Research
Sports & RTP
June 29, 2026
Musculoskeletal Injury Prevention Programs: What Exercise Modalities are Most Effective? A Meta-Analysis Overview

Introduction
Injury prevention is a major challenge in competitive sports. Musculoskeletal injuries result from a complex interaction of factors, including suboptimal movement patterns, inappropriate training loads, fatigue, and sport-specific demands. Consequently, numerous injury prevention programs have been developed to address modifiable risk factors in athletes.
Current approaches to injury prevention emphasize the principle of specificity, suggesting that preventive interventions should closely replicate the motor and biomechanical demands of a particular sport. However, motor learning and motor control theories indicate that the transfer of training adaptations from preventive exercises to sport-specific performance may be limited when task characteristics differ substantially. In clinical settings, preventive programs are often constrained by practical considerations and may not sufficiently recreate the demands encountered during sports participation. This raises questions regarding the effectiveness of multimodal injury prevention programs that combine components such as strength, agility, balance, and proprioceptive training. Conversely, simpler single-component interventions, particularly strength-based programs, may offer a more targeted and clinically realistic approach.
The purpose of this review is to examine the effectiveness of injury prevention programs across different anatomical regions and sporting populations, and to summarize the evidence around multimodal and single-component injury prevention programs.
Methods
A comprehensive literature search was performed in medical databases. Study selection was conducted independently by two reviewers, who screened titles, abstracts, and subsequently full-text articles according to predefined inclusion and exclusion criteria. Any disagreements were resolved through discussion.
Data extraction included study characteristics (author, publication year), participant demographics (age, sex, sport), sample size, intervention characteristics (duration and frequency), exposure time, injury type, injury incidence, and injury counts. Injury rates were calculated as the number of injuries divided by the total number of participants and expressed as a percentage.
