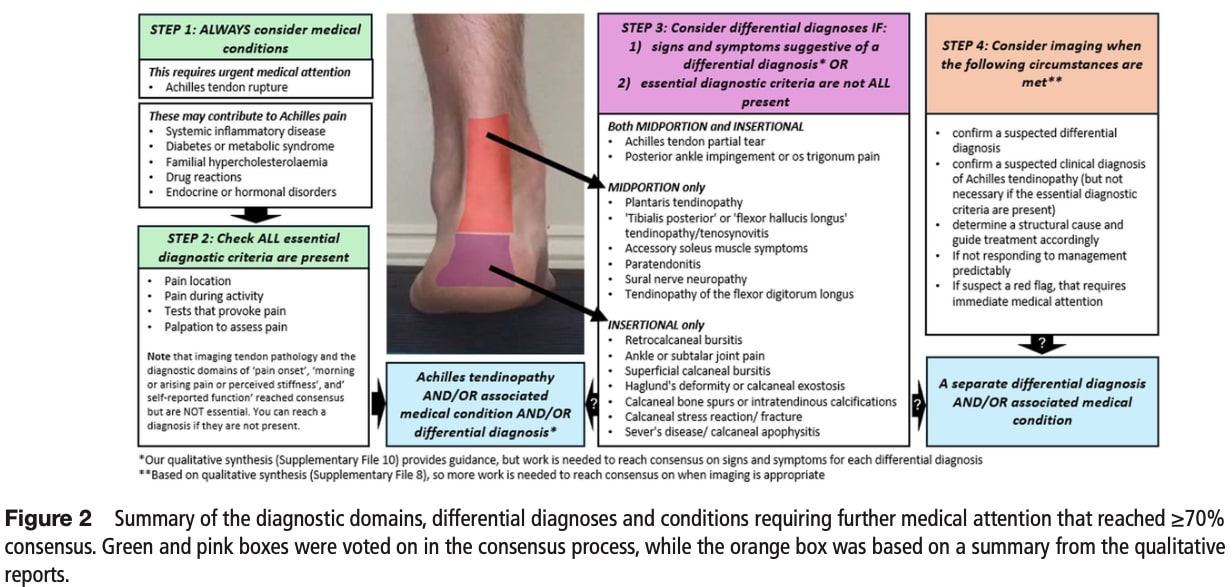
Seven diagnostic domains reached consensus (>70% agreement) as essential for Achilles tendinopathy diagnosis: pain location, pain during activity, pain-provoking clinical tests, and tenderness on palpation. In contrast, self-reported function, morning pain or stiffness, and pain onset patterns were excluded as non-essential criteria. Additionally, four domains—stiffness location, pain behavior, pain at rest or after inactivity, and special tests—were explicitly not recommended for diagnostic use.
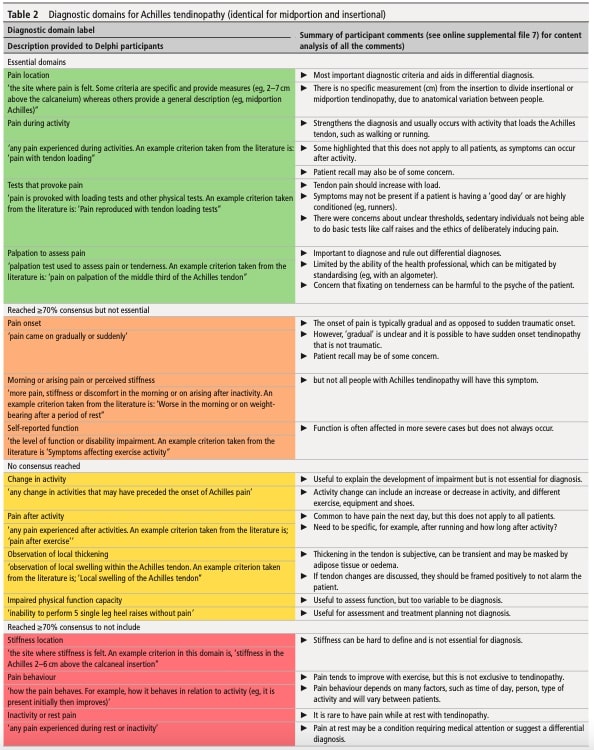
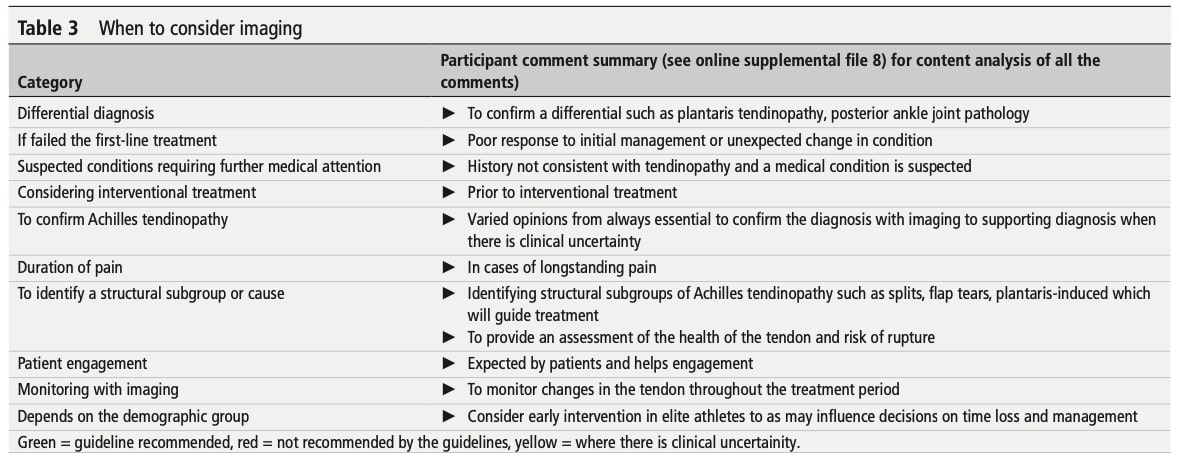
Use of imaging for Achilles tendinopathy diagnosis
While imaging achieved >70% consensus for inclusion in Achilles tendinopathy diagnosis, it was not deemed essential. Key disagreements emerged regarding whether normal imaging reliably excludes tendinopathy. Proponents argued that symptomatic cases with normal imaging are “exceptionally rare,” suggesting strong clinical-imaging correlation. Opponents countered