
Research
EBP & Statistics
April 30, 2026
Carpal Tunnel Syndrome Treatment: Hand Pain and Sensory Deficits – Latest Evidence from Clinical Practice Guidelines - Part 2: Intervention and Outcomes

Introduction
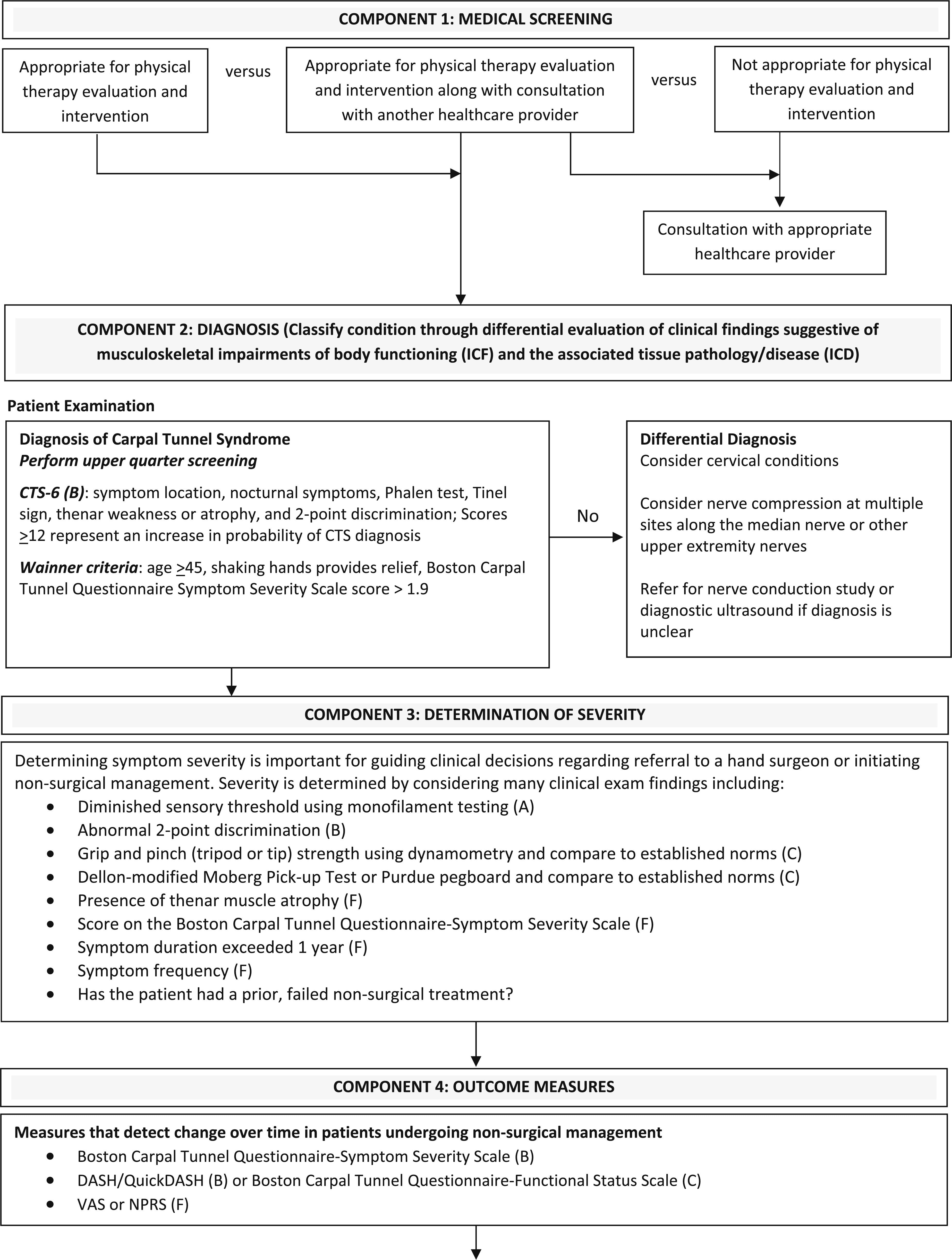
This Part 2 follows last week’s article on the diagnosis of carpal tunnel syndrome. This article aims to review current outcome measures and carpal tunnel syndrome treatment options, with a particular focus on physiotherapy management. Interventions ranging from orthosis prescription to manual therapy and biophysical agents will be discussed. In light of the evolving understanding of carpal tunnel syndrome pathophysiology, the rationale behind many commonly used physiotherapy interventions may warrant closer examination. If multiple mechanisms contribute to pain and functional impairment, can these traditional approaches fully address the complexity of the condition? While current guidelines provide broad recommendations, they leave room for interpretation. Therefore, clinical reasoning remains essential to identify and address the different drivers of symptoms in each patient. To support this process, this article also provides a practical decision tree to help guide the management of individuals with carpal tunnel syndrome.
