
Research
Hip
May 4, 2026
Hip Abductor Function After Gluteal Tendon Reconstruction: Recovery Benchmarks From a Prospective Cohort and Matched Healthy Controls

Introduction
The Gluteus medius and minimus muscles are important for hip abductor function and gait efficiency. Ruptures of their tendons are increasingly recognized as contributors to lateral hip pain and functional limitations such as a Trendelenburg gait. While function can be seriously compromised, requiring surgery to repair the damaged tendons, the literature lacks objective, reliable data on hip abductor strength before and after surgical procedures. Most reports relied on subjective grading systems like the MRC scale, limiting reproducibility. Additionally, while surgical repair aims to restore tendon integrity, it is unclear whether this translates into meaningful muscle function recovery and if tear severity influences outcomes. This study addresses these gaps by providing objective dynamometer-based strength data from before and 1 year post-surgical reconstruction. As a secondary aim, functional outcomes and prognostic factors are explored.
Methods
A prospective cohort study, following the STROBE guidelines, was conducted between 2018 and 2023. Female participants with MRI-confirmed gluteal tendon tears were followed from before their surgery (baseline) to 12 months post-operatively. Gluteus medius tendon tears with or without a gluteus minimus tear were eligible. Women with isolated gluteus minimus tendon tears were excluded from the study. Only participants who underwent open surgical repair of the tendon were included, so besides the tendon repair, no additional surgery was performed. Twenty-four age-matched healthy women were included as controls.
Surgical Procedure
The surgery was performed using an open repair via a direct lateral approach. The tendon tears were anatomically reattached using bone anchors. The surgeons classified the tears intraoperatively using Horsens classification into full-thickness and partial-thickness tears.
Postoperative Rehabilitation
Phase 1 (0–6 weeks):
Discharge from the hospital was typically on the day of the operation. The patients were allowed ambulation with 20 kg partial weight-bearing using crutches in the first 6 weeks. Active abduction or adduction was prohibited. During these first 6 weeks, the patient performed non-weight-bearing home exercises for edema control and light activation.
Phase 2 (6–12 weeks):
In this second phase, progression to full weight-bearing was gradually achieved, when gait pattern was normalized. Rehabilitation was outsourced by the patient’s local physiotherapy clinic, following a protocol prescribed and overseen by a specialized physiotherapist from the surgical center. In this phase, progressions were more individualized and supervised by a local physiotherapist.
Phase 3 (+12 weeks):
From 12 weeks onward, rehabilitation was largely self-managed, with no structured physiotherapy supervision reported until the 1-year follow-up.
Outcome Measures
- Maximal isometric hip abduction strength was measured using a handheld dynamometer according to a standardized protocol (Kemp et al. 2013). Three trials were performed, with the best recorded. Standardized markings ensured consistent dynamometer placement and moment arm measurement. Moment arm length was measured from the joint axis of rotation to the point of application of the force transducer for each test. For hip abduction strength, the force transducer was applied distally on the lateral lower leg, 5 cm proximal to the lateral malleolus, with the moment arm measured from the greater trochanter to this point. For each test, torque was calculated by multiplying the force (measured in Newtons (N) by the length of the moment arm measured in metres (m), and then the data were normalized for body weight (measured in kilograms (kg) to express the value in Nm/kg. All tests were conducted bilaterally. The minimal clinically important difference was not mentioned specifically.
