Cervicogenic Headache | Diagnosis & Treatment for Physios

Cervicogenic Headache | Diagnosis & Treatment for Physios
Introduction & Epidemiology
Headaches can manifest on their own but are also a very common symptom in neck pain patients as more than 60% of patients with a primary neck pain complaint report having concordant episodes of neck pain. Therefore it’s essential to find out what kind of headache the patient is suffering from.
To start off let’s differentiate between primary and secondary types of headaches. But what does this mean? Simply put, primary headaches are a “disease themselves” whereas, in secondary headaches, the headache is a symptom of another condition. So primary headaches would be migraines, tension-type headaches & cluster headaches. Secondary type headaches are headaches caused by tumors, hemorrhage, other trauma, TMJ dysfunction, substance overdose, or neck pain aka. The cervicogenic headache.
Now let’s take a closer look at cervicogenic headache, which is a secondary type of headache.
Epidemiology
The following figure shows the prevalence of headache on different continents around the world: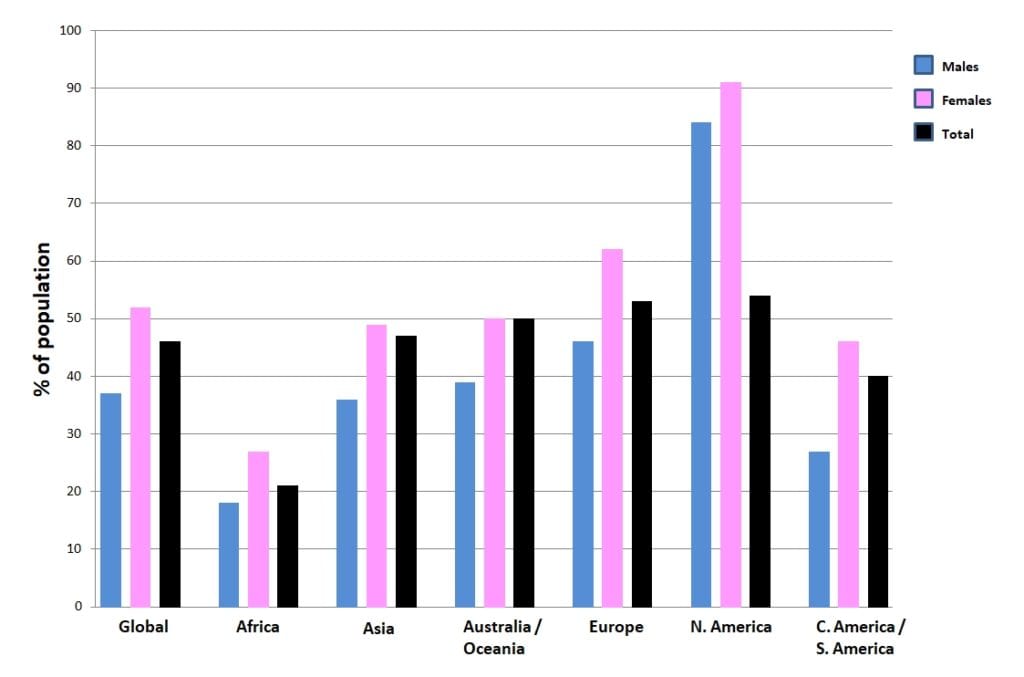
Other studies on the prevalence of CGH have reported a prevalence range between 0,17 – 4,1% (Knackstedt et al. 2010; Antonaci et al. 2011; Sjaastad et al. 2008).
But how can the neck refer pain to the head?
In the case of referred pain, pain is perceived in a region other than the site of the painful stimulus. Thus, pressure or load on the place where the pain is felt usually does not lead to an increase in pain intensity. However, pressure or load on the place of the sensitized nociceptors results in an increase in pain intensity in the referred area. In the case of cervicogenic headache, nociception in the structures of the neck leads to referred pain in the head.
If we follow the convergence-projection theory outlined in our other video, we first need a structure responsible for nociception in the high cervical area that has a low density of nociceptive afferent innervation. These are usually structures that are lying deep, such as the facet joints including their joint capsules at C2/C3 or the alar ligaments reaching from the dens of C2 to the occiput for example. The afferent innervation of those structures converges on the second-order neuron in the dorsal horn at the height of C1/C2.
At the same time, our face has a very high density of afferent nociceptive innervation and receives sensory innervation from cranial nerve number 5 – the trigeminal nerve. The trigeminal nerve in turn converges onto the second-order neuron in the trigeminal nerve nucleus, which is the largest cranial nerve nucleus. It extends from the midbrain, to the pons and medulla into the spinal cord until C1/C2. So the trigeminal nerve’s innervation and the innervation of deep structures of the upper cervical spine converge onto the same spinal segment.
So when the afferent nociceptive stimulus from the neck, travels to the second-order neuron in the dorsal horn at segment C1/C2 and finally reaches the somatosensory cortex, this part of the brain then has to figure out the origin of the stimulus. In this case, the brain makes a projection error and decides that the nociceptive stimulus must be coming from the area with the higher nociceptive afferent innervation, which is the face rather than the poorly innervated upper cervical area. In other words, the brain projects pain into the fronto-orbital area of the head.

If the whole face is innervated by the trigeminal nerve, why do we only feel headaches in the frontal-orbital area and not the cheek and the jaw? The trigeminal nerve splits into 3 different branches, which are:
- The ophthalmic nerve supplying the scalp, forehead, and orbital area amongst others
- The maxillary nerve supplying the cheek, upper lip, and upper teeth amongst others
- The mandibular nerve supplying the lower lip, chin and jaw up to the temporal area
When those 3 nerve branches reach the trigeminal nerve nucleus, they are inverted. Remember that the trigeminal nerve nucleus is large and it consists of three different subparts. The mandibular and maxillary nerves converge onto the pars oralis and pars interpolaris of the trigeminal nerve nucleus respectively, which both don’t reach as far caudal as the spinal cord. Only the ophthalmic nerve converges onto the pars caudalis of the trigeminal nerve nucleus which is located in the spinal cord at the height of C1/C2, exactly where the afferents from structures in the upper cervical spine converge.
