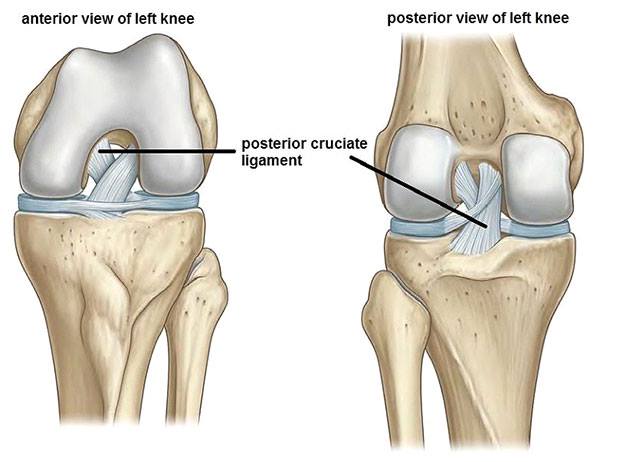
Posterior Cruciate Ligament Tears - From Diagnsosis to Treatment will give you a quick overview inlcuding all important facts about PCL tears
There is a lot of literature about the ACL, but what about the less common injured posterior ligament? In April this year, a systematic review was published by Vaquaro-Picado et al. We will try to give you the highlights:
Incidence
– 200000 ACL injuries per year in the US, only 3% of the injured knees have a PCL disruption.
– PCL injuries rarely occur in isolation. Most grade III PCL injuries present concurrently with other ligament injuries (79% of cases). 5 These associated injuries are of the ACL in 46%, the MCL in 31% and the PLC in 62%.
– PCL is more seen by man (97%) compared with females (73%).
Mechanism
– High-energy trauma, such as sport and motor vehicle accidents (57% of cases).
– Abrupt posterior tibial translation (such as dashboard impact), falls in hyperflexion, and direct hyperextension trauma
– Knee dislocation or rotation combined with varus/valgus forces.
Diagnosing
– Patient history is important: trauma-analysis, instability, and discomfort
– Physical examination: Posterior drawer test, Dial test and the External rotation-recurvatum test
– Imaging: The use of MRI techniques has been demonstrated to be highly accurate for diagnosing acute PCL tears. High sensitivity (near 100%) and specificity (near 97%) have been reported
Surgery or not?
Acute injury
– Grade I and II injuries: (< 10 mm posterior laxity): Conservative treatment
– Grade III injuries (> 10 mm posterior laxity): PCL injury may be treated conservatively but if instability persists, reconstruction should be performed
Chronic injury
– Grade I and II injuries: Conservative treatment
– Grade III injuries: PCL injury should be reconstructed if pain and instability persist after conservative treatment
ACL Injuries: From Theory to Practice
This first-of-its-kind online course offers an incredible continuing education opportunity for clinicians who manage patients with ACL injuries.
Treatment
Conservative:
– In acute stadium a brace for 2-4 weeks. The PCL has an intrinsic capability for healing. This is the reason why, nowadays, the majority of isolated PCL tears are managed non-operatively, with rehabilitation and bracing.
– After that, a program encouraging strengthening is required.
– Return to sport time is often nog before three months from the injury, depending on the sport.
After surgery:
– Immobilised for three to six weeks in full extension, after that progressive passive flexion range is allowed.
– The brace should be worn all the time for at least two to four months. Dynamic braces, applying an anterior drawer force depending on flexion degree, can be useful during the rehabilitation programme.
– Rehabilitation takes normally 6-9 months, depending on the sport. End-critera are badly described, but at least 90% LSI must be achieved.
Vaquaro-Picado et al. (2017): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5420825/