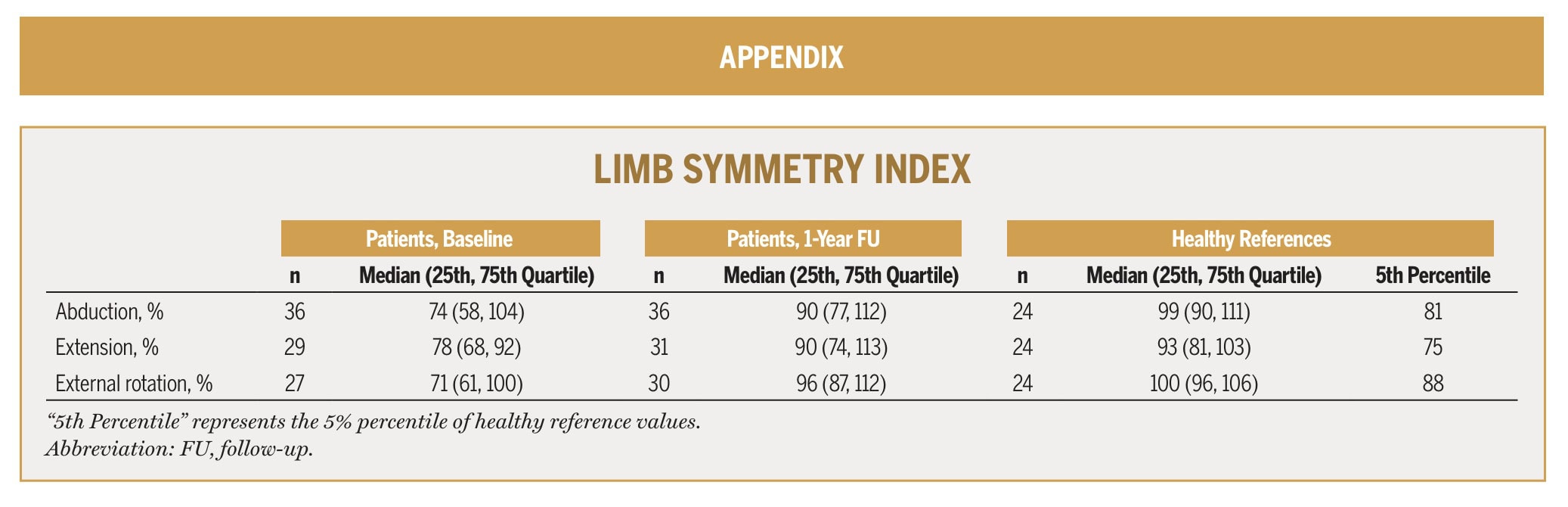
- Limb Symmetry Index (LSI) was calculated from absolute strength measurements during the isometric testing. The affected limb strength was divided by the contralateral leg’s strength and multiplied by 100.
- The Trendelenburg Sign was performed to assess hip abductor function. The patient stood on one leg for 30 seconds, and the assessor, standing behind