Methods
As this review is the second part of an earlier published review on examination and diagnosis, the methods have already been described there.
Results
Outcome measures
Patient-reported outcome measures are the most appropriate tools for assessing change over time in carpal tunnel syndrome, as they capture symptom progression and functional impact more accurately than impairment-based or performance-based measures.
Grade A: Clinicians should not use lateral pinch strength as an outcome measure for non-surgically managed or surgically managed carpal tunnel syndrome.
Grade B: Clinicians should not use grip strength to assess short-term changes (less than 3 months) in patients with surgically managed carpal tunnel syndrome.
Clinicians should use the Boston Carpal Tunnel Questionnaire Symptom Severity Scale (BCTQ-SSS) to assess change in symptoms, as it has the strongest and most consistent evidence for responsiveness and clinically meaningful change in both nonsurgical and surgical populations. Clinicians should also use a region-specific functional questionnaire such as the DASH or QuickDASH to assess functional change over time.
Grade C: Clinicians may use the Boston Carpal Tunnel Questionnaire Functional Status Scale (BCTQ-FSS) to assess functional change when the DASH or QuickDASH are unavailable, although some concerns exist regarding its construct validity.
In surgically managed patients, clinicians may also use PROMIS domains, including Pain Interference (PROMIS-PI) and Upper Extremity (PROMIS-UE), as well as the Michigan Hand Questionnaire (MHQ) (not readily available), which demonstrate favourable results for assessing changes.
Regarding the PPB test, the Jebsen-Taylor Hand Function Test, or the Nine-Hole Peg Test, to assess clinical change following carpal tunnel release, no additional evidence is available. As such, the 2019 guidelines remain applicable. None of these tests should be used to assess changes following carpal tunnel release surgery.
Grade D: As there is no new evidence and as stated by the 2019 guidelines, there is conflicting evidence regarding the use of sensory measures (e.g., two-point discrimination, threshold testing) and certain strength measures (e.g., tip and tripod pinch, abductor pollicis brevis strength) to assess change over time following surgical management, limiting their clinical utility.
Treatment
Orthoses
Grade B: Clinicians should recommend a forearm-based wrist immobilization orthosis that maintains the wrist in a near-neutral position in the sagittal plane. This orthosis should be worn at night to achieve short- to mid-term improvements in symptoms and function in individuals with mild to moderate carpal tunnel syndrome who are seeking nonsurgical management or awaiting surgery.
Grade C: Clinicians may adjust orthosis wear time to include daytime, symptomatic, or full-time use when nighttime wear alone is insufficient to control symptoms. Modifications such as adding metacarpophalangeal (MCP) joint immobilization or altering wrist positioning may also be considered in individuals who do not experience adequate symptom relief.
Grade C: Clinicians may recommend the use of a wrist orthosis for women with carpal tunnel syndrome during pregnancy, with postpartum follow-up to assess symptom resolution.
Grade C: Clinicians may recommend using a wrist orthosis in conjunction with corticosteroid injection as part of nonsurgical management.
Interestingly, the available literature suggests that longer durations of orthosis use are associated with greater improvements in symptoms and function, as measured by the BCTQ, with outcomes at 6 months exceeding those observed after 6 weeks of use.
Ergonomic education
Grade C: Clinicians may educate patients on the effect of computer mouse use on carpal tunnel pressure and assist them in developing alternative strategies, such as using arrow keys, touch screens, or alternating the mouse hand. Clinicians may also recommend keyboards requiring reduced strike force for individuals who report pain during keyboard use.
Grade F: Clinicians may provide general education on carpal tunnel syndrome pathology and risk factors, identify potentially contributing activities and wrist or hand positions, and collaborate with patients to modify these exposures. However, current evidence does not support a meaningful impact of these interventions on clinical outcomes.
