Cluster Headache | Diagnosis & Treatment All you need to know

Cluster Headache | Diagnosis & Treatment All you need to know
Introduction & Epidemiology
Headaches can manifest on their own but are also a very common symptom in neck pain patients as more than 60% of patients with a primary neck pain complaint report having concordant episodes of neck pain. Therefore it’s essential to find out what kind of headache the patient is suffering from.
To start off let’s differentiate between primary and secondary types of headaches. But what does this mean? Simply put, primary headaches are a “disease themselves” whereas, in secondary headaches, the headache is a symptom of another condition. So primary headaches would be migraines, tension-type headaches & cluster headaches. Secondary type headaches are headaches caused by tumors, hemorrhage, other trauma, TMJ dysfunction, substance overdose, or neck pain aka. The cervicogenic headache.
Now let’s take a closer look at cluster headaches, which are primary types of headaches.
Fischera et al. (2008) conducted a meta-analysis to assess the lifetime prevalence of cluster headache and found low numbers of 0,12% with a 1-year prevalence of 53 per 100,000 persons and the overall sex ratio was 4.3 (male to female). Cluster headache had a 1-year prevalence of 0,054% among the working-aged population in a Swedish cohort (Manzoni et al. 2019)
Epidemiology
The following figure shows the prevalence of headaches on different continents around the world: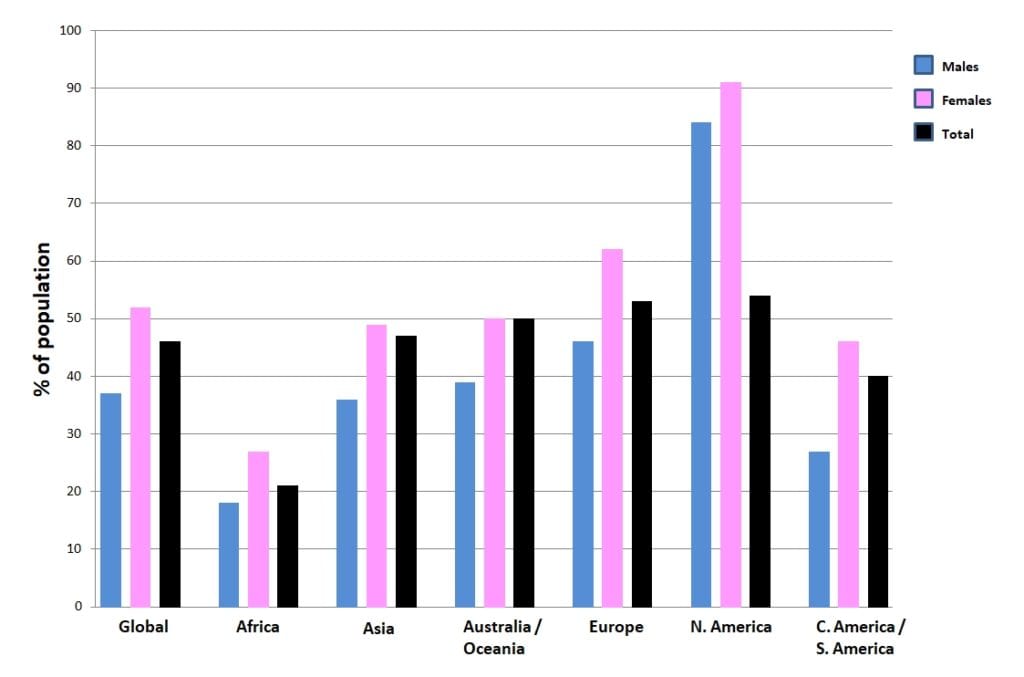
Clinical Picture & Examination
In order for a headache to qualify as a cluster headache it has to fulfill certain criteria (ICHD-III):
A. At least five attacks need to fulfill criteria B-D
B. An untreated episode lasts 15-180 minutes and shows severe or very severe unilateral orbital, supraorbital, and/or temporal pain
C. It matches either or both of the following:
- at least one of the following signs and symptoms, ipsilateral to the headache:
– conjunctival injection and/or lacrimation
– nasal congestion and/or rhinorrhoea
– eyelid edema– forehead and facial sweating
– miosis and/or ptosis - a sense of restlessness or agitation. There are reports of patients pacing back and forth through the room, banging their heads due to the severe pain.
D. It occurs with a frequency between one every other day and 8 per day
100% Free Headache Home Exercise Program