the patient, placed his hands on the iliac crests to observe for pelvic drop on either side. A positive test was a pelvic drop on the contralateral side, below the horizontal line between both iliac crests.
- Patient-reported outcomes included
- Average lateral hip pain (NRS) during the last 14 days at rest, during activities of daily living, and at worst pain.
- Hip function, measured by the Copenhagen Hip and Groin Outcome Score (HAGOS)
Results
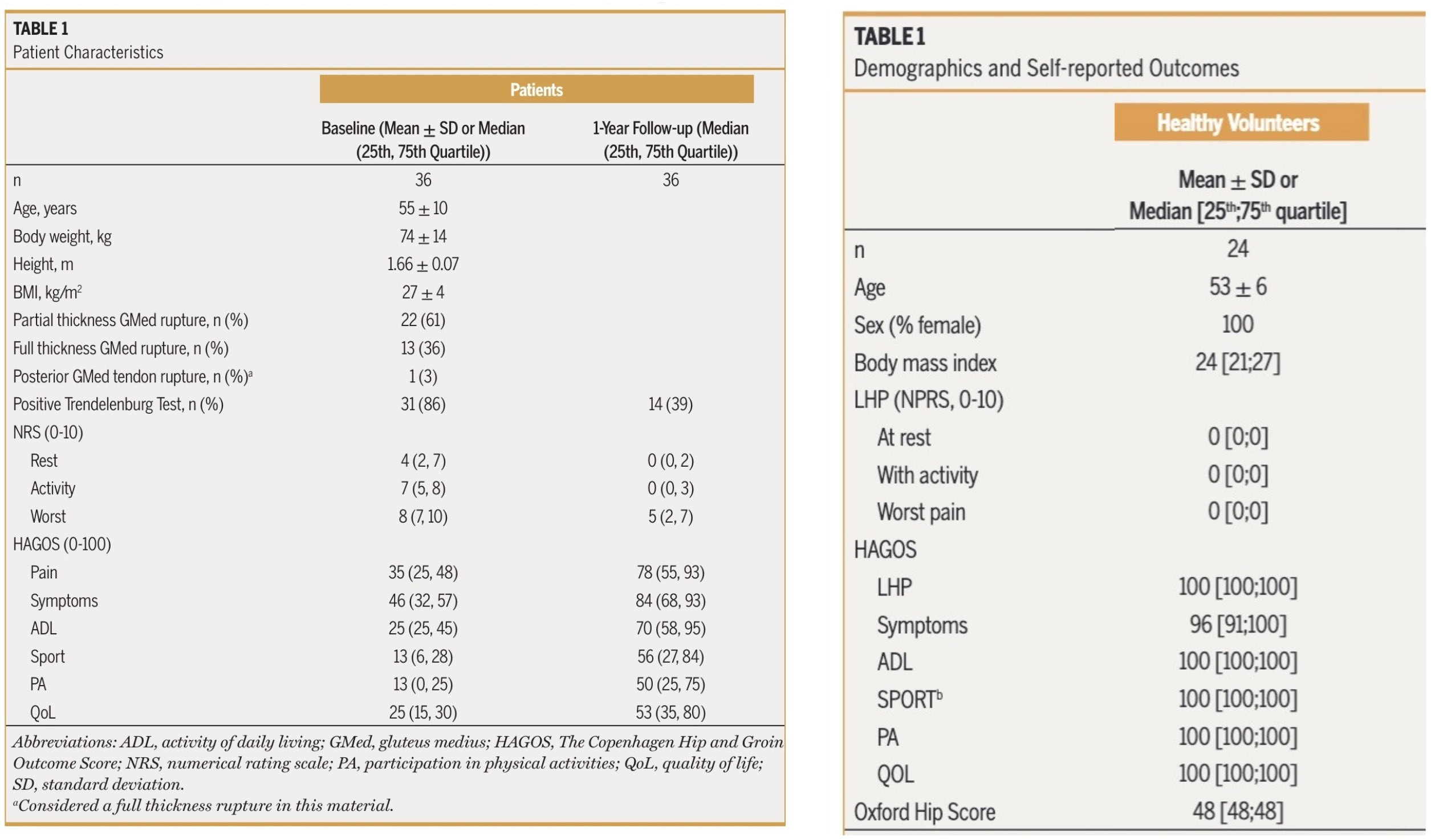
Thirty-six patients and 24 healthy controls were included.
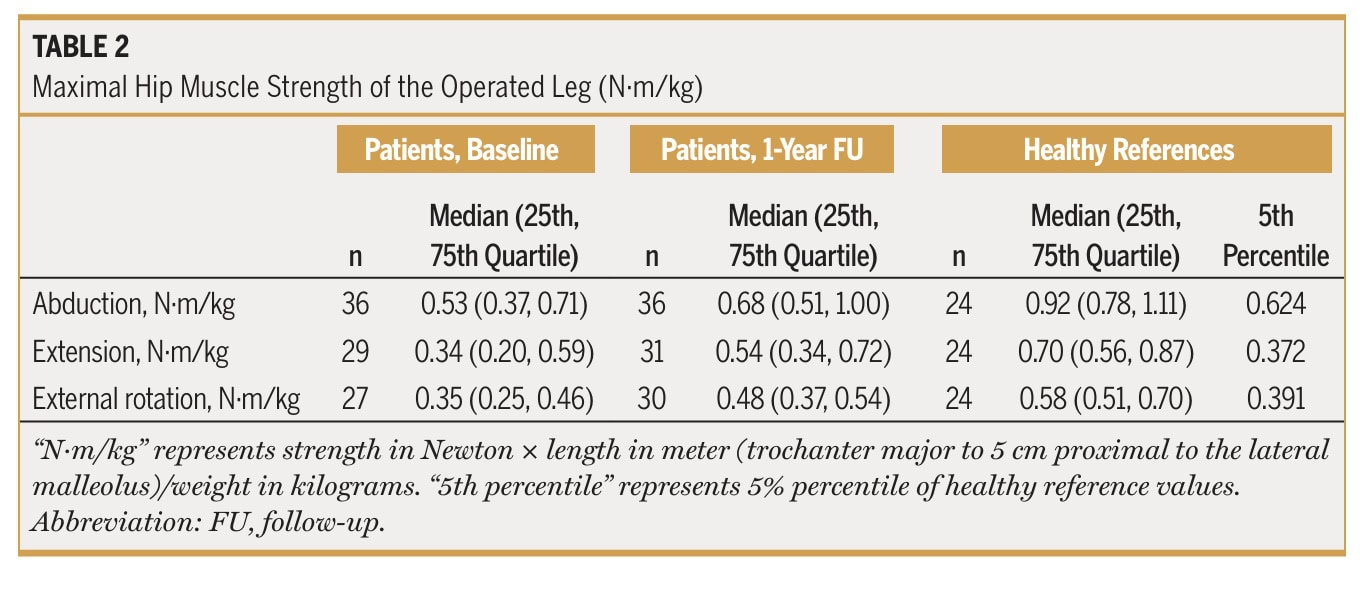
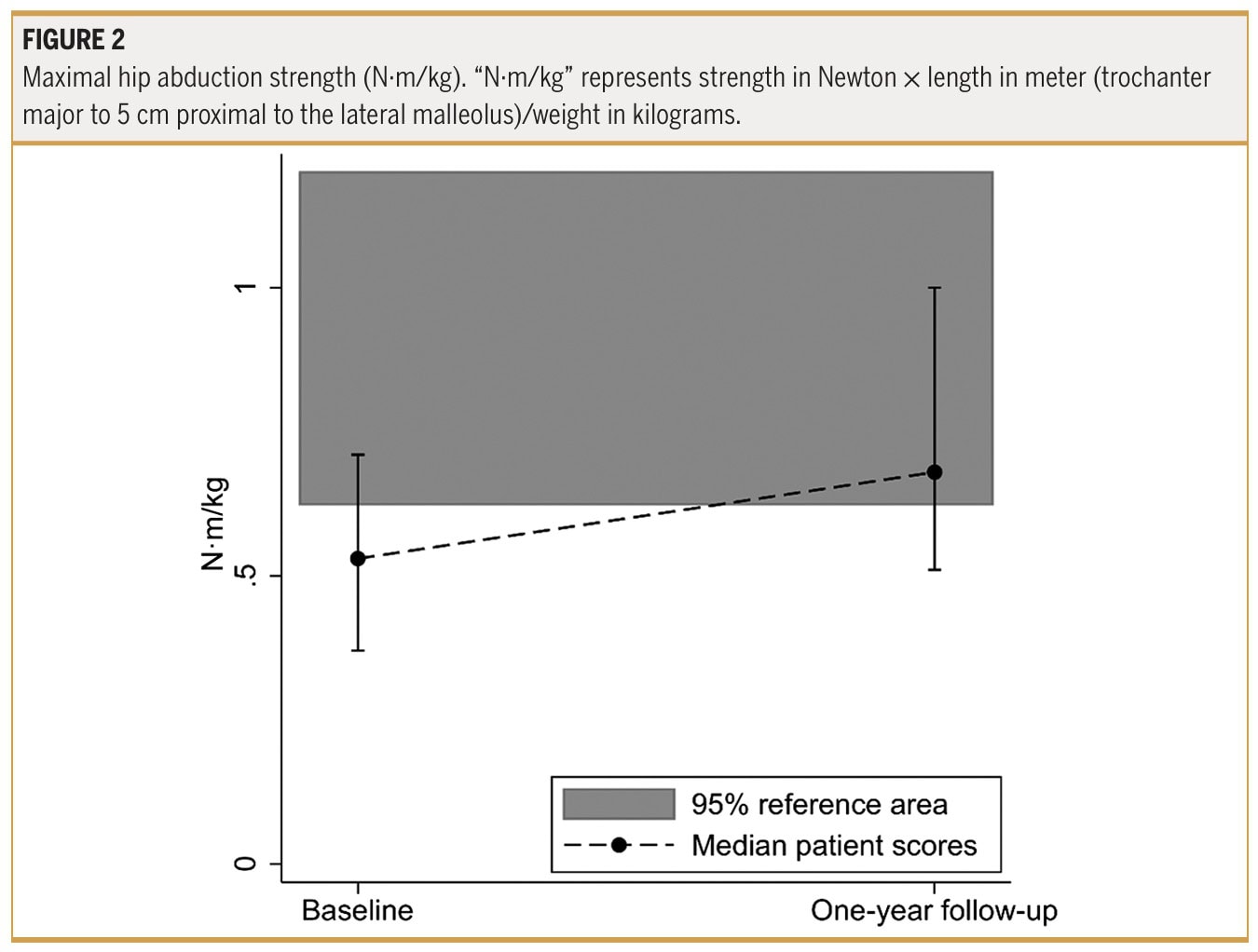
Data from strength testing revealed that patients increased their maximal hip abduction strength of the operated hip 1 year after gluteal tendon reconstruction.