No studies meeting the inclusion criteria examined the effect of education on carpal tunnel syndrome pathology and risk factors on patient symptoms or function. However, based on expert consensus from the CPG authors, education should still be provided to promote patient understanding of the condition and support self-management.
Manual therapy techniques
Grade C: Clinicians may provide manual therapy targeting the cervical spine and upper extremity, particularly along areas of potential median nerve entrapment, to achieve short-term improvements in pain and function in individuals with mild to moderate carpal tunnel syndrome managed nonsurgically.
Grade C: Clinicians may use instrument-assisted soft tissue techniques, such as diacutaneous fibrolysis, to support short-term improvements in symptoms and function in individuals with mild to moderate carpal tunnel syndrome managed nonsurgically.
Therapeutic exercises
Grade C: Clinicians may implement a combined orthotic and stretching program for individuals with mild to moderate carpal tunnel syndrome managed nonsurgically, particularly in the absence of thenar atrophy and when two-point discrimination remains normal.
Taping
Grade C: Clinicians may apply kinesiology taping to achieve short- to mid-term improvements in symptoms in individuals with mild carpal tunnel syndrome managed nonsurgically.
Limited evidence is available regarding the use of taping for carpal tunnel syndrome treatment. One study reported that rigid taping produced greater short-term improvements in BCTQ scores compared to a night orthosis; however, the evidence is too sparse to support a definitive recommendation. Similarly, one study found that kinesiology taping combined with exercise was more effective in improving pain and symptom severity than exercise with sham taping. Despite these findings, the underlying mechanisms by which kinesiology taping may influence carpal tunnel syndrome symptoms remain unclear.
Biophysical agents
Laser therapy
Grade C: Clinicians may use low-level laser therapy (LLLT) or high-intensity laser therapy (HILT) to achieve short-term improvements in pain and function in individuals with mild to moderate carpal tunnel syndrome managed nonsurgically.
The evidence regarding laser therapy for carpal tunnel syndrome treatment is conflicting. Some studies report greater short-term improvements in pain and BCTQ scores with low-level laser therapy (LLLT) compared to kinesiology taping. However, when LLLT is added to orthotic management and compared to sham LLLT with orthoses, no significant short-term differences between groups are observed. A similar pattern is seen with high-intensity laser therapy (HILT), with inconsistent findings and no clear additional benefit emerging.
Ultrasound
No recommendation could be made on ultrasound therapy for carpal tunnel syndrome treatment.
Contradictory and inconsistent evidence persists regarding the use of ultrasound in the management of carpal tunnel syndrome. One study reported that non-thermal ultrasound combined with an orthosis improved short-term pain compared to thermal or sham ultrasound. For functional outcomes, non-thermal ultrasound showed greater improvement in DASH scores at 4 weeks, whereas thermal ultrasound demonstrated superior results at 8 weeks. These variable and conflicting findings limit interpretability and suggest that ultrasound should not be routinely considered for carpal tunnel syndrome treatment.
Extracorporeal Shock Wave Therapy
Grade C: Clinicians may use extracorporeal shock wave therapy (ESWT) to achieve short- to mid-term (<6 months) improvements in symptoms and function in individuals with mild to moderate carpal tunnel syndrome managed nonsurgically, with consideration given to radial ESWT over focused ESWT.
The specific treatment parameters for ESWT remain unknown. This recommendation is based on two meta-analyses published between 2019 and 2026. However, the high heterogeneity of the included studies and the limitations of their included studies should foster caution when interpreting these results.
Transdermal drug delivery
Topical anti-inflammatory drugs, both steroidal and nonsteroidal, have been explored for carpal tunnel syndrome treatment using delivery methods such as iontophoresis (using electrical current), phonophoresis (US), and direct topical application, based on the condition’s inflammatory model.
Grade A: Clinicians should not use corticosteroid delivery via iontophoresis or phonophoresis for the nonsurgical management of carpal tunnel syndrome.
Grade C: Clinicians may use interferential current to achieve short-term pain relief in individuals with mild to moderate carpal tunnel syndrome managed nonsurgically.
Grade B: Clinicians should not use or recommend magnets for the management of carpal tunnel syndrome.
Thermotherapy
Grade C: Clinicians may recommend superficial heat to achieve short-term symptom relief in individuals with carpal tunnel syndrome managed nonsurgically.
Grade C: Clinicians may also consider microwave or shortwave diathermy for short-term symptom improvement in individuals with mild to moderate carpal tunnel syndrome managed nonsurgically.