The authors conducted a meta-analysis to determine whether strength training reduced injury risk in contact sports. For each study, they calculated the injury rate by dividing the number of injuries by the number of participants in both the intervention and control groups. These injury rates were then used to calculate a Relative Risk (RR) with a 95% confidence interval, and the results from all studies were pooled together. A random-effects model was applied to account for differences between studies. The authors also performed subgroup analyses to examine whether the effects of strength training varied depending on body region (shoulder, knee, ankle, groin, or hamstring). Sensitivity analyses were conducted to assess the robustness of the findings. Finally, publication bias was evaluated using funnel plots and Egger’s test.
Results
This meta-analysis included 16 studies with a total of 7459 participants. Age ranged from 16 to 47 years, with males representing > 70% of participants. The study only included regular sport practitioners to minimize the confounding effect that inadequate training might have on injury risk.
Intervention and compliance
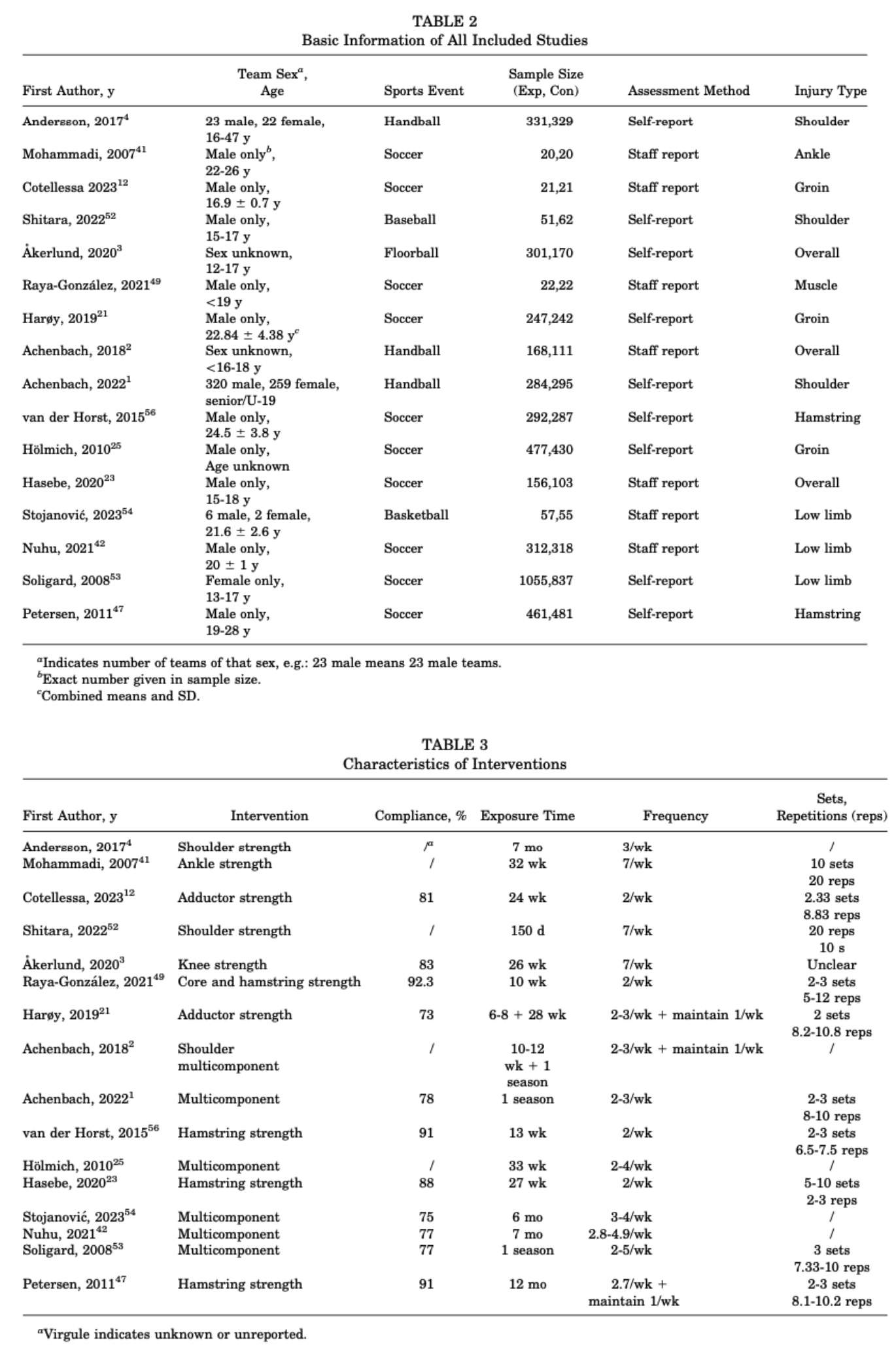
Although all 16 included studies followed established strength-training principles, the injury-prevention programs varied considerably. Interventions included eccentric exercises (such as Nordic hamstring exercises), concentric strengthening, isometric training, and combinations of different strength-training modalities. Some interventions also incorporated additional components such as balance and plyometric exercises and were typically performed as part of the warm-up before training sessions or matches. The duration of the interventions ranged from 10 to 46 weeks, and outcomes were reported as either overall injury rates or injuries affecting specific body regions. Participant adherence was generally high, with most studies reporting compliance rates above 70%. Detailed information on the study characteristics and intervention protocols, including training frequency, volume, exposure time, and compliance, is provided in Tables 2 and 3.