The authors noted that at 1 year following the surgery, 61% reached the 95% reference interval of maximal abduction strength.
Furthermore, they stated that 69% of patients reached the healthy reference level of abduction strength symmetry at the 1-year follow-up.
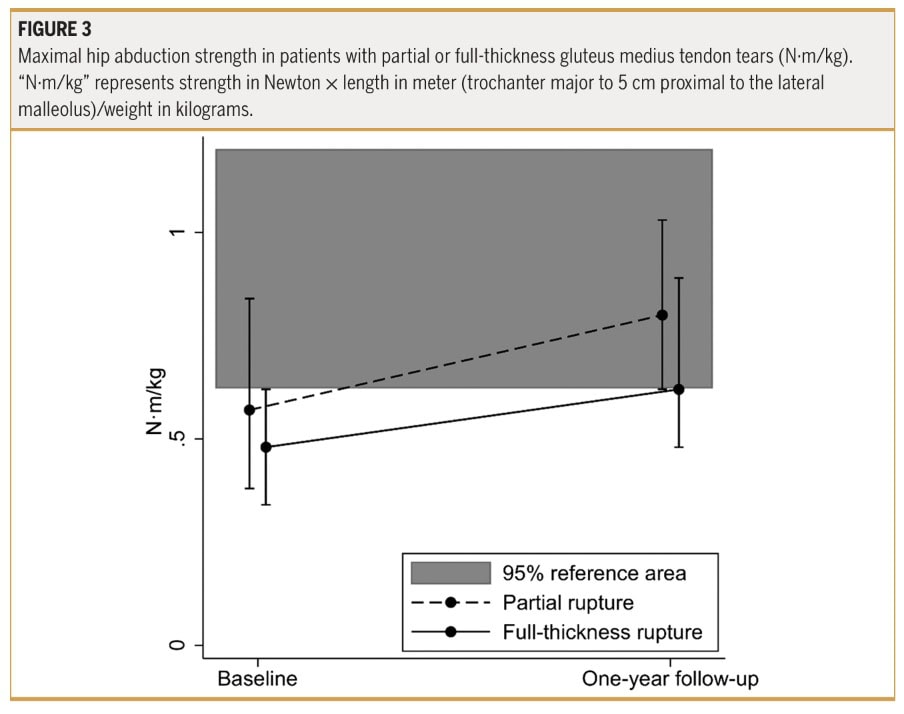
When taking a closer look at patients with partial versus full-thickness gluteal tendon rupture, the authors reported a “tendency for patients with a full-thickness rupture to have lower strength than those with a partial rupture.” Yet, this is a non-significant finding. However, they reported that 73% of those with a partial rupture reached healthy reference levels of hip abduction strength, whereas only 46% of those with a full-thickness rupture did.
When assessing the association between strength recovery and function, as measured by the Trendelenburg sign, it was noted that those with a positive Trendelenburg sign at the 1-year follow-up had a significantly lower maximal hip abduction strength than those with a negative test (0.51 [0.42, 0.95] Nm/kg vs 0.80 [0.64, 1.06] Nm/kg, P = .021).