The available evidence is of very low quality, with insufficient detail on treatment parameters and study designs that introduce a high risk of bias.
Dry needling
No recommendation could be made.
Only one study addressed this topic, reporting that a single session of dry needling targeting myofascial trigger points produced short-term pain reduction in individuals with moderate carpal tunnel syndrome. However, it remains unclear whether the observed improvement was specific to carpal tunnel symptoms or related to the treatment of myofascial trigger points.
Questions and thoughts
As highlighted by the clinical practice guidelines, no biophysical agents or traditional physiotherapy interventions (e.g., taping, manual therapy) demonstrate clear superiority over one another in the management of carpal tunnel syndrome. These approaches are often justified through different mechanisms—such as reducing inflammation, decreasing oedema, or modulating pain—yet they ultimately produce similar clinical effects. This raises an important question: are we targeting the right mechanisms?
If carpal tunnel syndrome were purely a mechanical compression problem, one would expect decompressive surgery to consistently outperform conservative care by reducing intracarpal pressure. However, observational data do not consistently support the superiority of surgery over physical therapy. This discrepancy suggests that our understanding of carpal tunnel syndrome pathophysiology may be incomplete.
The current model describes carpal tunnel syndrome as increased pressure within the carpal tunnel leading to nerve ischemia, intraneural oedema, and eventually fibrosis due to reduced perfusion. Yet several uncertainties remain: are these structural changes reversible, and to what extent do they actually drive symptoms? Emerging evidence points toward a more complex picture, including the role of central sensitization, which may help explain why symptoms can persist despite successful structural decompression.
In addition, systemic inflammation may contribute to the condition by increasing cytokines and growth factors, potentially promoting fibrotic changes within the nerve environment. This broader perspective challenges the strictly local, pathoanatomical view of carpal tunnel syndrome.
At the same time, advances in surgical techniques, particularly minimally invasive and ultrasound-guided procedures, may improve short-term outcomes by reducing tissue trauma and recovery time, addressing some of the limitations seen with traditional surgical approaches.
Talk nerdy to me
This Clinical Practice Guideline recommends a conservative management approach centered on patient education and wrist immobilization. Education should include identification and modification of aggravating factors. A forearm-based night orthosis maintaining the wrist in a neutral sagittal position is advised as a first-line intervention, with progression to daytime wear if nighttime use alone does not adequately relieve symptoms.