Meta-analysis and subgroup analysis results
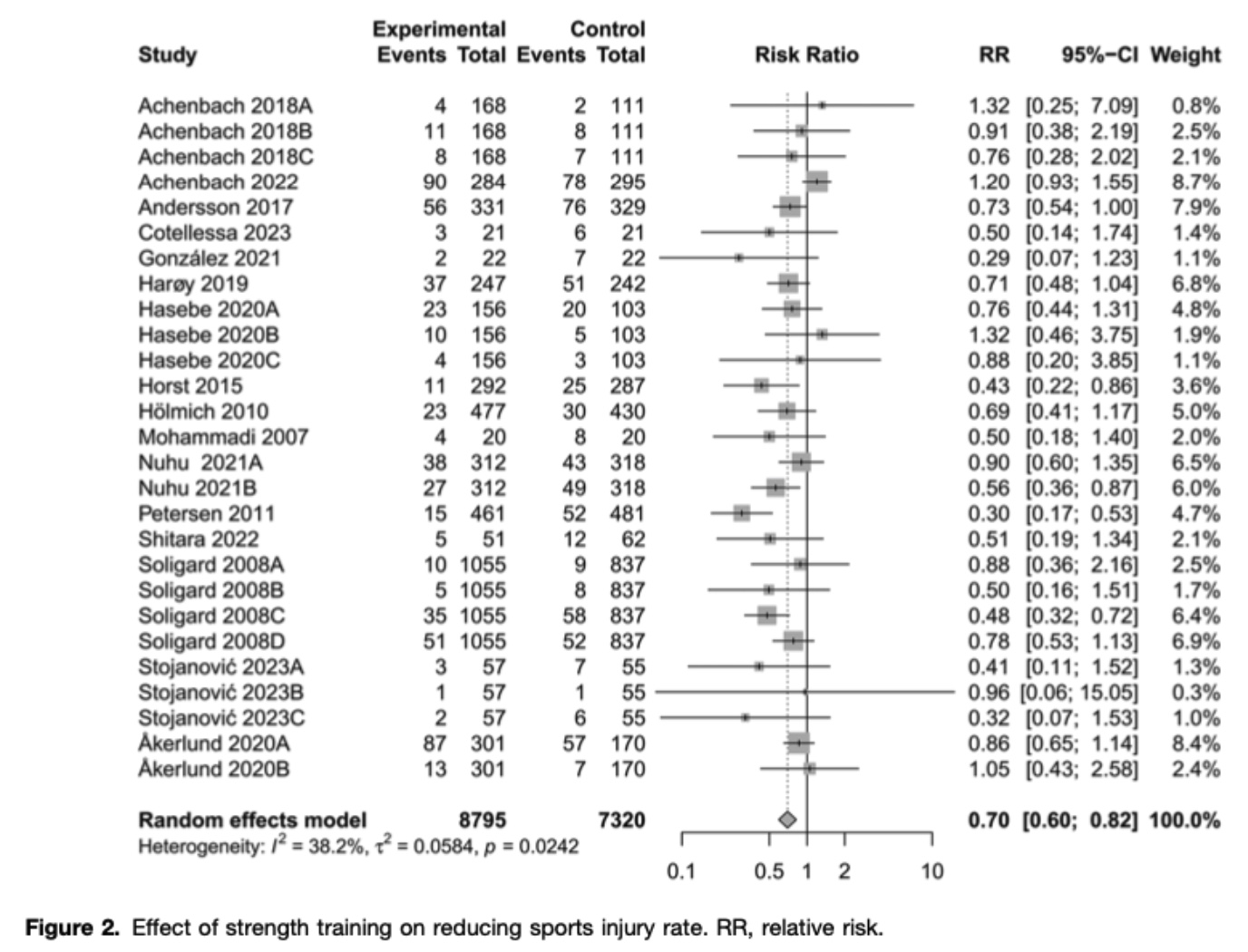
The meta-analysis included 16 studies reporting 27 outcomes and found that strength training significantly reduced the overall risk of injuries in contact sports. Using a random-effects model, the pooled results showed a 30% reduction in injury risk among athletes performing strength training compared with controls (RR = 0.70, 95% CI 0.60–0.82). The level of heterogeneity was low (I² = 38%), and there was no evidence of publication bias based on funnel plot inspection and Egger’s test.