Questions and thoughts
The data we obtain from this prospective cohort study can help inform our prognosis after surgery, and contains important information about which strength values can be considered normal or pathological. We can also derive the expected strength recovery timelines from such studies, especially when our patient has comparable characteristics to those in this cohort study. Although there was no significant difference in strength recuperation between participants with partial- versus full-thickness gluteal tendon tears after reconstruction, recovery of hip abduction function might be somewhat slower in some. The authors describe a “tendency” for full-thickness gluteal tendon tears to recover more slowly in terms of force output after surgical reconstruction. Indeed, inspection of Figure 3 shows that those with a partial tear are more rapidly progressing to the 95% reference area, the authors defined as “normal strength” values, while those with full-thickness gluteal tendon tears appear to only approach this reference area around 1 year post-operative. So this information helps us steer patient expectations, inform prognosis, and set realistic long-term goals.
The authors expressed the isometric force in Nm/kg to standardize outcomes according to the participant’s moment arm length and body weight. While it is a good thing to standardize outcomes to make accurate comparisons across individuals, not all strength-measurement equipment expresses force in the same way. So how do we know our patients are comparable to these reference values?
As the study expressed strength as torque normalized to body mass, force values from other dynamometers must first be converted to Newtons, multiplied by the patient’s moment arm, and then divided by body mass. Therefore, raw force values expressed in kilograms are not directly comparable unless the same test position, dynamometer placement, and moment-arm calculation are used.
Below is a way of converting the strength outcomes to other units.

Talk nerdy to me
The strength data from the healthy control participants were used to define a reference threshold for maximal hip abduction strength. The authors defined the lower boundary of the healthy reference interval as the 5th percentile of the healthy control distribution. This represents the value below which only 5% of healthy individuals in the control sample fell. For hip abduction strength, this threshold was 0.624 Nm/kg. Therefore, patients who reached or exceeded 0.624 Nm/kg were classified as being within the healthy reference interval, whereas those below this value did not reach the lower boundary of the healthy reference values. However, this threshold should not be interpreted as full recovery or average normal strength; it represents only the lowest boundary of the healthy reference values.
A relevant question mark could be placed at why that 5th percentile was chosen. Especially because the authors then calculated the percentages of patients above this threshold and of those achieving normal limb symmetry. First of all, this reference frame was based on only 24 healthy women, so it is basically a very small sample to define a population-based threshold. But most importantly, would you consider yourself recovered when you’re just at the 5th percentile? I guess not, so why do we set such a low threshold for patients? The 5th percentile represents the lower boundary of healthy reference values, not typical or complete recovery. People at this level are still healthy, but clearly below average.
This is not just semantics; it changes the whole interpretation since a low threshold of “normal values” inflates the perception of recovery success. Saying “61% reached normal” sounds reassuring, but actually, many of those patients may still be weak compared to average healthy individuals. So, a more accurate interpretation is that 61% of patients reached the lowest acceptable boundary of healthy hip abduction strength, not necessarily average, optimal, or full functional strength. This distinction matters clinically, especially because the median hip abduction strength of the healthy controls was 0.92 Nm/kg, whereas the 5th percentile threshold was only 0.624 Nm/kg.
Therefore, the findings suggest that many patients improved enough to cross a minimal healthy reference threshold, but not necessarily enough to regain typical healthy strength. This is particularly relevant when setting rehabilitation goals, because stopping rehabilitation once a patient crosses the 5th percentile may leave meaningful residual strength deficits unaddressed.

Take-home messages
This prospective longitudinal cohort study provides insight into the recovery patterns of hip abductor function after gluteal tendon reconstruction from baseline to 1 year postoperative. Data from patients scheduled for partial- or full-thickness repair of the torn gluteus medius (with or without a concomitant gluteus minimus tendon tear) were compared with healthy age-matched controls to inform strength recovery timelines. One critical limitation is the set minimum threshold for regaining “normal” strength. The authors set this threshold at the 5th percentile of the strength data from the healthy controls. While it is a good way of setting a goal, the 5th percentile can not be considered “normal”. Rather, it should be seen as the lowest acceptable boundary of normal, and interpreting it as full recovery risks overestimating patient outcomes.
Reference
LEVEL UP YOUR DIFFERENTIAL DIAGNOSIS IN RUNNING RELATED HIP PAIN - FOR FREE!
Don’t run the risk of missing out on potential red flags or ending up treating runners based on a wrong diagnosis! This webinar will prevent you to commit the same mistakes many therapists fall victim to!