that false negatives may stem from: (1) modality sensitivity limitations, (2) early disease stages, or (3) inconsistent definitions of “normal” tendon imaging.
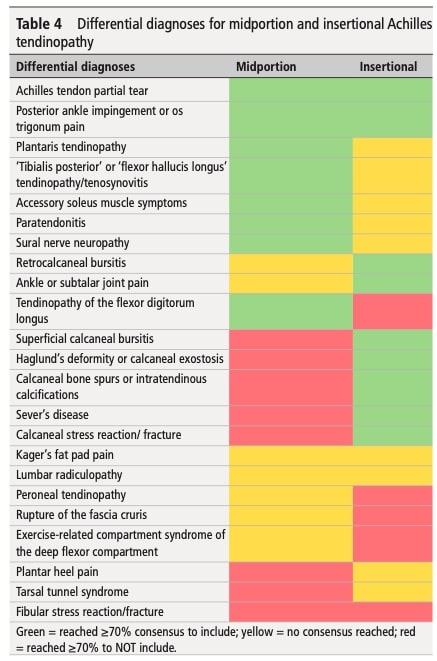
Differential diagnosis
Fifteen differential diagnoses achieved >70% expert consensus, categorized by pathoanatomical location. Differential diagnoses are presented in Table 4.
Conditions requiring further medical attention
Experts agreed (≥70% consensus) that the following six conditions must be ruled out during assessment of all Achilles tendinopathy cases. Diagnoses requiring further medical investigation are presented in Table 5.
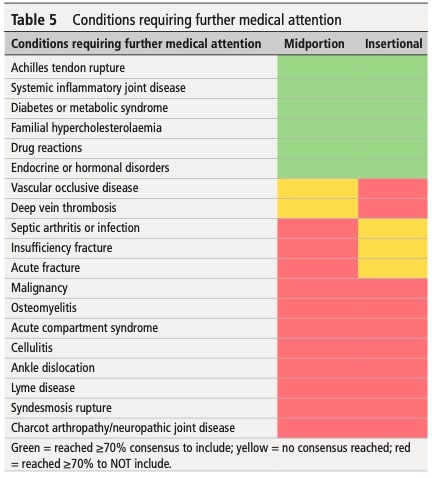
To screen for conditions requiring further medical attention, experts used most frequently medical history (family, medications, obesity) and blood tests. Imaging was reserved for suspected Achilles ruptures (US/MRI).
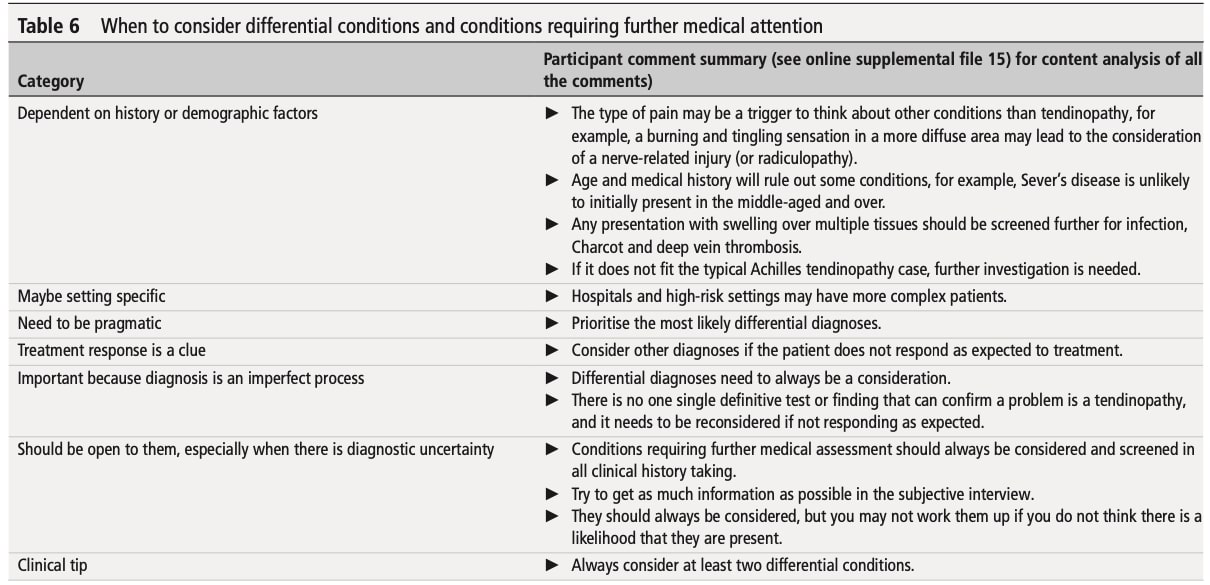
When to consider differential conditions and conditions requiring further medical investigations.