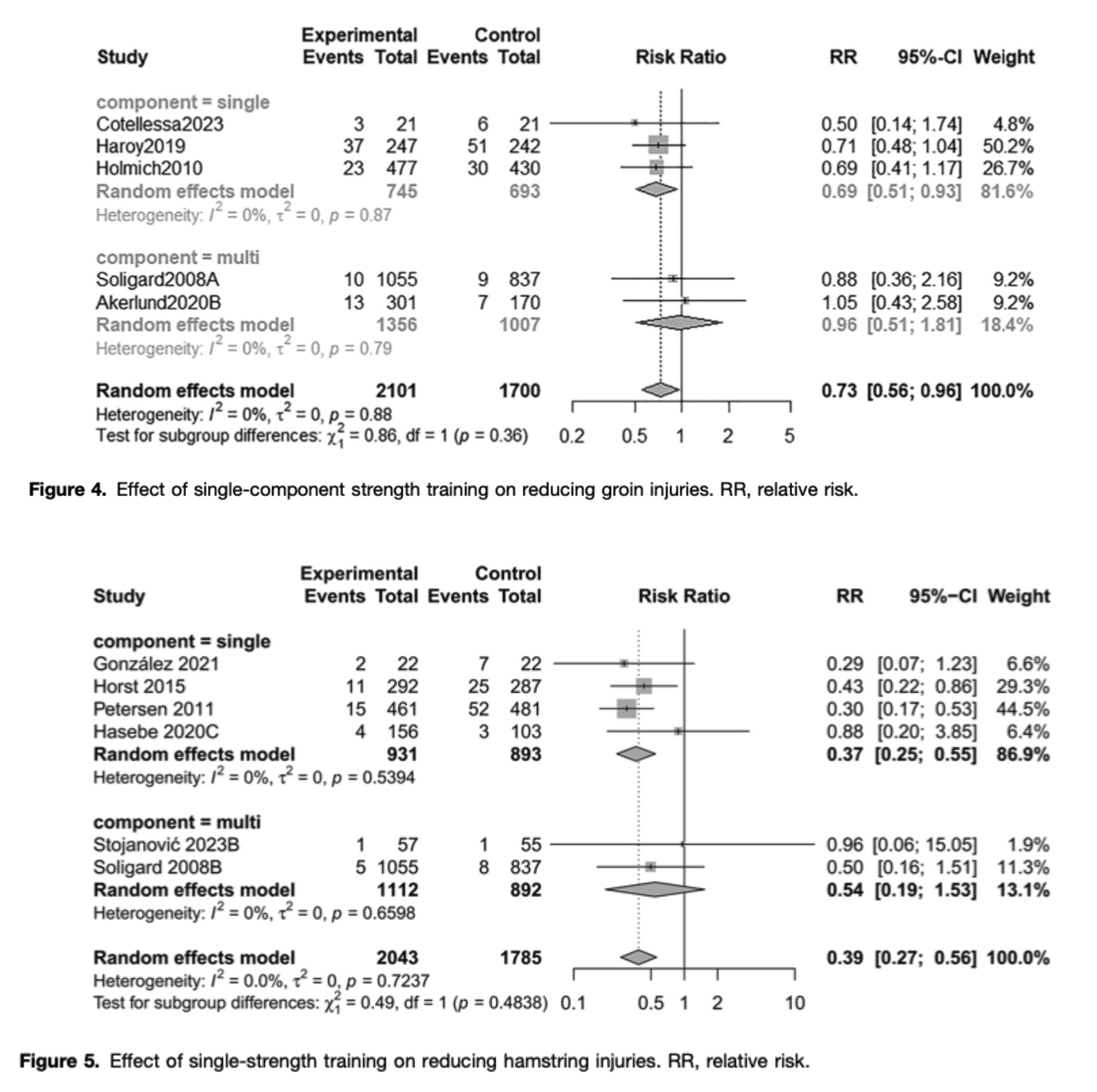
Subgroup analyses revealed that the effectiveness of strength training varied according to injury location and the type of intervention. Single-component strength-training programs significantly reduced groin injuries by 31% (RR = 0.69, 95% CI 0.51–0.93) and hamstring injuries by 63% (RR = 0.37, 95% CI 0.25–0.55), with no heterogeneity observed between studies for either outcome (I² = 0%).