Adjunctive interventions such as manual therapy, biophysical agents, taping, and stretching may be incorporated; however, current evidence does not demonstrate clear superiority of one modality over another. As such, treatment selection should be guided by availability, as well as patient and clinician preference.
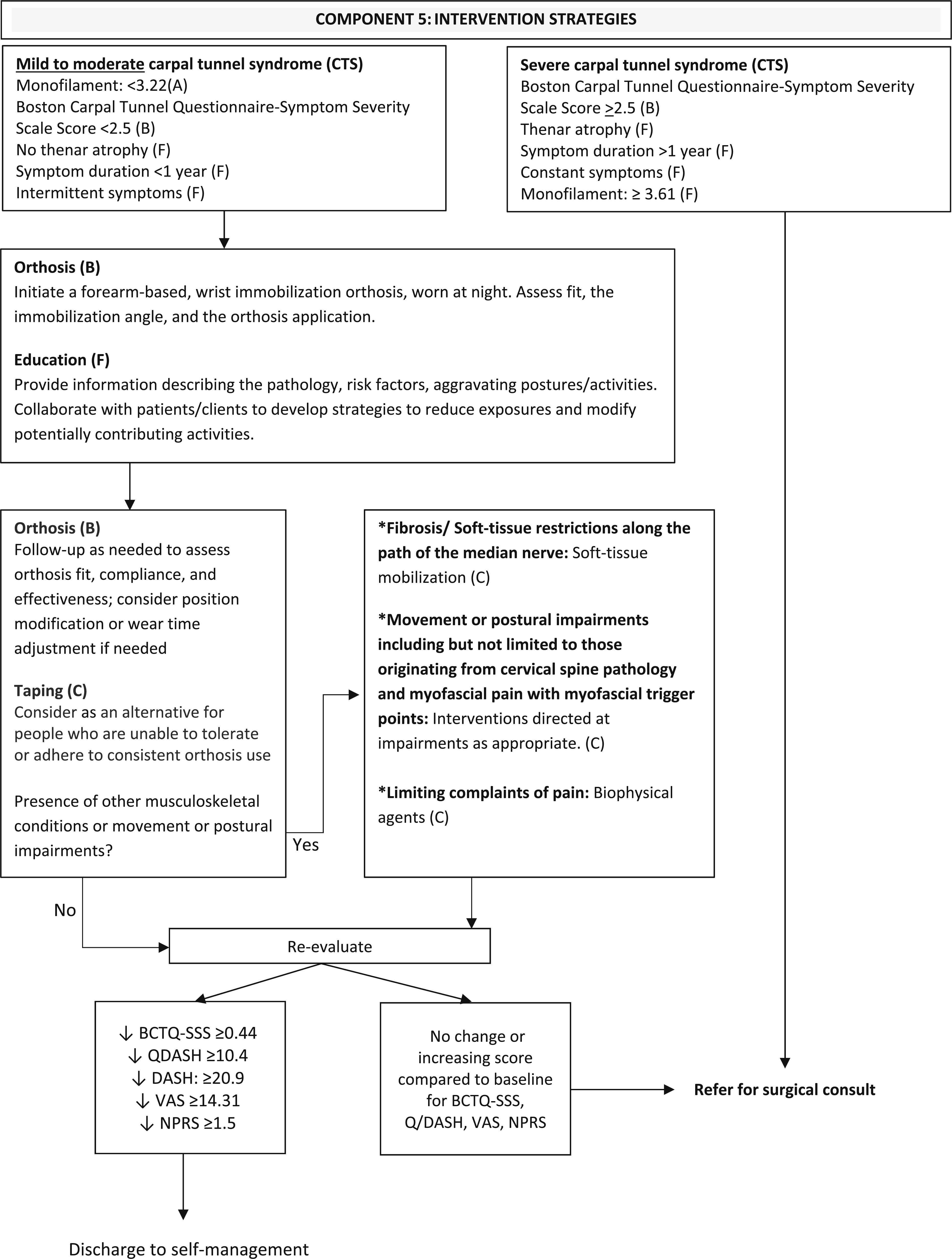
For individuals who do not demonstrate meaningful improvement based on validated clinical outcome measures, referral for surgical evaluation is recommended. The following decision tree can be used to guide clinical management.
Interestingly, no recommendations are provided regarding the role of psychosocial factors in the management of carpal tunnel syndrome. Although the authors acknowledge that psychosocial factors may be associated with greater pain severity, this dimension is not integrated into the treatment recommendations. As a result, the guidelines appear largely grounded in a pathoanatomical framework.
Moreover, given that no single intervention demonstrates clear superiority, many of the recommendations appear to be broad and non-specific. This contributes to the feeling that these are a “one size fits all” recommendation.
This may be inherent to the design of clinical practice guidelines. By synthesizing a wide range of data, often encompassing highly heterogeneous populations, this leads to recommendations that are broadly applicable but not necessarily tailored to specific patient groups. Moreover, the diagnosis of carpal tunnel syndrome itself likely encompasses a wide spectrum of presentations, including varying comorbidities, psychosocial influences, and other unmeasured or unknown contributing factors, further limiting the specificity of these recommendations.
Take-home messages
- Prioritize patient-reported outcomes: Tools like the BCTQ-SSS and QuickDASH are the most reliable for tracking symptom and functional changes. Strength and sensory tests are not valid for monitoring progress.
- Start simple: night orthosis + education: A neutral wrist night splint remains the cornerstone of conservative carpal tunnel syndrome treatment, with strong evidence for short- to mid-term symptom relief. Extend wear time if needed.
- Everything else is optional (and similar): Manual therapy, taping, exercise, laser, ESWT, and other modalities may provide short-term relief, but none clearly outperform others. Choose based on:
- Patient preference
- Availability
- Clinical reasoning
- Be cautious with modalities: Some interventions are not recommended (e.g., iontophoresis with corticosteroids, magnets), while others (e.g., ultrasound) show conflicting or insufficient evidence.
- Monitor outcomes and escalate when needed: If no meaningful improvement is seen, refer for surgical evaluation. Surgery is effective, but not always superior to conservative care.
Reference
DISCOVER FASCIA FROM ITS HISTORY TO ITS VARIOUS FUNCTIONS
Enjoy this free 3x 10min Video Series with Renowned Anatomist Karl Jacobs who will take you on a trip into the world of Fascia