Experts recommended expanding differential diagnoses when facing unclear cases or poor treatment response, emphasizing thorough history-taking (medications, family history) and risk-specific assessments (e.g., insufficiency fractures in postmenopausal women, Sever’s disease in children). Table 6 provides additional evaluation criteria for differential diagnoses requiring medical attention.
Questions and thoughts
Although this Delphi consensus did not establish lumbar radiculopathy as a formal differential diagnosis for Achilles tendinopathy (Table 4), clinicians should remain alert to its potential contribution to Achilles-region symptoms. Emerging evidence demonstrates that lumbar spine dysfunction frequently refers pain to the lower extremity. Given the distinct management pathways and typically faster progression of lumbar-related pain compared to local tendinopathy, incorporating neurological screening—including spinal assessment, neurodynamic testing, and repetitive movement testing—may be clinically warranted for refractory cases.
This study primarily focused on pathoanatomical diagnostic criteria, which inherently emphasizes nociceptive pain mechanisms. However, the absence of discussion regarding central nervous system contributions represents a critical gap, particularly for chronic tendinopathy cases. Central sensitization—a maladaptive amplification of neural signaling—may underlie persistent pain in some patients, even after tissue healing.
Talk nerdy to me
Quantitative data, including participant characteristics and survey responses, were analyzed descriptively using IBM SPSS Statistics (v29), with results reported as frequencies and percentages. For qualitative data from open-text responses, the researchers employed two complementary analytical approaches.
Inductive content analysis was used to synthesize unstructured text responses. This exploratory method involved systematically reviewing participant comments to identify naturally emerging themes, which were then grouped into subcategories and broader categories. The inductive approach allowed themes to arise organically from the data without being constrained by predetermined frameworks, providing insights into experts’ unconstrained perspectives.
For analysis of differential diagnoses and conditions requiring medical attention, the researchers applied deductive coding using a predefined clinical framework. Responses were categorized into: (1) history, (2) physical examination, (3) imaging, and (4) other. This structured approach ensured consistent classification of clinically relevant screening practices. The coding process followed three rigorous stages: preparation (data compilation in Excel), organization (dual independent coding by researchers with verification), and reporting (presentation of categorized results with representative quotes).
To ensure methodological rigor, the coders immersed themselves in the data through repeated review and reflective discussion. Only one analyst participated in the Delphi voting to maintain analytical independence and minimize potential bias in the qualitative interpretation. This combination of inductive and deductive methods provided both exploratory insights and standardized clinical classifications.
Take home messages
1. Safety First: Screening & Red Flags
- Always assess for red flags (e.g., systemic conditions, infections, ruptures) using a continuum of concern.
- Screen for lumbar referred pain and evaluate symptom modulation patterns (e.g., mechanical vs. persistent pain).
2. Core Diagnostic Criteria (Expert Consensus) Four key findings support Achilles tendinopathy diagnosis:
- Pain location (midportion or insertional)
- Pain during/after activity
- Positive provocation tests (e.g., tendon loading reproduces pain)
- Local tenderness on palpation
3. Targeted Use of Imaging
Reserve clinical imaging (US/MRI) for:
- Atypical presentations (poor response to treatment)
- Monitoring structural changes (e.g., tear progression, healing)
4. Managing non-responders
If progress stalls, broaden assessment to:
- Re-evaluate red flags (missed diagnoses)
- Assess central sensitization (e.g., allodynia, widespread sensitivity)
- Address biopsychosocial factors (e.g., load management, fear-avoidance,metabolic health)
To treat Achilles tendinopathy, use Achilles tendon loading strategies as a first-line approach.
- This blog article provides an in-depth exploration of Achilles tendinopathy rehabilitation.
- This review article offers evidence-based insights on Achilles tendon exercise progression.
Reference
LEARN TO OPTIMIZE REHAB & RTS DECISION MAKING AFTER ACL RECONSTRUCTION
Sign up for this FREE webinar and top leading expert in ACL rehab Bart Dingenen will show you exactly how you can do better in ACL rehab and return to sport decision making