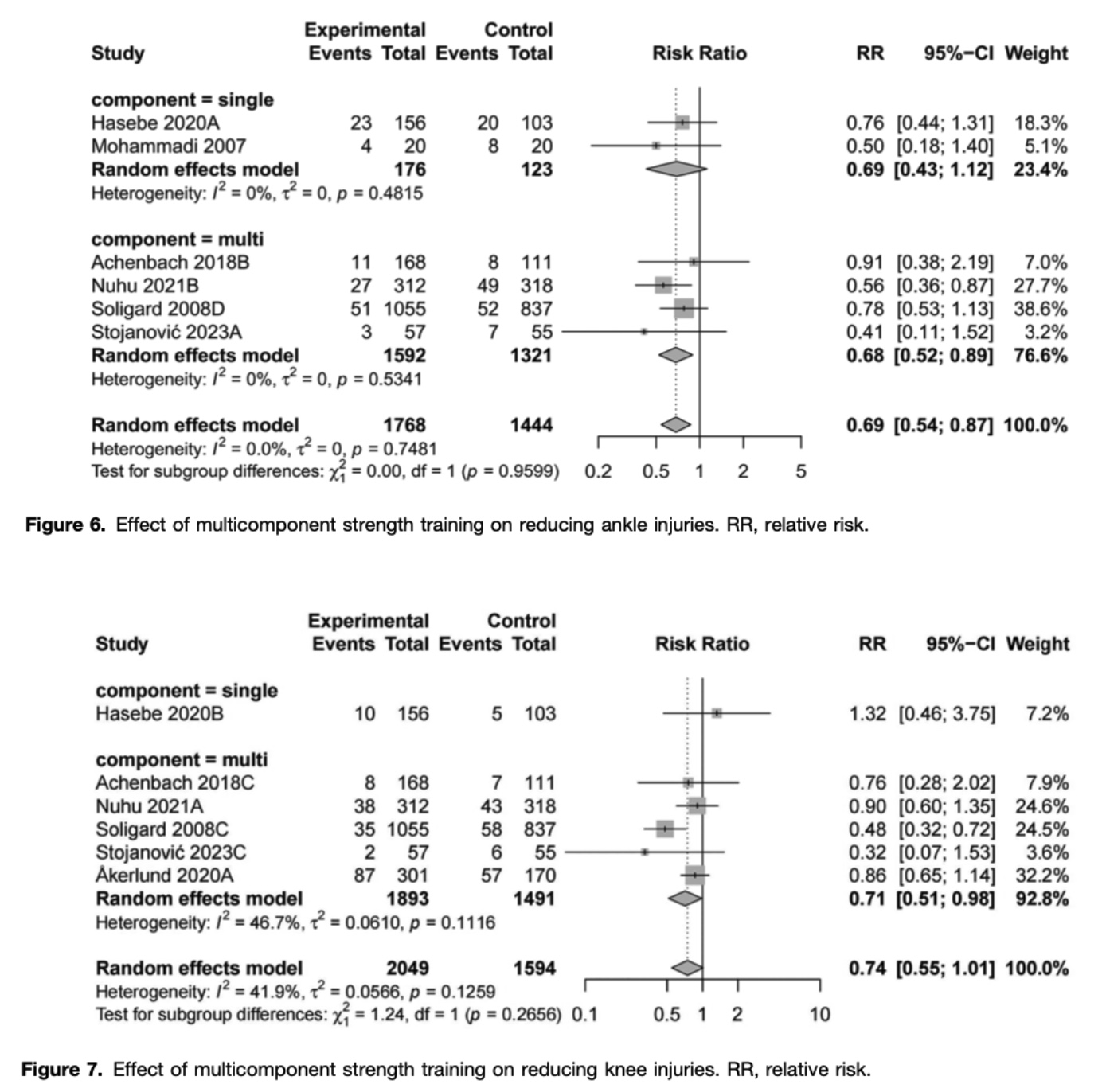
Multicomponent injury prevention programs, combining strength exercises with other elements such as balance or plyometric training, significantly reduced ankle injuries by 32% (RR = 0.68, 95% CI 0.52–0.89) and knee injuries by 29% (RR = 0.71, 95% CI 0.51–0.98). Heterogeneity was absent for ankle injuries (I² = 0%) and moderate for knee injuries (I² = 47%).