It’s important to mention that we are talking about unilaterally innervated structures of the neck and face. So referred pain from the structures of the neck on the right for example will always lead to headache on the right side and the left side will refer to the left side.
Clinical Picture & Examination
In order for a headache to qualify as a cervicogenic headache it has to fulfill certain criteria (ICHD-III):
First and foremost, there will be clinical, laboratory, and or imaging evidence of a disorder or lesion in the cervical region known to be able to cause headaches such as for example the facet joints or certain muscles.
Furthermore, at least two of the following criteria have to apply:
- The headache has developed after the onset of the cervical disorder or lesion. So patients will probably describe a trauma during patient history.
- The headache improves or resolves in parallel with the improvement and/or resolution of the cervical disorder or lesion
- Cervical range of motion is reduced, the pain is movement/posture dependent and the headache is made significantly worse by provocative testing. For example, decreased upper cervical spine rotation as assessed by the flexion rotation test can be linked to cervicogenic headache
- The headache is abolishe after diagnostic blockade of a cervical structure or its nerve supply
Next to the ICDH-III criteria, Sjaastad et al. (2008) have proposed the following criteria to classify a headache as cervicogenic:
- Provocation: unphysiological neck positions
- Provocation externally, neck
- Reduced range of motion in the neck ( ≥ 10 degrees deficit)
- Shoulder pain ipsilateral
- Arm pain, ipsilateral
- Unilateral headache (without side shift)
- Onset posteriorly in the neck/occipital area
Examination
Compared with healthy controls, the average patient with cervicogenic headaches differs on provocation, cervical range of motion (including the flexion-rotation test), and neck muscle endurance.
The goal of provocation tests is to recreate the patient’s familiar pain. This way, you are able to confirm the location of nociception in the cervical structures, possibly leading to referred pain to the head. Cervicogenic headache can be provoked with the following technique:
Passive assessment of the quantity and quality of segmental intervertebral motion, also known as motion palpation, is part of the diagnostic clinical expertise of manual practitioners to guide decisions on a therapeutic strategy for patients with spinal pain
Hypomobility indicates mobilizing interventions while hypermobility calls for a stabilizing approach. A systematic review done by van Trijffel et al. (2005) evaluated the reliability of passive segmental assessment of the cervical spine and found an overall reliability of poor to fair. However, for segments C1/C2 and C2/C3 at least fair reliability was reached consistently. For this reason, we give this examination a moderate clinical value.
In order to perform regional range of motion assessment for upper cervical spine flexion of vertebrae’s C0 til C3 have your patient sit upright at the edge of the bench or on a stool, the bench height should be adjusted so that your patient’s head is at the same height as your belly.
First, fixate the spinous process of C3 with a key grip into a ventrocranial direction. Be aware that this is the other way around than in other parts of the spine due to the ligamentous connections of the upper cervical spine.
Then your working hand is placed low on the patient’s occiput and the patient’s head is fixated between your working hand and chest. Now perform a maximal heteronymous 3D movement with equal components of flexion, contralateral lateral flexion, and ipsilateral rotation.
For the regional assessment of upper cervical spine extension, change your fixation of C3 into ventrocaudal direction and place your working hand higher on the patient’s occiput. Then perform a maximal heteronymous 3D movement with equal components of extension, contralateral lateral flexion, and ipsilateral rotation.
Both movements are judged on resistance during motion and at end range, range of motion, as well as possible pain provocation compared to the other side.
For upper cervical spine assessment be aware that a limitation at C2/C3 can influence the movement of the higher segments for this reason C2/C3 has to be assessed first. A limitation of C0/C1 can limit the movement of C1/C2. For this reason, we will start with the segmental assessment of C0/C1 first.
First, fixate your patient’s spinous process C2 with a key grip. Then place your hypothenar eminence on the patient’s mastoid process on the contralateral side and fixate the patient’s head with your chest. Then rotate your patient’s head until you feel resistance.
To assess movement at C0/C1 perform a lateral flexion movement to the contralateral side by a coupled movement between your working hand and your chest. The movement has to take place around a sagittal axis through the nose of your patient. Furthermore, you can specify if the limitation lies on the contralateral or the ipsilateral condyle of the occiput to pronounce the downslip movement of the contralateral condyle of C0 (condyle on the side of your working hand) and perform the same lateral flexion movement with C0/C1 in extension.
To pronounce the upslip movement of the ipsilateral condyle of C0 (side of your chest) perform the same lateral movement with C0/C1 in flexion.
For the assessment of C1/C2 keep your fixation and move the hypothenar eminence of your working hand down to the contralateral arch of C1. Your patient’s head is in neutral position and no lateral flexion is present. Then rotate maximally and assess the end feel. Both movements are judged on resistance during motion, end-feel, as well as possible pain provocation, compared to the other side.
Upper cervical range of motion in the direction of rotation can be reliably and accurately assessed with the Flexion-Rotation Test (Hall et al. 2010a, Ogince et al. 2007, Hall et al 2010b). This test – is positive – can give you an indication of limited rotation on segments C1/C2. In turn, hypomobility on C0/C1 or C2/C3 can lead to this limitation in rotation on C1/C2.So in case of a positive test, we still need to perform intervertebral motion assessment of all upper cervical segments in order to find the dysfunctional segment.
Although no clear cut-off values are given, the performance time can give an indication of neck flexor endurance:
100% Free Headache Home Exercise Program