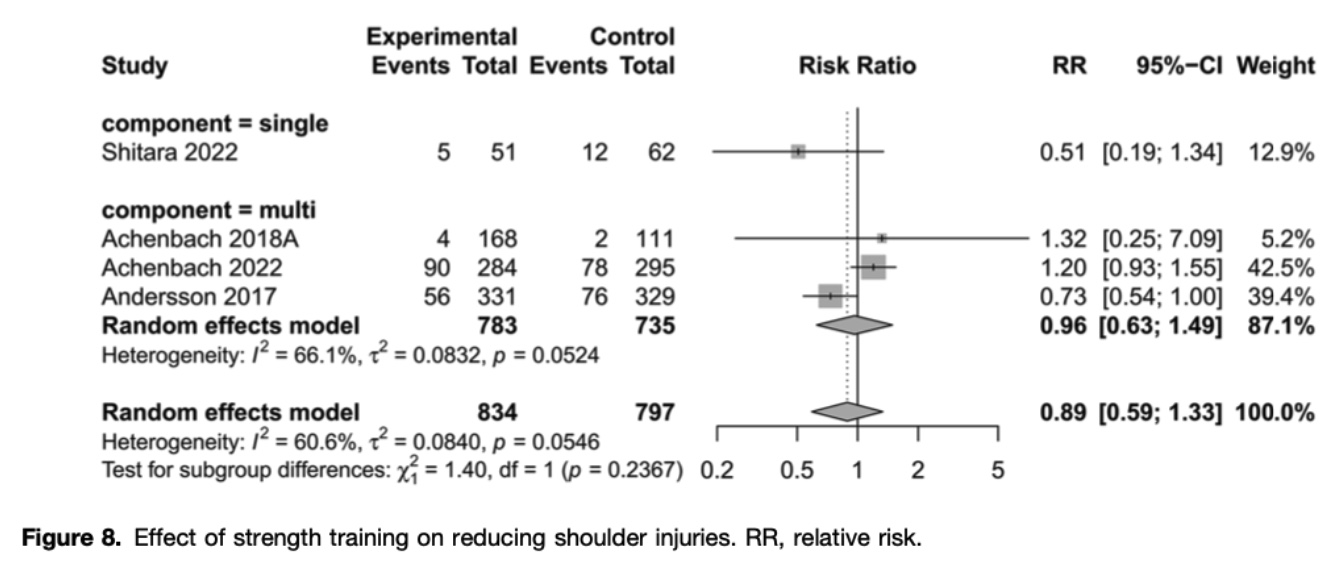
In contrast, strength training did not appear to reduce shoulder injury rates. The confidence intervals for all shoulder injury analyses crossed the null value (RR = 1.0), indicating no statistically significant effect. Furthermore, substantial heterogeneity was observed among shoulder injury studies (I² = 61%), suggesting greater variability in the results.
Quality assessment of included studies
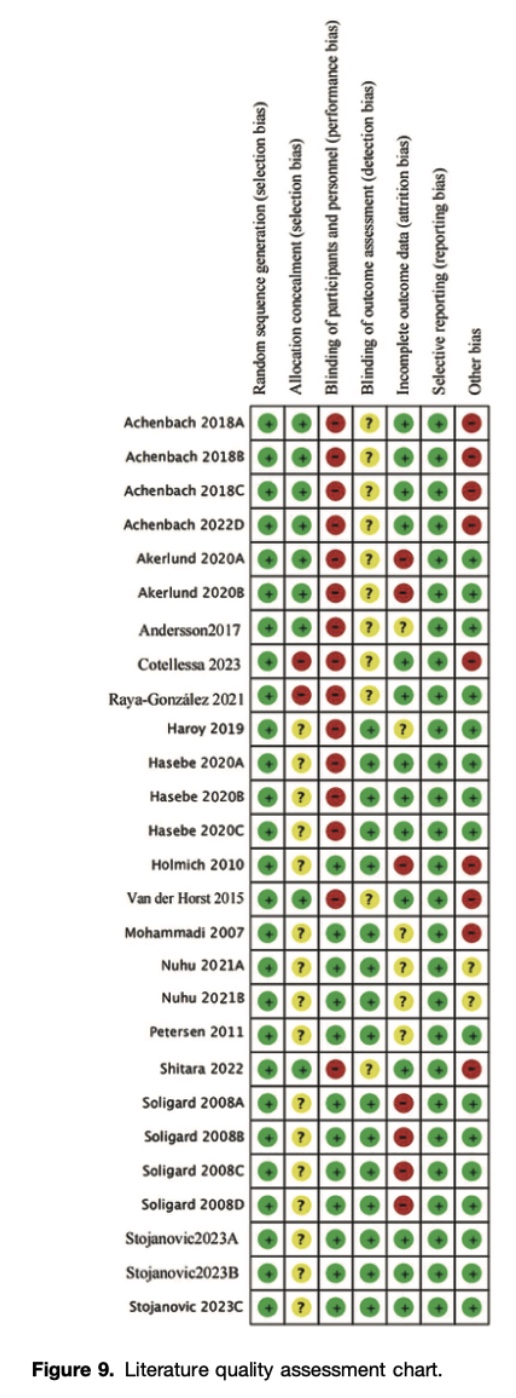
All included studies were randomized controlled trials and were considered to provide level 2 evidence or higher, reflecting a generally high methodological quality. However, blinding participants to group allocation was a major challenge due to the nature of exercise-based interventions. As is common in therapeutic exercise research, participants were aware of whether they were receiving the intervention, which may have increased the influence of contextual factors and potentially affected participant behaviour and exposure to injury risk. In addition, some studies relied on self-reported questionnaires to assess injuries, particularly overuse injuries, which may have introduced reporting bias and affected the accuracy of outcome measurement.
Questions and thoughts
The effectiveness of a multicomponent injury prevention program raises important questions regarding the transferability of training adaptations to sport-specific performance. In clinical settings, it is often difficult to reproduce the complex motor tasks, environmental constraints, and decision-making demands encountered during sport participation. Consequently, the transfer of injury prevention programs to on-field performance may not be as straightforward as commonly assumed.
Ecological motor control theory provides an interesting framework through which to interpret these findings. According to this theory, movement emerges from the interaction between the individual, the task, and the environment. A central concept is perception-action coupling, whereby movement behaviour is continuously shaped by the information available in the environment.
Applied to injury prevention, this perspective suggests that transfer may be enhanced when training environments preserve key perception-action constraints present during sport participation.
For hamstring and groin injuries, isolated strength training interventions were highly effective, probably because the hamstring and adductor muscles are exposed to substantial mechanical demands during activities such as sprinting, cutting, and jumping. This finding may reflect the predominantly mechanical nature of these injuries, whereby increasing tissue load capacity directly targets a key component of the injury mechanism. In contrast, ankle and knee injuries occur within more variable and unpredictable environments involving multidirectional loading and rapid perturbations. This may explain why multicomponent programs, combining strength, balance, and coordination exercises, appear more effective for these joints.
However, these conclusions might be challenged regarding the ongoing debate surrounding proprioceptive training. Traditionally, injury prevention programs have frequently incorporated unstable surface exercises under the assumption that they improve proprioception. However, recent literature has challenged both the assessment and training of proprioception as an isolated construct. Performance during balance tasks reflects the integration of multiple sensory systems, including visual, vestibular, cutaneous, and proprioceptive inputs, making it difficult to determine whether observed improvements result from enhanced proprioceptive acuity itself.
From an ecological perspective, this debate may partly stem from an overly reductionist view of proprioception. Rather than considering proprioception as an isolated sensory capacity that can be independently trained, ecological theories emphasize the continuous interaction between perception and action within a specific task environment. Consequently, improvements observed following balance or unstable surface training may reflect enhanced sensorimotor coordination and more effective use of available environmental information rather than changes in proprioceptive function alone.
Interestingly, this interpretation may also help explain findings from previous systematic reviews on chronic ankle instability rehabilitation. While strength training has consistently demonstrated positive effects on postural control and dynamic balance outcomes such as the Star Excursion Balance Test, interventions labelled as proprioceptive or neuromuscular training have not always produced superior effects. Together, these findings suggest that increasing physical capacity through strength training may contribute substantially to injury prevention, while the specific mechanisms underlying the benefits of balance and proprioceptive interventions remain less clearly understood.
Talk nerdy to me
The heterogeneity of the included studies warrants careful consideration. As shown in Tables 2 and 3, the included studies present substantial clinical diversity across several dimensions, including the sport studied, sex distribution, age range, and outcome assessment methods. Yet, the statistical heterogeneity reported in Figure 5 is 0%, which would imply near-perfect uniformity across studies in terms of populations, protocols, and assessment methods.
This inconsistency becomes particularly apparent when examining the multi-component subgroup analysis in Figure 5. Despite reporting I² = 0%, Tables 2 and 3 reveal meaningful differences between the two included studies: one enrolled female-only adolescent soccer players (Soligard, 2008), while the other included a predominantly male basketball sample (Stojanović, 2023). Furthermore, the interventions differed notably in both frequency (2–5/week vs. 3–4/week) and duration (one full season vs. six months), and the sports contexts were distinct. The reporting of zero heterogeneity under these conditions is therefore difficult to justify on clinical grounds alone.
A plausible statistical explanation is that the heterogeneity analysis was underpowered, as subgroups comprising only two studies provide virtually no power to detect between-study variance, often resulting in τ² and I² estimates that default to zero as a computational artifact rather than reflecting genuine homogeneity. However, the authors provide no explicit description of the heterogeneity testing method in the methodology section, making it impossible to evaluate this assumption. This omission represents a meaningful methodological limitation, as transparency in statistical approaches is essential for appraising result validity.
Taken together, these concerns reduce confidence in the precision of the pooled estimates and suggest that the study’s conclusions should be interpreted with considerable caution.
Take-home messages
- Strength training is clearly effective for injury prevention in contact sports, with a pooled ~30% reduction in overall injury risk (RR = 0.70), supporting its role as a core component of prevention programs rather than an optional add-on.
- “Simple” may be powerful: single-component strength programs were highly effective for specific muscle-tendon injuries, particularly:
- Hamstring injuries (~63% reduction)
- Groin injuries (~31% reduction)
- Multicomponent programs are more relevant for joint injuries:
- Ankle injuries (~32% reduction)
- Knee injuries (~29% reduction)
- Shoulder injury prevention remains unresolved, with no clear benefit of strength-based interventions and high heterogeneity, indicating that:
- Current prevention models may not adequately target shoulder injury mechanisms in contact sports
- or that shoulder injuries are more context- and sport-specific than lower-limb injuries
- When designing injury prevention programs, therapists should prioritize tasks that closely replicate the performance context, particularly in terms of both perception and action demands, to enhance transferability to sport-specific situations.
- Interpret results with caution due to methodological limitations:
- Subgroup heterogeneity may be underestimated (e.g., I² = 0% in very small subgroups)
- Clinical diversity (sport, sex, age, protocols) is not always reflected in statistical outputs
- This reduces certainty in fine-grained comparisons between program types
Reference
100% FREE POSTER PACKAGE
Receive 6 High-Resolution Posters summarising important topics in sports recovery to display in your clinic/gym.